





Abstract
Increased frequency of microsatellite DNA instability (MSI) has been detected in the sputum of chronic obstructive pulmonary disease (COPD) patients. The aim of the present study was to investigate the relationship between MSI in sputum cells and exacerbation frequency, which is an important parameter in the clinical course of the disease.
Induced sputum samples and peripheral blood obtained from 36 patients with COPD at stable state were analysed. The control group consisted of 30 nonsmoking healthy subjects. DNA was extracted and analysed for MSI using the following microsatellite markers: RH70958, D5S207, D6S2223, D6S344, D6S263, G29802, D13S71, D14S588, D14S292 and D17S250. Following MSI analysis, exacerbations were recorded for 3 yrs in total.
No MSI was detected in healthy nonsmokers. A total of 18 (50%) out of 36 patients exhibited MSI in their sputum cells. Patients who exhibited MSI showed significantly increased frequency of exacerbations compared with patients that did not. In addition, a significantly increased frequency of purulent and of severe type exacerbations was found in patients exhibiting MSI. Patients positive for marker G29802, D13S71 or D14S588 presented increased exacerbation frequency.
The significant association between microsatellite DNA instability and chronic obstructive pulmonary disease exacerbations indicates that somatic mutations could be involved in the pathogenesis and natural history of the disease.
The course of chronic obstructive pulmonary disease (COPD) is characterised by exacerbations that induce inflammation and aggravate oxidative stress in the lungs leading to further physiological deterioration 1, 2. Notably, some COPD patients present the frequent exacerbation phenotype of the disease. The severity of the disease and the number of exacerbations in previous years have been associated with an increased exacerbation frequency 3, 4. However, it is not known whether exacerbation frequency is associated with genetic alterations or whether there is a genetic susceptibility for frequent exacerbations, despite the fact that previous studies have led to the identification of several genes that are probably involved in COPD pathogenesis 5, 6.
In previous investigations, the current authors reported that COPD patients present a high frequency of genetic alterations at the microsatellite DNA level, which are detected in their sputum cells 7, 8. Microsatellite DNA consists of very short tandem nucleotide repeats that are found scattered throughout the human genomes of eukaryotes 9–12. Insertion or deletion of these DNA sequences (microsatellite DNA instability (MSI)) has been correlated with a high somatic mutation rate and is associated with a defective DNA mismatch repair (MMR) system 13, 14. Thus, MSI detection in sputum cells of COPD patients could be a useful marker, indicating destabilisation of the genome at various loci.
In this respect, it was investigated whether there is a relationship between somatic genetic alterations and exacerbation frequency in COPD and, therefore, whether patients who exhibit MSI in their sputum cells present an increased exacerbation frequency compared with patients exhibiting no MSI.
METHODS
Subjects and protocol
A total of 66 subjects were studied. Baseline characteristics of 36 COPD patients are shown in table 1⇓. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) Consensus Statement was used for the diagnosis of COPD 15. The control group consisted of 30 healthy nonsmoking subjects (mean±sd age 56±17 yrs), with forced expiratory volume in one second (FEV1) 92±4% predicted, forced volume capacity (FVC) 88±4% pred and FEV1/FVC 83±8%. Patients were recruited by consecutive sampling from a cohort of a longitudinal study of lung function decline in COPD 3. Patients with asthma, an upper or lower respiratory tract infection within the last 4 weeks before the study, and a history of any cancer, were excluded from this study.
Baseline characteristics of 36 chronic obstructive pulmonary disease(COPD) patients by smoking status
The present investigation was a 3-year prospective study, incorporating a run-in period of 4 weeks, sputum induction and clinical assessment at baseline 15–17 and outpatient clinic visits, scheduled every 3 months. At baseline, patients underwent sputum induction at steady condition, sputum was cultured for bacteria and differential sputum cell count was estimated, and sputum and blood were examined for MSI. All 36 patients were then provided with diary cards to record changes in symptoms (dyspnoea, sputum production and purulence (major symptoms); and wheeze, cough, nasal discharge, sore throat and fever (minor symptoms)). A patient-directed diary card and clinical records were used to identify and assign exacerbations. A protocol-based on GOLD was used for individual exacerbation treatment 15. The study was approved by medical research ethics committees of the University of Crete, the University Hospital of Heraklion (Heraklion) and the Chania General Hospital (Chania, Greece) and the patients gave their informed consent.
