





Abstract
Tumour necrosis factor (TNF)-α has been shown to be an important factor in animal models of chronic obstructive pulmonary disease (COPD). However, human studies of TNF polymorphisms in COPD have been equivocal.
Six TNF single nucleotide polymorphisms (-1031C/T, -863C/A, -857C/T, -237G/A, -308G/A and +487G/A) and their haplotypes were investigated in 423 Caucasian smokers (298 patients with spirometric evidence of COPD and 125 without airflow obstruction).
The -308 minor allele (A) had a higher odds ratio (OR) of being associated with COPD in multivariate analysis (controlling for age, sex, pack-yrs; OR 1.9, 95% confidence interval (CI) 1.1–3.2) and was also associated with worse forced expiratory volume in one second/forced vital capacity. The -237 minor allele (A) had a lower OR of being associated with COPD (OR 0.40, 95% CI 0.19–0.86). In COPD patients, the -857 minor allele (T) had a lower OR of being associated with severe stages of COPD (Global Initiative for Obstructive Lung Disease stage III and IV versus stage I and II, OR 0.46, 95% CI 0.24–0.88). Other TNF single nucleotide polymorphisms were not associated with COPD but the -1031/-863 haplotype CC/TC had a lower OR in COPD patients versus smoking controls (OR 0.22, 95% CI 0.05–0.97).
The present study adds further evidence that tumour necrosis factor genotypes play a role in susceptibility to cigarette smoke.
Chronic obstructive pulmonary disease (COPD) develops in only 25–40% of cigarette smokers 1. However, risk factors for susceptibility to COPD in smokers have not been completely determined. α1-Antitrypsin deficiency, which is the best documented genetic risk factor for COPD, accounts for only an estimated 1–2% of cases 2, 3. Other host factors are suspected to be involved in the remaining 98–99% of cases.
One candidate susceptibility gene for COPD is tumour necrosis factor (TNF), the gene coding for the protein that is processed to TNF-α. In mice, TNF-α overproduction has led to pulmonary emphysema and inflammation 4, 5 and is thought to drive ∼70% of cigarette smoke-induced emphysema and inflammation 6, 7. TNF-α may exert its effects by stimulating the release of other enzymes, such as macrophage metalloelastase 8. In COPD patients, there is a higher concentration of TNF-α in bronchial biopsies 9, induced sputum 10 and bronchoalveolar lavage fluid (BALF) compared with control subjects 11. TNF-α levels in sputum are also increased significantly during acute exacerbations of COPD 12, 13. A recent meta-analysis found an association between COPD and elevated serum TNF-α levels 14. In contrast, healthy smokers have no increase in TNF-α in BALF 11, 15 and their alveolar macrophages have a decreased release of TNF-α 16, 17.
The factors that lead to increased TNF-α in COPD patients but not in smokers with normal lung function are unknown. One possibility is that TNF expression is regulated by single nucleotide polymorphisms (SNPs) in the gene. For instance, increased transcriptional activity of the TNF gene has been associated with the -308A allele in various disorders 18–23. The TNF -863A allele has been associated with increased gene 24 and TNF-α expression from peripheral blood mononuclear cells 25. The -857T and -1031C alleles have been associated with increased transcriptional activity of the TNF gene 25. The -237A allele has shown mixed results in association with TNF-α protein production 26–28.
Despite these promising in vitro studies, not all of these SNPs have been studied in COPD populations and those that have been studied often have conflicting results (table 1⇓). These inconsistencies may be due to study design limitations such as small number of subjects, genotyping with a limited number of informative SNPs, lack of haplotyping with multiple SNPs, failure to adjust for confounding variables, such as age, and lack of comparison to healthy smoking controls, the most relevant comparison group. In the present study some of these limitations were addressed by genotyping six TNF SNPs with biological activity in a large number of subjects with well-defined physiological phenotypes. Multivariate analysis was also used and TNF-α genotype/haplotype associations with COPD were examined.
