





Abstract
Purinergic signalling regulates airway defence mechanisms, suggesting that extracellular purines could serve as airway inflammation biomarkers in cystic fibrosis (CF).
The purines adenosine triphosphate (ATP), adenosine diphosphate (ADP), adenosine monophosphate (AMP) and adenosine were measured in sputum from 21 adults (spontaneously expectorated from seven CF patients, induced from 14 healthy controls) to assess normal values and CF-associated changes. Subsequently, purine levels were measured in bronchoalveolar lavage fluid (BALF) from 37 children (25 CF patients, 12 disease controls) and compared with neutrophil counts, presence of airway infection and lung function. To noninvasively assess airway purines, ATP levels were measured using luminometry in exhaled breath condensate (EBC) from 14 children with CF and 14 healthy controls, then 14 CF children during a pulmonary exacerbation.
Both ATP and AMP were elevated in sputum and BALF from CF subjects compared with controls. In BALF, ATP and AMP levels were inversely related to lung function and strongly correlated with neutrophil counts. In EBC, ATP levels were increased in CF relative to controls and decreased after treatment of CF pulmonary exacerbation.
The purines adenosine triphosphate and adenosine monophosphate are candidate biomarkers of neutrophilic airways inflammation. Measurement of purines in sputum or exhaled breath condensate may provide a relatively simple and noninvasive method to track this inflammation.
- Biomarker
- bronchoalveolar lavage fluid
- cystic fibrosis
- exhaled breath condensate
- inflammation
- purinergic signalling
Extracellular adenyl purines, including the purine nucleotide adenosine triphosphate (ATP) and its metabolites, are important signalling molecules on airway surfaces. These purines serve as agonists for purinergic signalling pathways that play critical roles in airway mucus clearance. Indeed, ATP-mediated signalling regulates airway surface liquid volume, ciliary function and mucin secretion 1–3, each critical for control of mucus clearance rates.
Purines also mediate multiple components of inflammatory cell responses that are part of lung defence. For example, pro-inflammatory stimuli enhance release of ATP from epithelial 4–6 and inflammatory cells 7–10. In particular, stimulated neutrophils release ATP and accumulate both extracellular ATP and adenosine monophosphate (AMP) 10, 11. Inflammation also affects airway-luminal extracellular purine metabolism, both by altering ectonucleotidase activity on epithelial cell surfaces 12 and by addition of ectonucleotidase activity associated with the accumulation of inflammatory cells 8. ATP released onto airway surfaces in response to inflammation also stimulates inflammatory cell responses, including chemotaxis and degranulation in neutrophils 10, 13–15, cytokine production and oxidative bursts in macrophages 16–18, and activation of lymphocytes and eosinophils 17. Adenosine formed as a consequence of ATP release also acts as a signalling molecule with both pro-inflammatory and anti-inflammatory effects 19, 20.
The importance of purinergic signalling in lung inflammation has been demonstrated in vivo. For example, ATP receptor (P2Y1-R and P2Y2-R)-deficient mice exhibit impaired inflammatory responses and difficulty eradicating Pseudomonas from the lung 21. Similarly, mouse strains with modest increases in lung adenosine have enhanced interleukin (IL)-4-mediated inflammatory responses 22, and higher lung adenosine levels lead to airway inflammation and pulmonary fibrosis 23, 24. In vivo studies of airway purines in humans are limited, although increased levels of ATP have been observed in nasal lavage fluid 25 and blood 26 of subjects with cystic fibrosis (CF), and adenosine levels in airway secretions are elevated in untreated asthma and correlate with disease state 27–29.
The role of purines as mediators of the inflammatory response suggests that they may also be markers of inflammation. However, the concentrations and pattern of extracellular adenyl purines in the normal and diseased human airways surface remain largely unexplored. The aim of the present study was to measure the levels of purines in human airway secretions and evaluate their potential as biomarkers of airway inflammation, particularly in children with CF. First, purine levels were measured in sputum to establish normal values and assess changes associated with CF. In addition, purine levels were measured in the supernatant of mucopurulent material (SMM) aspirated from CF lungs removed for transplantation. Following this, bronchoalveolar lavage fluid (BALF) was collected from children undergoing clinically indicated bronchoscopy, and correlations were sought between purines and established markers of airways disease, including neutrophil counts, presence of infection and lung function. Finally, a simple and noninvasive method to measure airway purines in children by measuring ATP levels in exhaled breath condensate (EBC) was explored.