Exacerbations
The definition of an exacerbation was based on previously described criteria 4, 16 requiring either an increase of at least two major respiratory symptoms (dyspnoea, sputum amount and sputum purulence) or an increase of one major symptom in addition to at least one minor symptom (wheeze, cough, fever, nasal discharge or sore throat), for at least two consecutive days. The first day with increased symptoms was taken as the onset of the exacerbation. Following an exacerbation, patients were required to have a 2-week period (recovery period) with the same or a reduction of symptoms as those present before the start of an exacerbation, before another exacerbation was studied.
Monitoring of exacerbation
Diary card
The development of the diary card was based on a previously used diary card 3. All patients were instructed to record, at the end of each day, any increase in symptoms during the previous 24 h. Changes in symptoms were registered using a binary-coded system. Patients were seen in scheduled visits as outpatients every 3 months and diary cards were collected. Exacerbations identified from diary cards were termed “diary card recorded exacerbations”.
Medical records
Exacerbations when no diary card symptoms were recorded were identified either by questioning the patients about symptoms during clinical visits or on admission to hospital, or by a review of hospital medical records. Exacerbations identified in this way were termed “medical records identified exacerbations”.
Exacerbation rate
The total number of exacerbations was obtained by combining the number of diary-card recorded exacerbations plus the number of medical records identified exacerbations. The total annual rate for each patient was calculated by dividing the total number of exacerbations by the number of days participated in the study and then multiplying by 365.
Sputum induction
Sputum was induced via inhalation of a hypertonic saline solution aerosol, generated by an ultrasonic nebuliser (Ultraneb 2000; DeVilbiss, Somerset, PA, USA). A previously described procedure was followed for sputum induction, processing, and total and differential cell counting 8.
DNA extraction from sputum and blood cells
The presence of MSI in sputum cells in comparison with DNA obtained from peripheral white blood cells from the same individual was investigated. DNA extraction was carried out (Qiagen Extraction Kits, QIAmp DNA Blood Maxi and Mini Kits; QIAGEN Inc., Valencia, CA, USA) and DNA samples were stored at -20°C.
Microsatellite markers and MSI analysis
A total of 10 polymorphic microsatellite markers were used to assess MSI (RH70958, D5S207, D6S2223, D6S344, D6S263, G29802, D13S71, D14S588, D14S292 and D17S250; table 2⇓). These markers were chosen as they are located closely to genes that are thought to be related to COPD pathogenesis 6–8. The sequences of the microsatellite markers used were provided through the National Center for Biotechnology Information Database. The PCR technique was used to amplify DNA sequences. PCR amplifications were carried out in 50 µL final volume reaction mixtures in a PTC-100 thermal cycler (M.J. Research Inc, Watertown, MA, USA), using the Qiagen Taq PCR Core Kit (QIAGEN Inc.). Forward primers were labelled with the Licor IR800 fluorochrome. The following thermal cycling protocol was applied: 3 min at 94°C, 30 cycles at 94°C for 30 s, 55°C for 30 s, 72°C for 30 s, 72°C for 5 min and termination at 40°C. The PCR products were analysed and visualised by electrophoresis in 8% Long Ranger polyacrylamide (BMA, Rockland, ME, USA) 7 M urea sequencing gels in a Licor 4200 DNA sequencer (Li-Cor Inc, Lincoln, NE, USA) and alleles were sized with GeneProfiler version 3.54 software (Scanalytics, Rockville, MD, USA). MSI was identified by comparing the electrophoretic patterns of the microsatellite markers of DNA of sputum versus peripheral blood demonstrating a shift of one or both of the alleles, thus generating novel alleles as indicated by an addition or deletion of one or more repeat units. Figure 1⇓ shows representative sample of microsatellite DNA stability, as well as MSI, in the microsatellite marker D6S344. Two scientists who were not aware of the clinical characteristics of the subjects performed independent readings. All MSI-positive samples were tested twice using fresh DNA, showing 100% reproducibility.