Previoustumour necrosis factor-α single nucleotide polymorphisms (SNPs) association studies in chronic obstructive pulmonary disorder (COPD)
METHODS
Selection and description of participants
All subjects were studied under protocols approved by the Institutional Review Board at the National Jewish Medical and Research Center (Denver, CO, USA) or the Colorado Multiple Institution Institutional Review Board (Denver, CO, USA), with guidelines recommended by the National Institutes of Health (Bethesda, MD, USA). Signed informed consent was obtained for all subjects. Control subjects were healthy volunteers recruited from the local community by word of mouth and advertising, had no report of respiratory symptoms or disease and had a smoking history >20 pack-yrs. Patients with COPD were recruited from an outpatient pulmonary clinic. The diagnosis of COPD was made using Global Initiative for Obstructive Lung Disease (GOLD) criteria 49 using a post-bronchodilator forced expiratory volume in one second (FEV1) after the onset of full expiration compared FEV1 % predicted for age, sex and ethnicity based on a sample of the general population of the USA 50. GOLD state I patients (FEV1/forced vital capacity (FVC) <0.7 and FEV1 ≥80% pred) were included as cases. Patients with emphysema on high-resolution computed tomography and normal pulmonary function test (n = 11) were placed in GOLD stage I for analysis (table 2⇓).
Study subject characteristics
Blood collection
A total of 6 mL of blood was withdrawn from the antecubital vein into a sterile 13×1,000-mm sodium heparin Vacutainer Plus (BD, Franklin Lakes, NJ, USA). The sample was immediately centrifuged at 2,100×g for 10 mins at room temperature. The buffy coat was removed and stored at -80°C.
DNA extraction/isolation and genotyping
Buffy coats were used to extract DNA using QIAamp 96 DNA Blood Kit (QIAGEN, Valencia, CA, USA), and the DNA was eluted with nuclease-free water. A total of six SNPs were tested in all subjects. The polymorphisms -1031T/C, -863C/A and -857C/T were tested using PCR conditions and primers as previously described 51. Direct haplotypes were also tested using two pairs of primers for -857C/T with -237G/A and -308G/A with +488G/A as previously described 51, 52. Each SNP was analysed using a sequence specific primer to detect the presence of that SNP.
Data analysis
Genotype frequencies of each polymorphism in the case and control populations were evaluated for departures from Hardy–Weinberg equilibrium, using Chi-squared tests (p<0.001). Tests for genotypic differences between cases and controls were conducted in the context of logistic regression, univariately and multivariately (adjusting for sex, age and smoking pack-yrs, where appropriate). A dominant model was used for the genetic analysis. Caucasians accounted for the vast majority of subjects and, thus, it was the only group analysed in the present study. Univariate and multivariate linear regression models were used to assess the influence of genotypes on cross-sectional continuous severity outcomes (FEV1 % pred and FEV1/FVC). Normalising transformations were performed on continuous outcome variables when necessary to better approximate model assumptions. For analysis of severity, GOLD stage was dichotomised to a mild-to-moderate (GOLD stage I or II) and severe disease (GOLD stage III or IV). Genotypic differences between cases with severe and mild-to-moderate disease were evaluated in the context of logistic regression univariately and multivariately. The measures of linkage disequilibrium, d' and R2, were calculated using Haploview (Copyright 2003–2005 Whitehead Institute for Biomedical Research, Cambridge, MA, USA). In addition, Haploview was also used to determine haplotype blocks using the confidence interval method 53.
Haplotype frequencies were estimated using Haplo.Score 54. This software uses an expectation maximisation-based algorithm to calculate the posterior probability of each possible haplotype combination for each individual when haplotype phase is unknown. In order to adjust for the uncertainty in haplotype assignments, a weighted logistic regression model was used. Each subject could appear in the dataset more than once, with each entry weighted by the probability of that haplotype combination for that individual, so that the total contribution of each individual was one observation. Both haplotype combination and single haplotype effects were tested for the presence of a specific haplotype pair versus no presence and for carrying at least one specified haplotype versus not carrying the specified haplotype.
RESULTS
Demographics
The COPD and control groups were significantly different in FEV1 % pred (45.0±19 and 98.5±18% for COPD and controls, respectively; p<0.0001; table 2⇑). Compared with COPD patients, control subjects were more likely to be male, but had a similar smoking history (in pack-yrs). Only Caucasians were analysed in the present study to minimise the effects of population stratification.
TNF SNP genotypes
TNF genotype frequencies are listed in table 3⇓. A genotype with the -308 minor allele (GA or AA) was significantly more frequent in COPD patients than in control subjects in both univariate (odds ratio (OR) 1.9, 95% confidence interval (CI) 1.1–3.2; p = 0.03) and multivariate analyses (OR 1.9, 95% CI 1.1–3.4; p = 0.03; table 4⇓). There was significantly less chance of having the genotype with the -237 minor allele (GA or AA) in COPD patients than control subjects by multivariate analysis (OR 0.40, 95% CI 0.19–0.86; p = 0.02; table 4⇓).