METHODS AND MATERIALS
Study subjects
Subject demographics are outlined in table 1⇓. Control populations were healthy individuals, except in the BALF study, which included the following disease controls: two subjects with primary ciliary dyskinesia and 10 subjects with recurrent cough or wheeze, all of whom were clinically stable at the time of bronchoscopy. All subjects were studied at the University of North Carolina at Chapel Hill (Chapel Hill, NC, USA), and studies were approved by the Institutional Review Board.
Study subject demographics
Study design
Differences between purine levels in airway secretions were assessed by comparison of CF with control populations. The relationship between purine levels and other markers of disease were assessed by regression analysis.
Methods
Sputum from healthy controls was collected and processed using induction as previously described 30. Briefly, mucus plugs were selected, weighed and incubated with 0.1% dithiotreitol to solubilise mucus. Sodium citrate was added at 0.32% to the sample buffers to limit hydrolysis of purines. Samples were then washed in Dulbecco’s PBS, filtered and analysed for cell viability, cell counts and differential. Sputum from CF subjects was collected by spontaneous expectoration, but was processed identically to induced samples.
SMM was recovered from the airway lumen of 13 excised human CF lungs at the time of transplant 31. This material was centrifuged at 440,000×g for 60 min at 4°C and the supernatant filtered through a 0.2-µm filter and frozen at -80°C.
BALF was obtained via clinically indicated bronchoscopy. Aliquots were placed on ice, centrifuged at 11,000×g for 5 min at 4°C to remove cells and bacteria, and the supernatant immediately frozen and stored at -80°C. Separate aliquots were processed for cell differential and quantitative microbiological culture.
EBC was collected using an RTubeTM device (Respiratory Research, Inc., Charlottesville, VA, USA). The chiller tube was held at -10°C until immediately before the collection, and the subject exhaled through the device during 7 min of tidal breathing. No nose clips were used. EBC was recovered from the RTubeTM and frozen at -80°C until analysis.
Purine analysis
Adenyl purines were measured in airway secretions using etheno-derivatisation and HPLC 32. Samples were boiled for 2 min prior to analysis, to inactivate nucleotidases.
Luminometry
The luciferin–luciferase assay was a modification of a previously described protocol 33. In brief, 100 µL aliquots from each sample were analysed in the light chamber of an LB953 AutoLumat luminometer (Berthold Technologies GmbH, Bad Wildbad, Germany) after a 100 µL injection of a luciferin–luciferase cocktail (luciferin 160 µg·mL−1 and luciferase 8 µM). Luminescence was recorded for 10 s and compared with an ATP calibration curve performed in parallel.
Analysis
All data are expressed as mean±se, except demographic information, which is reported as mean±sd. Data that did not follow a normal distribution by D’Agostino–Pearson tests were log-transformed prior to analysis, including all purine measurements and neutrophil counts. Comparisons between groups were performed using unpaired t-tests, except for pre- and post-antibiotic comparisons, which were performed on paired data. Correlations were performed using Pearson’s correlation.
RESULTS
Purine levels in normal induced sputum and CF sputum
To establish normal purine levels and assess whether these were altered in CF, purines were measured in sputum collected by induction from 14 healthy adults and spontaneously expectorated from seven adult CF subjects. Given the relationship between purines and inflammation, it was hypothesised that sputum purines would be elevated in subjects with CF, a disease characterised by high levels of airway inflammation. Purines were measured using etheno-derivatisation and HPLC, a technique which has been successfully utilised to measure purines from a variety of biological fluids 32. Assessment of recovery and metabolism of purines in sputum revealed that purines could be readily recovered and measured in both control and CF sputa (recovery rates: 89 and 81% for control and CF, respectively), and that purine metabolism during processing could be limited by addition of sodium citrate to the sample (for further details see supplementary data).