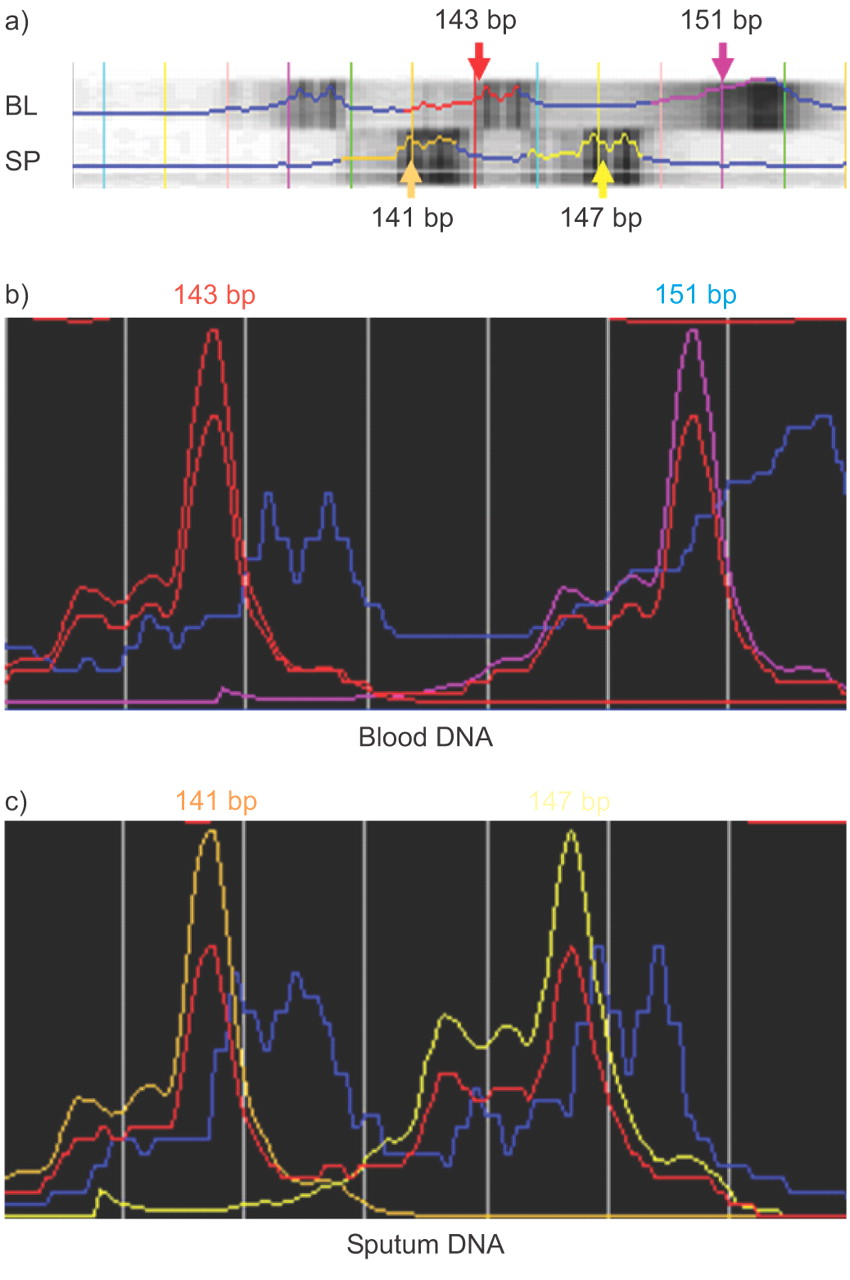
Representative sample of microsatellite DNA Instability (MSI), in the marker D6S344, analysed with LI-COR Saga GT Microsatellite Analysis Software (Version 3.2; LI-COR, Inc., Lincoln, NE, USA). The expected PCR product size for the locus D6S344 is 139–159 bp (NCBI UniSTS:36924). Hereby, the software is given the range between which the product is expected (139–159 bp); starting from 139 bp the program puts coloured lines every 2 bp, providing the exact size of each allele. The figure shows a microsatellite instability, where each allele is characterised according to its size. The blood DNA sample shows one allele in 143 bp as red (together with its corresponding peak) and the other in 151 bp as pink. In contrast, the sputum DNA sample is translocated, clearly showing the instability: the first allele is in 141 bp (coloured dark yellow) and the second in 147 bp (bright yellow). The greater the peaks are, the more amplified the sequence is. Lower peaks (blue line) only show by-products of the reaction. BL: DNA specimen obtained from peripheral blood; SP: DNA specimen obtained from sputum.