Genotype frequencies oftumour necrosis factor (TNF)-α single nucleotide polymorphisms (SNPs)
Univariate and multivariate analyses(dominant model)
A genotype with a minor allele for the -857 SNP (CT or TT) had a statistically significant lower OR in COPD subjects with severe COPD (GOLD stage III and IV) compared with those with mild–moderate COPD (stage I and II) in both univariate (OR 0.5, 95% CI 0.26–0.95; p = 0.03) and multivariate analyses (OR 0.46, 95% CI 0.24–0.88; p = 0.02; supplementary table S3). No association was found with any of the genotypes and FEV1 % pred (data not shown), although the -308 genotype (GG) was associated with a higher mean FEV1/FVC (supplementary table S4). There were no statistically significant associations with COPD for SNPs -1031, -863 and +488.
Haplotype analysis
Haplotype blocks were constructed according to the confidence interval method of Gabriel et al. 53 in cases and controls separately using Haploview. This method uses both an estimate of d' and a measure of its precision (confidence bounds) to construct haplotype blocks (fig. 1⇓). Blocks with pairwise d' <1 have actual d' values in the squares. Although the estimated pairwise linkage disequilibrium (LD) between many of the SNPs was high, the precision of the estimates was not high enough to fulfill the criteria for construction of haplotype blocks utilising all the SNPs. The estimate of LD between the -1031 SNP and the -863 SNP was the only estimate that had sufficient precision to warrant construction of a haplotype block. The estimated frequencies can be found in supplementary table S5. There were no haplotypes associated with COPD (data not shown).
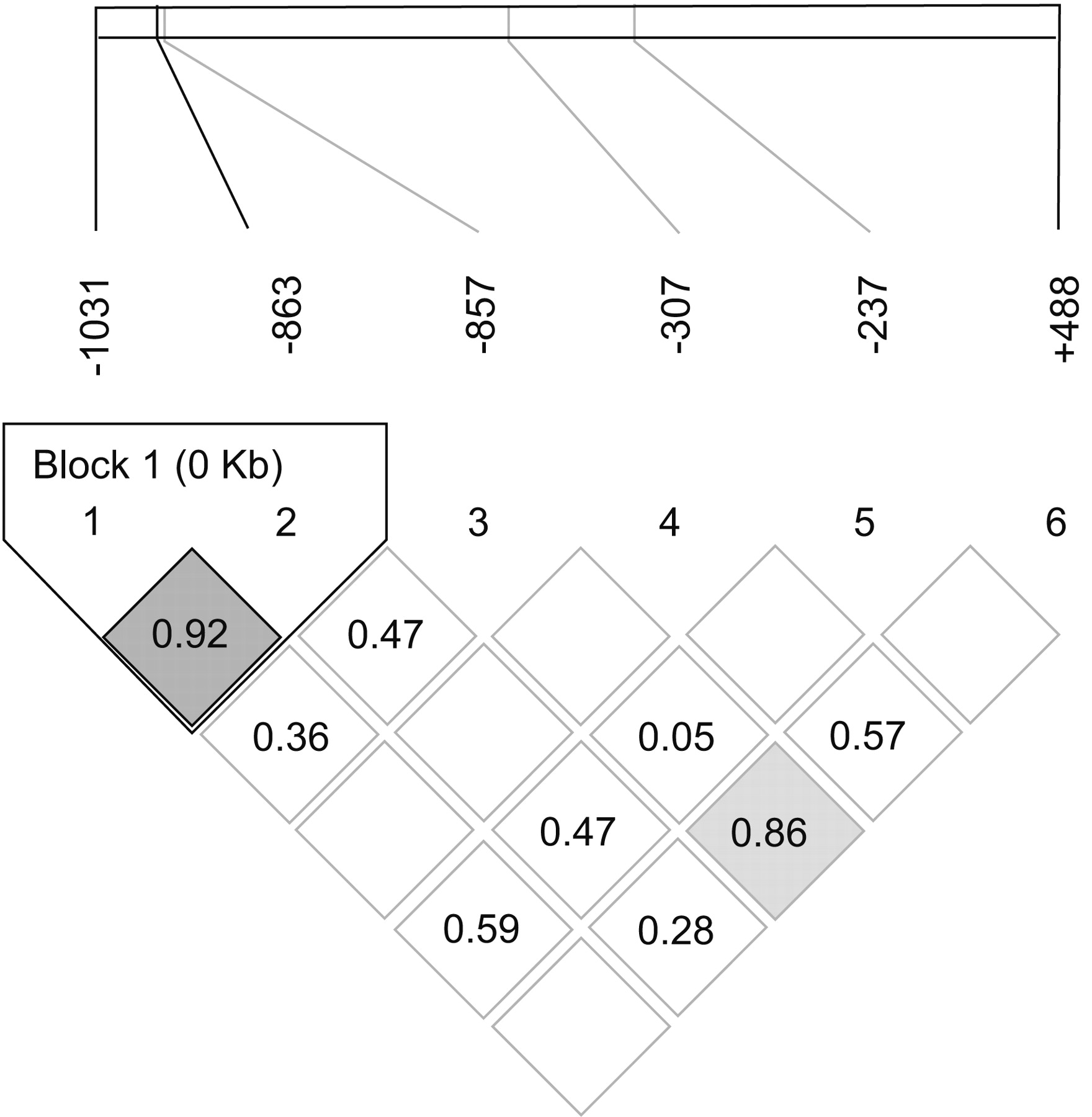
Linkage disequilibrium plot of tumour necrosis factor haplotypes. Haplotypes were constructed from genotyping data from Caucasians using the Gabriel block method 53. Significant d' values are shown. There was only one block of SNPs (-1031 and -863).
Meta-analysis of the -308 and -237 SNPs in COPD
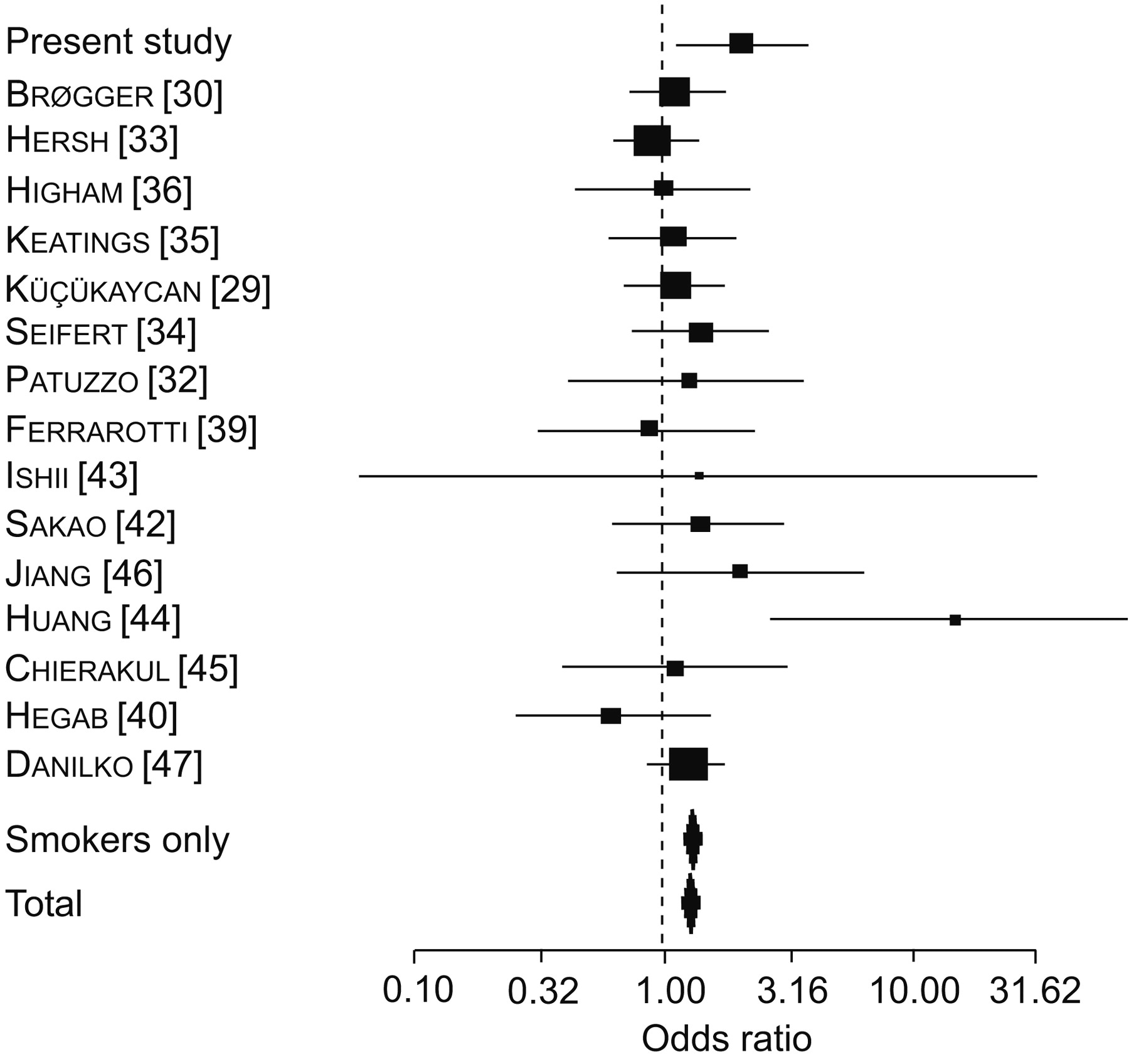