Analysis of sputa revealed the expected increase in neutrophilic inflammation in the CF sputa compared with control (14,700 versus 240 neutrophils·mg−1 sputum, respectively; p = 0.01). Differences in the pattern and concentration of purines were also observed. Analysis of purine concentrations in normal sputa revealed a pattern of adenosine ≈ AMP> adenosine diphosphate (ADP)>ATP. In contrast, CF sputa contained increased levels of both ATP and AMP, but not ADP or adenosine, relative to controls (fig. 1a⇓). Indeed, the ATP to adenosine ratio was elevated in sputa from CF subjects compared with control (mean±se: 33.0±6.6 versus 0.99±0.2, respectively; p = 0.003), as was the AMP to adenosine ratio (1.85±0.4 versus 0.08±0.0 for CF and control, respectively; p = 0.007). To ensure that the induction procedure in controls did not affect the results, purine levels were examined in paired spontaneously expectorated and induced sputum samples from three individuals (one CF patient and two with chronic obstructive pulmonary disease). Purine levels were actually modestly higher (approximately two-fold) in the induced samples, suggesting that the differences between CF and control could not be attributed to use of induction in the control population (data not shown).

Airway purines were elevated in cystic fibrosis (CF). a) Sputum was obtained by spontaneous expectoration from adults with CF (n = 7; •) and after induction in healthy controls (n = 14; ○), and purines measured in isolated supernatants. Both adenosine triphosphate (ATP) and adenosine monophosphate (AMP) were significantly elevated in CF compared with control, while adenosine diphosphate (ADP) and adenosine (Ado) levels were similar between groups. b) Supernatant of mucopurulent material (SMM) was obtained from the explanted lungs of adults with end-stage CF at time of lung transplantation (n = 13). The pattern of purine levels in SMM was similar to that observed in CF sputum. #: p<0.0001.
To assess whether these findings were reproducible in airway secretions not accessible to expectoration, SMM obtained from the airways of explanted CF lungs at the time of transplantation was obtained. The pattern of purines in the SMM from 13 explanted CF lungs was similar to that observed in CF sputum, with proportionally higher levels of AMP and relatively low levels of adenosine (fig. 1b⇑). Thus, the pattern of purines in CF secretions appeared to be independent of sample collection technique.
Airway purines were elevated in BALF from children with airways disease and correlated with neutrophilic bronchitis