Cases exhibiting microsatellite DNA instability(MSI) according to each marker, the corresponding chromosomal location and related gene
Statistical analysis
Normality of the numerical parameters was tested using the Kolmogorov–Smirnov test. Unpaired t-test for normally distributed data and the Mann–Whitney test for data not normally distributed were used to estimate significant differences among the groups. Chi-squared test was used for comparison of percentages. A p-value of <0.05 was considered statistically significant.
RESULTS
Exacerbations
Table 3⇓ shows the overall number of exacerbation in the 3-yr period. The participants were followed for median (range) 1095 (760–1095) days and recorded their symptoms on the cards for 745 (490–1095) days. The types of exacerbations are presented in table 3⇓. More than 50% of the exacerbations were characterised as purulent. A total of 48 (15.4%) exacerbations required hospitalisation, which occurred at the same hospital in 46 cases. The mean (95% confidence interval) annual rate of admissions due to exacerbations was 0.44 (0.2–0.68). Patients (n = 10) with bacterial colonisation at baseline had significantly higher median (interquartile range (IQR)) 3-yr annual exacerbation rate than patients (n = 26) without evidence of colonisation (4.4 (2.3–5.3) versus 2.6 (1.3–3.3); p = 0.01).
Exacerbation number and annual rates in all 36 chronic obstructive pulmonary disease patients during the study period
MSI
Out of a total of 36 COPD patients, 18 (50%) exhibited MSI in their sputum cells (MSI+ subjects). All healthy subjects showed no MSI in any of the 10 microsatellite markers tested.
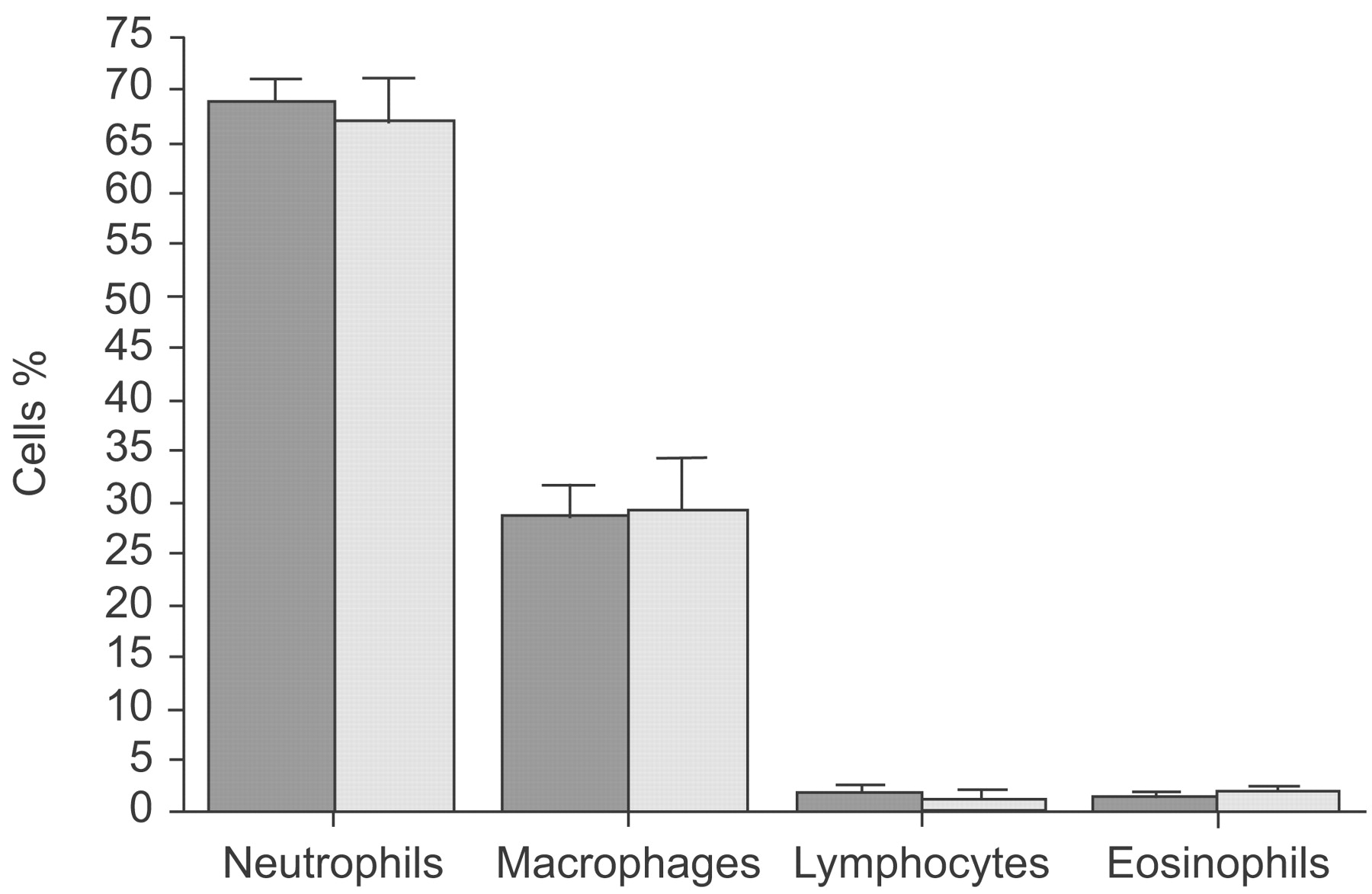
