





Abstract
The present study aimed to assess whether arterial carbon dioxide pressure (Pa,CO2) has an impact on agreement between oxygen saturation measured with pulse oximetry (Sp,O2) or arterial blood gas co-oximetry (Sa,O2).
Sa,O2 and Sp,O2 determinations were obtained simultaneously from 846 patients under assessment for long-term home oxygen therapy in a specialised outpatient clinic. Both measurements were taken with patients seated and breathing room air.
Agreement between Sa,O2and Sp,O2results was analysed by the Bland–Altman method and the Lin concordance coefficient. In addition, potential interactions of arterial oxygen tension (Pa,O2) or Pa,CO2 on agreement were analysed by adjusted multivariate analysis.
Upon comparison of Sa,O2and Sp,O2 results, the Bland–Altman technique yielded a bias (95% confidence interval (CI)) of -1.24 (-6.86–4.38) and -1.32 (-7.78–5.15) when P</emph>a,CO2 >48 mmHg (6.39 kPa) or Pa,O2<54 mmHg (7.20 kPa), respectively. Estimate by Lin's coefficient (95% CI) in these cases was 0.88 (0.85–0.90) and 0.81 (0.77–0.85). Adjusted multivariate analysis, performed to assess the impact of pH, Pa,O2, Pa,CO2 and bicarbonate on bias, showed that Pa,O2, Pa,CO2 and their interaction terms were the most important predictors of the bias (standardised estimates of -0.54, -0.94, and 0.85, respectively). The effect of pH, although statistically significant, was small, and bicarbonate had no significant effect.
Arterial carbon dioxide pressure status can contribute to impaired agreement between arterial oxygen saturation and arterial oxygen saturation measured with pulse oximetry, particularly in patients with hypercapnia.
The use of pulse oximetry is one of the most important advances in respiratory monitoring and in the management of certain respiratory diseases 1. Nevertheless, there may be discrepancies between oxygen saturation measured with pulse oximetry (Sp,O2) and the actual status as calculated from arterial blood gas co-oximetry (Sa,O2). Sp,O2 can be elevated relative to Sa,O2when carboxyhaemoglobin levels are high, and in the presence of intravascular dyes, dark skin pigmentation, motion artefacts, nail polishes, optical shunting or poor peripheral perfusion 2–4. In contrast, lower Sp,O2 values can be produced when there is: an abnormal haemoglobin variant; methaemoglobinaemia; sulfhaemoglobinaemia; prominent venous pulsations; or contamination of measurement by ambient light, as well as intravenous dyes and nail polish 5.
Several studies have demonstrated that the majority of pulse oximetry readings correlate well with Sa,O2 when none of the aforementioned factors is present and Sp,O2 is 84–96% 6, and quite well when Sp,O2 is >70% 7. Most of these studies have been done in hospitalised patients, generally in intensive care units, or in healthy individuals who are exposed to various conditions of hypoxia. Very few studies have examined the agreement between Sa,O2 and Sp,O2 in the setting of outpatient monitoring 8–10, an area in which this information can be highly relevant. With the development of long-term home oxygen therapy and home mechanical ventilation, clinicians attend an increasingly greater number of patients with end-stage lung disease in whom the decisions regarding these and other therapies are often based on pulse oximetry findings 11–14.
Many patients with end-stage lung disease have chronic respiratory failure and present elevated arterial carbon dioxide pressure (Pa,CO2) 15. Currently, there are no studies that determine whether blood CO2 alterations can result in discrepancies between Sa,O2and Sp,O2 results and very few have analysed agreement between Sa,O2and Sp,O2 in patients with Sp,O-2 <70% 16, a frequent situation in this population 11–13. The main aim of the present study was to determine whether altered blood CO2 levels can change the existing relationship between Sa,O2 and Sp,O2. In addition, it was assessed whether Sp,O2 could provide a valid estimate of Sa,O2at very low levels of hypoxaemia in a large number of samples from patients with various respiratory diseases.