In order to put the present results in perspective, a search of the online database PubMed for previously reported frequencies of TNF SNPs was performed. For the -308 SNP, data was extracted from all the studies listed in table 1⇑, except for one that did not report frequencies for case and control separately 31, two that only reported rapid decliners with no cases 37, 38 and one that only reported emphysema in COPD subjects 42. Combining the present data with the remaining 16 studies (a total of 610 cases and 1,612 controls), a genotype with the -308 minor allele was found to have an OR±se of 1.28±0.03 for COPD. Four of these studies did not use healthy smokers as their control group or did not state whether the individuals in the control group were smokers 29, 32, 46, 47. Therefore, data was only pooled from studies that compared COPD subjects with healthy smokers (fig. 2⇓) and found an OR±se of 1.29±0.04 for COPD with the -308 SNP.

Forest plot of the odds ratio (OR) of having chronic obstructive pulmonary disease (COPD) with genotype of GA or AA of -307 single nucleotide polymorphism in the present study and previously published studies. Boxes indicate the point estimate and whiskers represent 95% confidence intervals (CIs). The size of the box is proportional to the number of subjects in the study. Diamonds represent the combined ORs and CIs for all studies (total) and for studies comparing COPD patients with smoking controls (smokers only).
SNP frequencies for the -237 TNF SNP were also compared with other populations. Combining the present results with the pooled data from three other studies listed in table 1⇑, the ORs were not statistically significant either for all subjects (OR±se 1.25±0.12) or for the studies just comparing COPD subjects with smokers (OR±se 1.22±0.14; fig. 3⇓).

{kind=link}
{kind=link}
{kind=link}