The present authors wished to determine whether the relationship between purines and airways disease could also be observed in children. Due to the frequent inability of children to expectorate sputum, airway secretions were obtained using bronchoalveolar lavage (BAL). BALF was prospectively collected and analysed from 25 children with CF and 12 non-CF subjects (disease controls; DC). Similar to the previous data, higher levels of both ATP and AMP were observed in CF BALF, compared with DC BALF, with AMP present at the highest absolute concentration (fig. 2a⇓). Neither ADP nor adenosine levels differed among the groups.
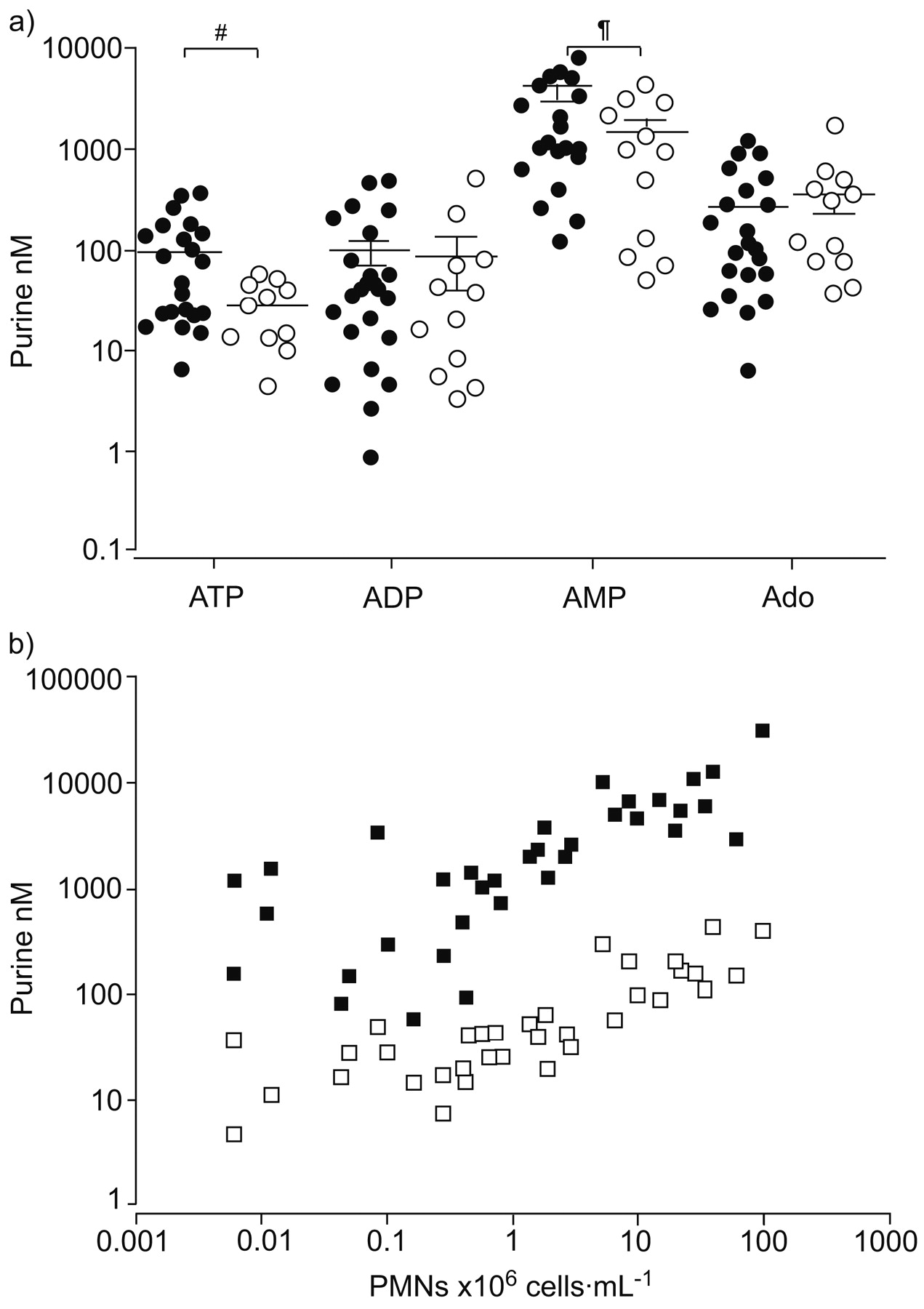
Purines in bronchoalveolar lavage fluid (BALF) from children were elevated in cystic fibrosis (CF) and correlated with neutrophilic airway inflammation. a) BALF was obtained from children with CF (n = 25; •) and from disease controls (n = 12; ○) with other respiratory diseases. Measurement of purines in the supernatant of this BALF revealed elevated levels of adenosine triphosphate (ATP) and adenosine monophosphate (AMP) in the CF group. b) Statistically significant correlations were observed between polymorphonuclear neutrophil (PMN) counts and levels of both ATP (□) and AMP (▪) in BALF. ADP: adenosine diphosphate; Ado: adenosine. #: p = 0.0164; ¶: p = 0.0300. b) ATP: r = 0.81, p<0.0001; AMP: r = 0.74, p<0.0001.
While higher levels of ATP and AMP were observed in BALF from CF subjects, it could not be distinguished whether the differences were CF specific or reflected the higher levels of airway bacterial infection and/or neutrophilic bronchitis that characterise CF airways disease 34. To determine the variables most closely correlated with purine levels, a multiple regression model was used to assess whether CF status, presence of airway infection (>50,000 pathogens·mL−1 on BALF culture) or neutrophil cell count best predicted ATP or AMP levels in BALF. In the resulting model, only neutrophilic counts emerged as a significant predictor of ATP or AMP levels, with strong correlations to both ATP and AMP (fig. 2b⇑). In contrast, neutrophil counts were not strongly correlated with either adenosine (r = -0.22, p = 0.19) or ADP (r = 0.25, p = 0.14). Similar correlations were observed in the sputum samples between neutrophil counts and both ATP and AMP (r = 0.75, p = 0.0007 and r = 0.81, p = 0.0001, respectively), although the results were limited by the small number of subjects from whom accurate cell counts could be obtained (three CF subjects and 14 controls). These data suggest that ATP and AMP are primarily biomarkers of neutrophilic inflammation.