MATERIAL AND METHODS
Materials
The present study was performed from Sa,O2 and Sp,O2 determinations obtained simultaneously from 846 patients under assessment for long-term home oxygen therapy in a specialised outpatient centre. The population included all patients who underwent arterial blood gas measurement and Sp,O2 determination between January 1995 and December 2004. A total of 216 patients were excluded for the following reasons: one of the two determinations could not be performed; the patient presented factors that could result in false Sa,O2or Sp,O2results (e.g. active smoking at the time of the determination, carboxyhaemoglobin levels >2%, abnormal haemoglobin variants, presence of i.v. dyes, use of blue nail polish or prominent venous pulsations); or Sp,O2 changes were observed during puncture for blood gas measurement.
The characteristics of the patients studied are summarised in table 1⇓. All were Caucasian and none had scleroderma or Raynaud phenomenon. Among the total, 570 (67.4%) patients were receiving oxygen at home at the time they were assessed.
Baseline characteristics of patients included in the study
Methods
Measurement of arterial oxygen saturation by co-oximetry
Room air arterial blood gas sampling was performed according to the Spanish Society of Pulmonology and Thoracic Surgery guidelines 17. Briefly, samples were anaerobically drawn into 5-mL pre-heparinised syringes following administration of local anaesthesia in the area of the radial artery. Air bubbles were removed from the syringes and each sample was immediately taken for analysis. Arterial blood was analysed using an IL 682 co-oximeter (Instrumentation Laboratories, Lexington, MA, USA). Sa,O2 was determined with the following formula in which FO2Hb is the oxyhaemoglobin fraction, FCOHb is the carboxyhaemoglobin fraction, and FmetHb is the methaemoglobin fraction.
Sa,O2 = 100×(FO2Hb/100)–(FCOHb+FmetHb) (1)
Carboxyhaemoglobin and methaemoglobin values were also systematically recorded in all the determinations carried out.
Measurement of arterial oxygen saturation by pulse oximetry
Arterial oxygen saturation was measured with Minolta pulse oximeters (Pulsox-7; Minolta Company Ltd, Milton Keynes, UK). The measurement was taken with a digit sensor, and great care was taken to ensure that the test person's fingers were warm during the process. Measurements were performed when the subject was awake, had not exercised, and had been sitting for ≥10 min in the same position, and after an interval of ≥1.5 h since the last meal. It took 1–3 min for the measured Sp,O2value on the display to remain constant for >15 s. This value was taken as Sp,O2 at rest. In some patients, particularly those with severe hypoxaemia, saturation never fully stabilised. In these cases, the investigator measured continuously for ∼2 min, with all values being recorded in the pulse oximeter's memory. The minimum and maximum values were noted and the value appearing most frequently in the 2-min recording (i.e. the predominant value) was taken for the analysis, as has been described previously 18.
Statistical analysis
To investigate concordance between the two methods for estimating oxygen saturation, pulse oximetry and co-oximetry (the reference method), the mean of both methods was plotted against the difference (bias = Sa,O2–Sp,O2), according to the Bland–Altman recommendations 19, 20. The Bland–Altman 95% limits of agreement (mean bias±2sd) procedure uses datascale assessment to analyse the accuracy (i.e. bias) and the amount of variation, or precision, between any two measured values when the range of data is sufficiently limited.
Lin's concordance coefficient (LCC) and the corresponding 95% confidence interval were also used to determine the agreement between the two methods 21–23. The LCC measures of both precision and accuracy to determine whether the observed data deviate significantly from the line of perfect concordance, which occurs at 45 degrees; that is, it assesses the linear relationship between two variables under the constraint that the intercept is zero and the slope is one. The value of LCC increases as the accuracy and precision of the observed data improve.
In order to evaluate the impact of arterial oxygen tension (Pa,O2) and Pa,CO2on the measurements obtained by the two methods, the determinations were categorised by tertiles. To assess the combined effect of both these variables, the cut-off points used were the median for Pa,O2 and tertiles for Pa,CO2, resulting in six groups being available for the analysis.
Multivariate regression analysis was carried out to assess the repercussions of pH, Pa,O2, Pa,CO2, and bicarbonate on the bias. Standardised coefficients were used to rule out the adjusted influence of these variables concomitantly.
Significance was defined as a two-tailed p-value of <0.05.