Subject characteristics were then compared according to the presence of MSI or not (table 4⇓). No statistically significant differences were found in the anthropometric clinical data, including chronic bronchial colonisation between the two groups (table 4⇓). In addition, the median (IQR) number of days between sputum induction and last exacerbation was not significantly different between MSI+ and MSI- subjects (60 (45–137) versus 60 (45–120) days, respectively; p = 0.4). The degree of airway inflammation in stable disease state was not different between the two groups in terms of inflammatory cell profile (fig. 2⇓). No statistically significant relationship was found between FEV1% pred and MSI frequency.

Sputum differential cell counts in COPD patients with positive (▒) and negative (░) microsatellite DNA instability markers. Data are presented as median (interquartile range).
Baseline characteristics of chronic obstructive pulmonary disease patients according to microsatellite DNA instability(MSI) status
Table 2⇑ also shows that MSI was detected in more than one marker in the same individual (33 MSI in 18 patients). The most frequently affected markers were D13S71 and G29802 (positive in eight and seven subjects, respectively).
The relationship between MSI and exacerbations
Figure 3⇓ shows that patients who exhibited MSI experienced a significantly higher number of exacerbations compared with patients who did not present MSI (p = 0.003). When exacerbations were analysed according to sputum quality/severity, a significant increased number of purulent (p = 0.002) and type-I exacerbations was found in patients who exhibited MSI compared with patients who did not (p = 0.001).

Individual annual exacerbation rates of chronic obstructive pulmonary disease patients with positive (n = 18; •) and negative (n = 18; ○) microsatellite DNA instability (MSI) markers, overall and according to sputum purulence and severity (type-I, -II and -III exacerbations). Horizontal lines represent median values. #: p = 0.003; ¶: p = 0.002; +: p = 0.001; §: nonsignificant.