Airway purines correlated with lung function
Since neutrophilic inflammation mediates many of the clinical manifestations of CF airways disease, including declines in lung function, the present authors tested for correlations between purine levels in BALF and lung function. Although significant correlations were observed between raw ATP and AMP values and lung function (data not shown), it was recognised that variable dilution of airway secretions in BALF could confound the relationship between BALF biomarkers and clinical outcomes. The current authors attempted to control for dilution using the BALF to serum urea ratio, a widely used albeit problematic dilution marker 35. However, a correlation trend was observed between urea-based dilution factors and neutrophil counts (r = -0.40, p = 0.056), suggesting that BALF urea levels were artefactually increased in diseased airways, perhaps by increased efflux of urea through inflamed epithelia during lavage 35. Therefore, an alternative method to control for dilution using ratios of ATP or AMP to adenosine was examined, since ratios are not affected by dilution. This method is based on the observation that both ATP and AMP correlate with markers of airways disease, whereas adenosine does not. As anticipated, significant correlations were observed for both ATP/adenosine and AMP/adenosine ratios with the percentage of neutrophils as dilution-independent markers of bronchitis (fig. 3a⇓). Furthermore, significant correlations were also seen between the purine ratios and per cent predicted forced expiratory volume in one second (FEV1; fig. 3b⇓). These data indicate that with appropriate methods to control for dilution, airway ATP and AMP levels correlate with a clinically relevant index of disease severity as expected for a biomarker of neutrophilic inflammation.

Purine ratios correlated with neutrophilic airway inflammation and lung function. Ratios of adenosine triphosphate (ATP) to adenosine (Ado; □) and adenosine monophosphate (AMP) to Ado; ▪ were calculated as markers of purine levels corrected for variable dilution of airway secretions in bronchoalveolar lavage fluid. a) Both ATP/Ado and AMP/Ado ratios were strongly correlated with percentage of polymorphonuclear neutrophils (PMNs) as a dilution-independent marker of inflammation. b) Purine ratios were compared with spirometry data available from a subset of subjects (n = 28, 20 cystic fibrosis and eight disease controls). Both ATP/Ado and AMP/Ado ratios were negatively correlated with forced expiratory volume in one second (FEV1 % predicted). a) ATP/Ado: r = 0.76, p<0.0001; AMP/Ado: r = 0.67, p<0.0001. b) ATP/Ado: r = -0.41, p = 0.0335; AMP/Ado: r = -0.43, p = 0.0240.
ATP in EBC was correlated with airway inflammation
While the present data demonstrated that the purines ATP and AMP are potential biomarkers of neutrophilic inflammation in children with CF, risks and technical challenges associated with BAL limit clinical application. To determine whether airway purines could be measured using a simple and noninvasive method in children, the feasibility of detecting purines in EBC was explored.
In a pilot study, EBC was obtained from a small group of healthy and CF children (four in each group). Initial analyses using etheno-derivatisation and HPLC revealed that EBC purine concentrations were below the etheno-derivatisation detection threshold in most individuals (data not shown). As a more sensitive method, a highly sensitive and specific luminometry method was utilised, which is widely used to measure ATP levels in biological samples 25, 36, 37. With luminometry, a signal above background was detected in each of the pilot EBC samples (mean±se (range) 840±320 (157–2,428) arbitrary light units (ALU)). Consistent with the signal being ATP specific, the signal disappeared with sample pre-incubation for 30 min with 2 units·mL−1 of the ATP degrading enzyme apyrase (post-treatment 15±5 ALU; fig. 4a⇓), but not in time-control incubations. Based on comparison to known standards, EBC ATP concentrations were in the low picomolar range, consistent with those measured in BALF and sputum after taking into account the 103–104 (or higher) dilution of airway secretions in EBC 38, 39. At this concentration range, reproducibility was modest, with within-sample coefficients of variation between 20–30%. For this reason, EBC ATP levels were reported as the average of duplicate measures.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Adenosine triphosphate (ATP) in exhaled breath condensate (EBC) was elevated in cystic fibrosis (CF) and decreased with treatment of a CF exacerbation. ATP levels in EBC were measured by luminometry. a) Pilot EBC collections were obtained from four healthy controls (subjects 1–4) and four CF subjects (5–8). A luminescent signal was detected in all samples that was stable to incubation at 37°C for 30 min (▓), compared with samples kept at 0°C on ice (▪), and disappeared after incubation with 2 units·mL−1 of the ATP degrading enzyme apyrase (□). b) ATP levels were measured in EBC from CF (n = 14) and healthy controls (n = 14). ATP was elevated in the CF group. c) ATP levels in EBC were measured at the start and end of a course of antibiotics to treat a pulmonary exacerbation in children with CF (n = 14). ATP levels were lower at the end of treatment. ALU: arbitrary light units. #: p = 0.0441; ¶: p = 0.0175.