RESULTS
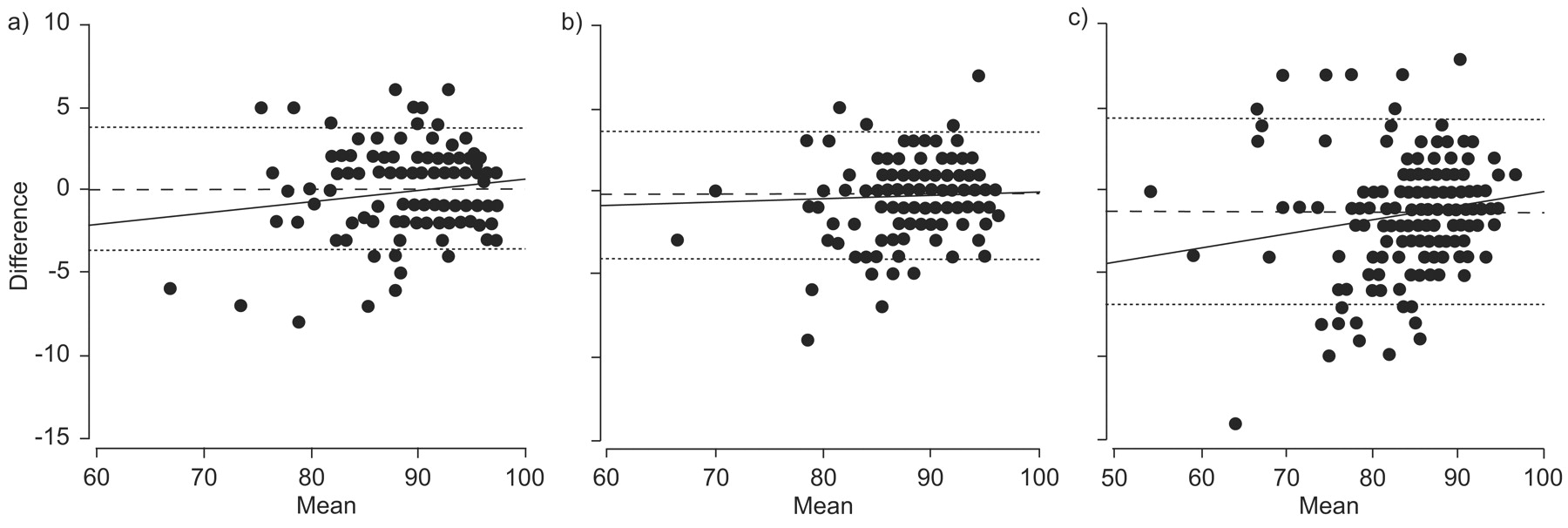
The variables analysed are summarised in table 2⇓. Cut-off values for Pa,O2and Pa,CO2 were as follows: tertiles for Pa,O2of 54 mmHg (7.19 kPa) and 62 mmHg (8.26 kPa); tertiles for Pa,CO2of 41.9 mmHg (5.59 kPa) and 48 mmHg (6.40 kPa); and median Pa,O258 mmHg (7.73 kPa). The differences between pulse oximetry and co-oximetry results plotted against the average of the two according to the grade of hypoxaemia (Bland–Altman method) are shown in figure 1⇓.

Difference versus mean of test and standard measurements, with mean bias (– – – – –) 95% limits of agreements (· · · · ·) and regression line (–––––) by level of arterial oxygen tension, a) first tertile; b) second tertile; c) third tertile.