Forest plot of the odds ratio (OR) of having chronic obstructive pulmonary disease (COPD) with genotype GA or GA of -237 single nucleotide polymorphism in the present study and previously published studies. Boxes indicate the point estimate and whiskers represent 95% confidence intervals (CIs). The size of the box is proportional to the number of subjects in the study. Diamonds represent the combined ORs and CIs for all studies (total) and studies comparing COPD patients with smoking controls (smokers only).
DISCUSSION
TNF-α plays an integral role in the pathogenesis of COPD. In the present study, the most comprehensive haplotype evaluation to date using six single nucleotide polymorphisms in TNF was performed. These SNPs were chosen based on their association with changes in biological activity and result from previous studies in COPD. Some of these SNPs have been previously reported to be independently associated with COPD 29, 33, 41, 42, 44, 46. For instance, it was confirmed that a genotype (GA or AA) with the minor allele of the -308 SNP was associated with a higher OR of having COPD, compared with smoking controls. Other SNPs (e.g. -237) and haplotypes were associated with a lower OR of having COPD or less severe disease.
The strongest association observed was for the most studied SNP, -308 (table 1⇑). This SNP is in the promoter region of the TNF gene and is associated with increased gene transcription 18–23. Although several earlier studies have shown an association of the -308 minor allele with COPD 33, 41, 42, 44, 46, four of these studies were in Asian populations 41, 42, 44, 46 in which the minor allele frequency is much lower. The present study is only the second to show this association in Caucasians, the first being a large family study from the Boston early-onset COPD study 33. Despite multiple studies showing positive associations, there are also 13 studies reporting no association between the -308 genotype (GA and AA) and COPD, including 10 in Caucasian populations 29–32, 34, 37–39. Previously, it was felt that the difference in studies were due to small sample size (underpowering) or low minor allele frequency 29; however, a Forest plot (fig. 2⇑) suggests that there is an association despite variability among populations.