To further assess EBC ATP levels with the luminometric method, the pilot study was expanded to include EBCs collected from a total of 14 children with CF and 14 healthy controls during regular clinic visits. Consistent with the previous results, EBC ATP levels were elevated in children with CF compared with healthy controls (fig. 4b⇑). Treatment of a CF exacerbation reduces neutrophilic airway inflammation 40; thus, it was hypothesised that EBC ATP levels would drop during treatment. To explore this relationship, EBC was collected from 14 children with CF at the beginning and end of a course of intravenous antibiotics for a pulmonary exacerbation, including four CF subjects from the previous study. The mean±sd treatment duration was 21.6±3.3 days, with antibiotics chosen by the treating physician. As expected, lung function improved after antibiotic treatment (mean±sd FEV1 % pred: 60.1±20.1% pre- versus 70.1±19.9% post-antibiotics, p≤0.01). This improvement was associated with a three-fold fall in EBC ATP levels (fig. 4c⇑), consistent with previously observed changes in sputum markers of neutrophilic inflammation after treatment 40. Although these data are preliminary, they do indicate that EBC ATP levels fit the pattern expected for a biomarker of neutrophilic inflammation.
DISCUSSION
Extracellular purines are the signalling molecules of purinergic signalling pathways that regulate airway defences, including mucociliary clearance and intraluminal inflammatory responses. In the present study, it was demonstrated that both the pattern and concentration of these purines have a strong relationship to CF airways inflammation. Analyses of secretions from CF subjects obtained as sputum, SMM and BALF provided a remarkably consistent picture in which AMP was the dominant purine, and both ATP and AMP were elevated in CF compared with control (table 2⇓). This pattern of purines differed significantly from the relatively equal levels of AMP and adenosine observed in sputum from normal subjects, which in turn was similar to that reported in cultures of normal airway epithelia 32. Although subjects with CF were primarily studied, the data suggest that the relationship between purines and neutrophilic inflammation is not CF specific. However, further study is necessary before the present findings can be confidently generalised to non-CF airways disease.
Relative purine composition of airway secretions
While the source of airway purines was not identified in the present study, the strong correlation between purine levels and neutrophil counts suggests that neutrophils may be a major contributor to purine levels in CF airway secretions. This conclusion is consistent with previous studies showing that activated neutrophils exhibit increased release of ATP and accumulate AMP 41. However, purine release from necrotic or apoptotic cells cannot be excluded, nor can a significant contribution from inflamed airway epithelia or other inflammatory cells be ruled out. Although bacteria are another potential source of extracellular purines, it seems unlikely that bacteria significantly contributed to ATP release at levels commonly found in CF sputum (∼107·mL−1) 42. The accumulation of AMP suggests a relative absence of 5′-nucleotidase metabolism of AMP to adenosine, a pattern which has been observed in isolated neutrophils (which lack 5′-nucleotidase) but not airway epithelia 32, 43. Therefore, the high levels of AMP in samples obtained from diseased airways suggest that neutrophils dominate the metabolic pattern of purine nucleotides on these airway surfaces.
Regardless of the underlying mechanism(s), the strong correlation with neutrophil counts indicates that airway levels of ATP and AMP are potential biomarkers of neutrophilic inflammation. The present data suggest that measurement of ATP in EBC may hold promise as a simple and noninvasive method to assess the degree of neutrophilic airway inflammation in children. Indeed, the approximately three-fold reduction in EBC ATP levels after treatment of CF pulmonary exacerbation parallels the reduction of neutrophil cell counts and IL-8 levels in sputum after similar treatment 40.