Patients who were positive for MSI markers G29802, D13S71 or D6S344 had relatively higher overall exacerbation rates compared with patients who did not exhibit MSI (fig. 4⇓). When exacerbations were analysed by severity, type-I exacerbations rates were found to be significantly higher in patients positive either to marker G29802 (p = 0.004) or D13S71 (p = 0.007), compared with patients who did not exhibit MSI.

Individual annual exacerbation rates of chronic obstructive pulmonary disease patients according to the presence of different microsatellite DNA instability (MSI) markers in their sputum. Horizontal lines represent median values. **: p<0.01.
DISCUSSION
The purpose of the present prospective study was to investigate the relationship between somatic genetic alterations and exacerbation frequency in COPD patients. In agreement with the current authors’ previous investigations 7, 8, 18, a significant proportion (50%) of COPD patients in the present study exhibited MSI in markers which are located closely to genes encoding for proteins possibly related to COPD pathogenesis. Moreover, six (33%) out of 18 subjects showed MSI in more than one marker (table 2⇑). The novel finding in the present study is the significant association between MSI incidence and frequency of exacerbations. COPD patients positive for MSI were found to have a significantly higher overall exacerbation frequency than patients with no microsatellite instability; this was particularly true for more complex (type-I) and for purulent exacerbations. In addition, analysing MSI for each marker separately, patients who exhibited MSI in the chromosomal region related to genes encoding either tumour necrosis factor, serpines, (protease inhibitor (PI)6, and PI9) or perforin experienced significantly higher number of overall exacerbations compared with patients who did not exhibit MSI (fig. 4⇑).
Despite the fact that sputum is a relatively heterogeneous sample to consider and the fact that it is not yet known which cell subpopulation is responsible for MSI, previous studies by the current authors have provided evidence suggesting that the detection of MSI in sputum may be of importance in COPD. First, COPD patients presented sputum MSI in different chromosomal regions compared with sputum from asthmatics 8. Secondly, MSI was found in sputum but not in nasal cytological samples of COPD patients, despite the fact that inflammation coexists in the nasal mucosa of these patients 18. The latter suggests that MSI in the markers studied is a specific finding for the target organ of COPD, i.e. the lungs. Thus, MSI detection in COPD raises the questions of when and how acquired somatic mutations at the microsatellite level occurring during the course of COPD play a role in the pathogenesis or in the natural course of the disease. However, the precise role of MSI detection in COPD has not yet been established.
MSI is seen in chronically inflamed tissues 19. It has been suggested that oxidative stress can modify the inflammatory response and can inactivate the human DNA MMR system in a dose-dependent manner 20. Thus, MSI can clearly be subject to a secondary change related to airway inflammation and increased oxidative stress, which characterise COPD. In this respect, the current authors assessed the relationship between MSI and COPD exacerbations, which augment further airway inflammation and oxidative stress compared with stable state 21–23. Remarkably, it was found that patients who exhibited MSI in their sputum experienced a significantly higher number of exacerbations (fig. 3⇑). This was true particularly for exacerbations categorised clinically as more complex or purulent. On this basis, it is tempting to hypothesise that repetitive stimulation by frequent exacerbations aggravates inflammation and oxidative stress in the airways and leads to an altered DNA repair process and therefore to an increased detection of genetic alterations at the microsatellite level.
One might argue that MSI may represent insult from other factors which are not related to exacerbations per se. It cannot be excluded that other environmental or clinical factors may result in MSI. However, the population studied represented mainly COPD patients followed at a specialist hospital clinic and it was in many terms homogenous (white, Greeks, inhabitants of an island). Thus, it can be assumed that all of the subjects were affected by the same environmental factors. In addition, on comparing subgroups of COPD patients that were respectively positive and negative for MSI (table 4⇑), no statistically significant difference was found in relation to age, duration of illness, baseline treatment (including steroids), bacterial colonisation, smoking status and spirometric indices. Therefore, despite the fact that the association between MSI and exacerbation frequency complexity does not prove a causal relationship, the present results deserve consideration. The current findings suggest that there is a potential relationship between an increased frequency of exacerbations and somatic acquired mutations at the microsatellite DNA level that might be considered in the investigation of the pathogenesis of the disease. A longitudinal investigation of MSI, using markers especially related to oxidative stress (i.e. haemoxygenase), before and after a long follow-up for exacerbation monitoring will potentially provide further information for the relationship between MSI, oxidative stress and exacerbations.