Bias, agreement and concordance for estimation of oxygen saturation comparing pulse oximeter and co-oximeter results
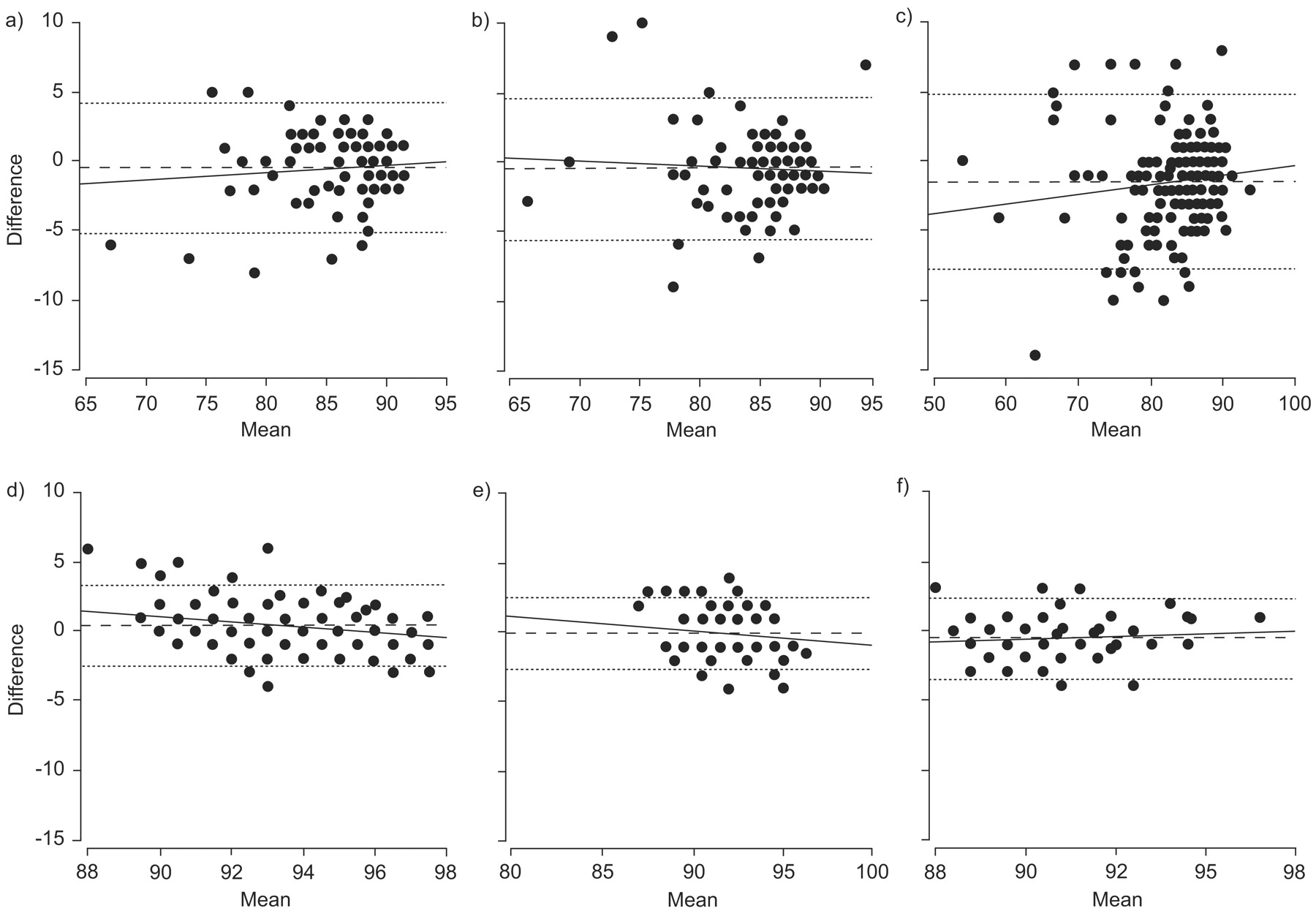
Agreement between Sa,O2and Sp,O2 was poorer for lower values of Pa,O2and for higher values of Pa,CO2. The differences by Pa,CO2level are shown in figure 2⇓: the degree of agreement becomes progressively lower as Pa,CO2increases. Analysis of Pa,O2and Pa,CO2values together disclosed poorer agreement in hypoxic patients with increased Pa,CO2 (table 2⇑ and fig 3⇓). The analysis performed using the LCC method estimated overall concordance at 0.91, with the estimates ranging from 0.63 (second Pa,O2tertile) to 0.92 (first PaCO2tertile).

Difference against mean of test and standard measurements, with mean bias (– – – – –) 95% limits of agreements (· · · · ·) and regression line (–––––) by level of arterial carbon dioxide pressure; a) first tertile; b) second tertile; c) third tertile.