However, the current results also highlighted many of the known limitations to EBC analysis. The measured ATP concentrations were low and near the threshold for detection, suggesting that small technical artefacts or variations could significantly affect the results. Furthermore, the small volumes of EBC collected precluded measurement of both ATP and dilution markers. Consequently, systematic differences in sample dilutions among groups could not be assessed and could contribute to the observed differences. Therefore, further improvements in methodology are needed for more thorough evaluation of the clinical potential of EBC purine measurements.
While ATP and AMP emerged as potential biomarkers, similar findings were not observed for adenosine. While the levels of adenosine in BALF were similar to previously published values 27, the present authors did not observe the elevated levels of airway adenosine 27, 28 or correlation to disease severity previously described for asthma 29. This difference may reflect fundamental differences in airway pathophysiology between asthma and CF. CF is characterised by a pathogen- and neutrophil-dominated airway inflammation that differs significantly from the less cellular, eosinophil rich, and relatively sterile airway inflammation observed in asthma. These findings suggest that factors responsible for increased adenosine levels in asthma are not common in the neutrophilic bronchitis that characterises CF.
In addition to exploring the potential of airway purines as biomarkers of inflammation, the present study also provides new insights into purinergic signalling pathways in airways disease. While it was not possible to accurately determine the dilution in the BALF samples, both the ATP and adenosine levels in BALF were consistent with previous reports 25, 27, and previous studies suggest that airway secretions in BALF were probably diluted 10–100-fold 35. Given this level of dilution, in situ ATP levels would be above the median effective concentration (EC50) for the P2Y2 ATP receptor in airway epithelia (0.24 μM) 44 and approach the levels needed to activate P2Y2 receptors in inflammatory cells 13, 45. These considerations suggest that ATP-mediated purinergic signalling may be adaptively increased in bacterially infected airways, leading to higher mucociliary clearance and greater activation of inflammatory cells. Similarly, the average adenosine levels in both healthy and CF airways are predicted to be above the EC50 values of the A1 and A2a adenosine receptors (0.31 and 0.73 μM, respectively) found on inflammatory cells 46, 47, although somewhat lower than the EC50 of the dominant adenosine receptor (A2b) expressed in airway epithelia 32. As adenosine levels did not correlate with markers of disease, the present authors would not anticipate that adenosine-mediated signalling would increase with neutrophilic inflammation, and the increased ATP to adenosine ratio might favour a more pro-inflammatory environment 20. However, recently published evidence suggests that AMP may serve as an adenosine receptor agonist, either directly 48 or after conversion to adenosine at the epithelial surface 49. Thus, increased adenosine receptor signalling, mediated through AMP, could modulate increased inflammation.
In conclusion, the present study demonstrates that purines recovered in airway secretions are biomarkers of neutrophilic airway inflammation and are elevated in cystic fibrosis airways disease. The results suggest that measurement of purines in exhaled breath condensate may be useful as a noninvasive method of assessing airway inflammation, although further refinements are necessary.
Support statement
C.R. Esther Jr was supported by the National Institutes of Health (NIH), grant No. K12 RR17667, and the University of North Carolina Program for Translational Science. N.E. Alexis was supported by the US Environmental Protection Agency, grant No. CR829522. S.H. Donaldson was supported by grant No. K08 HL68617 from the NIH. C.G. Moore was supported by NIH grants K12 RR023248 and K30 RR022267. R.C. Boucher was supported by NIH grants HL34322 and HL084934. N.E. Alexis, E.R. Lazarowski, S.H. Donaldson and R.C. Boucher were supported by the NIH Specialized Centers of Clinically Oriented Research (SCCOR) program, grant No. NHLBI P50HL084934.
Statement of interest
None declared.
Acknowledgments
The authors wish to thank C. van Heusden (University of North Carolina at Chapel Hill, Chapel Hill, NC, USA) for assistance measuring purine levels in airway samples.
Footnotes
-
This manuscript has supplementary data accessible from www.erj.ersjournals.com
- Received July 16, 2007.
- Accepted January 20, 2008.
- © ERS Journals Ltd
References