An alternative explanation for the relationship between MSI and exacerbations could be that MSI indicates predisposition to frequent exacerbations. MSIs may represent dysfunctional changes in genes directly causing increased exacerbations (i.e. within causal genes), or they may be in linkage disequilibrium with nearby causal genes. From this perspective, host response to environmental insult (viruses and bacteria) may be impaired, and some COPD patients may experience frequent exacerbations, at least in part owing to molecular deregulations of host defences 24, 25. Notably, clusters of smoking-induced somatic mutations has been previously reported in genes related to nuclear factor-κB and activator protein-1 activation, which coordinate the expression of a plethora of inflammatory mediators 26, 27. This alternative hypothesis is also supported by previous studies reporting that patients who presented frequent exacerbations were those who had increased exacerbation rates in previous years 4. In addition, although advanced disease may be a significant parameter of increased exacerbation rate, not all patients with severe COPD are prone to frequent exacerbations 28. Thus, genetic predisposition for increased exacerbation frequency is not unlikely.
Furthermore, it maybe speculated that since MSI indicates a defective DNA MMR system, its presence might be also associated with a mechanism that inhibits the resolution of the inflammation after exacerbation. Thus, these mutations might contribute to the pathogenesis of airway inflammation that is observed in stable COPD and consequently to an increased exacerbation frequency. Notably, frequent exacerbators have increased airway inflammation when stable 23, 28. A longitudinal study is under way to investigate whether MSIs represent dysfunctional changes in genes, or whether they are markers of epithelial or other cell turnover and/or mutation.
It should be underlined here that the present findings do not suggest that MSI is the only responsible mechanism for frequent exacerbation or that the role of other parameters that affect exacerbation frequency, such as the bacterial airway load, is negligible 29. Indeed, an increased exacerbation frequency was associated with the presence of bacterial colonisation at baseline stable state in the present study. In contrast, the presence of bacterial colonisation was not associated with MSI. On this basis, MSI may be a biomarker of a causal mechanism, not directly related to bacterial colonisation, that leads to increased frequency of exacerbations.
It should certainly be acknowledged that quantitative sputum cultures were not performed, and viral colonisation, which may be also important in influencing the rate of exacerbation, was not assessed in the present study. This limitation should be considered in the interpretation of the results. In addition, the hospitalisation rate in the present study may be higher than rates previously reported. This is probably due to the structure of the healthcare system in Greece, where public primary healthcare is still developing. Hence, many patients are admitted to hospitals even for short hospitalisations, owing to the presence of a high standard public service in the community. However, this fact may not have significantly affected the present results because detection of exacerbations and evaluation of their severity was based on daily monitoring of symptoms using diary cards.
In conclusion, the instability of the microsatellite sequences that have been investigated indicates a destabilisation of the genome in chronic obstructive pulmonary disease patients. Oxidative stress may damage the DNA of lung cells, probably at the microsatellite level, leading to acquired somatic mutations. These mutations, expressed as microsatellite instability, permanently alter DNA auto-repair ability 30. This phenomenon was demonstrated, particularly in chronic obstructive pulmonary disease patients with an increased number of exacerbations, who were assessed during a 3-yr period. The current authors may speculate that the relatively high exacerbation rate found in chronic obstructive pulmonary disease patients with genetic instability could provide a link between alteration in DNA mismatch repair activity and oxidative damage due to frequent chronic obstructive pulmonary disease exacerbations and vice versa. Therefore, it would be of interest to consider not only the inherited alterations in the DNA but the somatic acquired mutations at the microsatellite DNA level, as this may provide novel information in the pathobiology of chronic obstructive pulmonary disease.
Statement of interest
None declared.
- Received December 16, 2007.
- Accepted May 5, 2008.
- © ERS Journals Ltd











{kind=link}
{kind=link}
{kind=link}
{kind=link}