{kind=link}
{kind=link}
{kind=link}
Difference versus mean of test and standard measurements, with mean bias (– – – – –), 95% limits of agreements (· · · · ·) and regression line (–––––) for levels of arterial oxygen tension (Pa,O2) and arterial carbon dioxide pressure (PaCO2) a) median or less Pa,O2 and first tertile of PaCO2; b) median or less Pa,O2 and second tertile of PaCO2; c) median or less Pa,O2 and third tertile of PaCO2; d) more than the median Pa,O2 and first tertile of PaCO2; e) more than the median Pa,O2 and second tertile of PaCO2; f) more than the median Pa,O2 and third tertile of PaCO2.
The results of the adjusted multivariate analysis, performed to assess the impact of the different factors on the bias (table 3⇓), indicate that Pa,O2, PaCO2 and their interaction term were the most important predictors (standardised estimates of -0.54, -0.94 and 0.85, respectively). The effect of pH was small, although statistically significant, and bicarbonate had no significant effect.
Multivariate regression to assess the influence of pH, arterial oxygen tension(Pa,O2), carbon dioxide arterial tension (Pa,CO2)and bicarbonate on the oxygen saturation bias, i.e. difference between pulse oximeter and co-oximeter measurements (arterial oxygen saturation minus arterial oxygen saturation measured by pulse oximetry)
DISCUSSION
The main finding emerging from the present study is that Pa,CO2levels can affect the accuracy and reliability of Sp,O2measurements. Agreement between Sa,O2and Sp,O2decreases as Pa,CO2 increases, regardless of the grade of associated hypoxaemia. Moreover, in a large series of determinations, the present study also confirmed that Sp,O2 correlates poorly with Sa,O2when Pa,O2is low, particularly when it is <54 mmHg (7.20 kPa).
To the current authors knowledge, the possibility that alterations in blood carbon dioxide levels might affect concordance between Sa,O2and Sp,O2measurements has not been specifically investigated. The only closely related study is by Lee et al. 8, who assessed the accuracy of pulse oximetry in 664 determinations in the emergency department. Following an analysis of several variables including age, sex and levels of haemoglobin, bicarbonate, pH, Pa,O2, Pa,CO2, and carboxyhaemoglobin, Lee et al. 8 concluded that the only variable affecting agreement between Sa,O2and Sp,O2 was carboxyhaemoglobin level. In the analysis, however, the authors categorised the oxygen saturation results of the two methods instead of performing direct assessment with LCC and the Bland–Altman approach, as was carried out in the present study. Moreover, including a variable in the analysis that is recognised as having an effect on Sa,O2and Sp,O2agreement, namely carboxyhaemoglobin level 24, could have masked the effect of other variables, such as Pa,CO2. In patients with normal carboxyhaemoglobin the present study found that, Pa,CO2levels can alter agreement between the two determinations and that the magnitude of this effect was greater for Pa,CO2 than for Pa,O2, the interaction between Pa,O2and Pa,CO2, bicarbonate, or pH. It is also important to note that in the present study, Sa,O2 measurements were adjusted for carboxyhaemoglobin and methaemoglobin; therefore, the results presented are likely to underestimate the overmeasurement bias occurring in the clinical setting, and may account for the apparently smaller bias seen here than in other comparisons.
The mechanism by which abnormal blood carbon dioxide levels can affect the agreement between Sa,O2and Sp,O2measurements is unknown. Pulse oximetry provides instantaneous, in vivo determination of oxygen saturation by measuring arterial blood light absorption at two specific wavelengths, 660 nm (red) and 940 nm (infrared), to distinguish between deoxygenated and oxygenated haemoglobin, whereas co-oximetry uses at least four different wavelengths of light for arterial blood gas analysis. In normal conditions, ∼5% of carbon dioxide in arterial blood and 30% in venous blood transported in a haemoglobin-bound form, as carbaminohaemoglobin 25. It is reasonable to hypothesise that the presence of elevated Pa,CO2levels can alter the wavelength reading of the pulse oximeter because of increases in the amount of carbaminohaemoglobin, as occurs with carboxyhaemoglobin when carbon monoxide levels are elevated 24, or because of an increase in red blood cell osmolarity, which can induce changes in cell morphology 25. Another possible explanation might be that the venous blood pulsatility index is larger in the context of a vasodilated dynamic circulation, owing to an increase in the Pa,CO2.
The present findings indicate that the lack of agreement between Sa,O2and Sp,O2in relation to carbon dioxide levels may be clinically relevant. The individuals studied were referred to the study centre to undergo assessment for home oxygen therapy. Some authors have proposed 11–13 that these patients can be evaluated by pulse oximetry alone, without the need for arterial blood gas analysis. Nevertheless, 59% of the patients in the present study had high Pa,CO2levels, which we have shown can lead to overestimation of Sa,O2. On the basis of these results, the physician might not prescribe oxygen for these patients, or prescribe an inadequate flow.
Another situation that is becoming increasingly more common in daily clinical practice is assessment of patients who might benefit from noninvasive home mechanical ventilation (NIHMV). Some authors have suggested that adaptation to NIHMV can be performed according to the response observed on pulse oximetry 14, 26. Considering that nearly all the patients who receive this treatment have high Pa,CO2 levels, the overestimation of Sa,O2 produced when there is severe hypercapnia might lead to a suboptimal choice of ventilation parameters.
In the present study patients with hypoxaemia, a decrease in Pa,CO2to levels below the first tertile (Pa,CO2<42 mmHg (5.60 kPa)) also affected agreement between Sa,O2and Sp,O2. Under these conditions, Sp,O2underestimates Sa,O2, although the magnitude of the discrepancy is smaller than when Pa,CO2levels are elevated. This fact may be relevant in clinical situations of hyperventilation, as occurs in patients with pulmonary thromboembolism or pulmonary hypertension, or when assessing adaptation to hypobaric hypoxia in the process of acclimatisation to high altitudes 27–31.
The present study also showed that Sp,O2correlates poorly with Sa,O2when Pa,O2 is low. These findings are similar to reported results demonstrating that most pulse oximeters are accurate to ±4% in normal patients when Sa,O2is >70% 6–7, 32–34. The additional value of the present data is that it was obtained in a large number of determinations from patients with various respiratory pathologies attended on an outpatient basis. Moreover, in contrast to previous studies, it was possible to examine a large series of samples from patients with very low Pa,O2, in whom agreement was particularly poor.
The present results were obtained in outpatients with stable respiratory disease. This fact might be considered a limitation of the study because the effect of acute Pa,CO2 changes in parallel with the pH were not evaluated. In this regard, some authors have suggested that acidosis might result in poorer agreement between Sa,O2and Sp,O235, whereas a recent study did not confirm this possibility 36. Moreover, Sp,O2 is generally higher in the outpatient population than in intensive care patients and most hospitalised patients. In the hospital setting the effect of altered Pa,CO2and low Sa,O2may be more pronounced. Another limitation of the study is the fact that the pulse oximeters used were all the same model. Oximeters from different manufacturers show small differences related to the algorithms used to determine Sp,O2from the raw measurements of red and infrared light transmitted through the tissues. These differences were greater in the early days of oximetry than they are now because the current technical characteristics and performance of the majority of pulse oximeters are quite similar 6, 7, 32–34, 37 and all will be equally affected by the various factors known to alter the accuracy of Sa,O2measurements. Although the effect of Pa,CO2on the accuracy of these devices has not been systematically assessed, it is likely that the present findings can be generalised to other models. Lastly, it cannot be excluded that elevated levels of Pa,CO2 might also affect the co-oximetry readings, although in the literature no data encountered support this idea.
In conclusion, in a heterogeneous group of patients with advanced respiratory disease, the present authors report that carbon dioxide arterial tension status can impair the agreement between arterial oxygen saturation and arterial oxygen saturation measured by pulse oximetry, particularly in patients with hypercapnia. In addition, the present results in a large number of paired samples show that agreement between arterial oxygen saturation and arterial oxygen saturation measure by pulse oximetry worsens as hypoxaemia values decrease. Therefore, it is likely that arterial oxygen saturation measured by oximetry may not be sufficiently accurate when assessing patients for long-term home oxygen therapy and should not substitute the gold standard arterial oxygen tension measured in arterial blood.
Statement of interest
None declared.
- Received September 25, 2007.
- Accepted April 29, 2008.
- © ERS Journals Ltd
References