The second most significant association observed in the present study was with the -237 genotype (GA and AA). This SNP has been associated with decreased transcriptional activity and reduced TNF-α production from peripheral blood mononuclear cells 55. The present multivariate analysis of Caucasian subjects showed that this genotype was less likely to be found in COPD subjects (7% in controls versus 4% in COPD subjects). Previous studies have reported no association of this SNP with COPD 29, 30; these studies had minor allele frequencies in controls (4 and 6%, respectively), slightly lower than in the present study (7%). In another study 33 the sample size was larger (n = 718), yet minor allele frequencies were also lower in control subjects (4% for controls and 6% in cases; C. Hersh; Pulmonary and Critical Care Division, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA; personal communication) suggesting that this association may have been due to a false-positive association (fig. 3⇑).
Although other TNF SNPs appear to have biological activity in vitro, only two of these other SNPs (-376 and +488) have been previously reported in COPD studies 29, 30, 33, 40. The +488 SNP has been associated with renal cell carcinoma 56 and prostate carcinoma 57. This SNP is in the first intron of the TNF transcript but its significance is unclear 51, 58, 59. In most studies there was no association between this SNP and COPD 33, 40 except for one study that compared COPD patients with healthy donors 29. Surprisingly, this study found that the association between the +488 SNP and COPD was even stronger for COPD subjects that had none or limited radiographical evidence of the disease 29. Although the -376 SNP was not included in the present study, it is associated with an increase in TNF transcriptional activity and very strongly associated with an increased risk of cerebral malaria 60.
The present study is the first to report genotype frequencies of the -857 SNP in COPD, although it has been studied in other pulmonary diseases. This SNP is thought to be associated with decreased transcription by affecting binding of OCT1 and nuclear factor (NF)-κB transcription factors in the TNF promoter region, although reports have been conflicting 25, 61, 62. Although in this investigation the OR for this SNP was not statistically significantly different, it was associated with mild-to-moderate COPD (GOLD stages I and II). It is speculated that the -857T allele affects TNF-α production negatively in certain inflammation pathways using different transcription factors, thus leading to less inflammation of the airways and destruction of lung parenchyma: a model similar to that postulated for the gut in inflammatory bowel disease 61.
One strength of the present study is that multiple TNF SNPs were investigated and a haplotype analysis was conducted. Although only two SNPs were in significant LD, the haplotype block -1031/-863 was found to be associated with COPD. This region of TNF is also thought to play a role in binding of OCT1 and NF-κB transcription factors to the promoter region of TNF and the minor alleles are felt to cause increased TNF transcription 24, 25, 63. The minor alleles for the -1031 and -863 SNPs have also been reported to be associated with gastric ulcers and gastric cancer 64. In the haplotype in which COPD was found to be less likely, CC/TC -1031/-863, the present authors hypothesise that several minor alleles at these sites make a patient less likely to have increased TNF-α production and, therefore, less likely to develop COPD.
In summary, the present study is one of the larger and more comprehensive studies of tumour necrosis factor polymorphisms in chronic obstructive pulmonary disease. It was confirmed that the well studied -308 single nucleotide polymorphism is associated with chronic obstructive pulmonary disease and other associations with the tumour necrosis factor gene were also reported, suggesting that tumour necrosis factor polymorphisms may play a role in the susceptibility to tobacco smoke. Additional large independent studies in both Caucasian and non-Caucasian populations are needed to replicate the present findings.
Support statement
This study was supported by the Kenneth Monfort Foundation, the Flight Attendant Medical Research Institute (Miami, FL, USA), Specialized Program of Research Excellence In Lung Cancer (University of Colorado Cancer Institute, Aurora, CO, USA) grant CA58187 and General Clinical Research Centre/National Institutes of Health grant MO1 #RR000051.
Statement of interest
None declared.
Acknowledgments
The authors would like to thank J. Orcutt, A. Jonth, C. Wheeler and M. Nicks (Dept of Medicine, National Jewish Medical and Research Centre, Denver, CO, USA), and R. du Bois and K. Welsh (Interstitial Lung Disease Unit, Royal Brompton Hospital, Imperial College of Science, Technology and Medicine, London, UK).
Footnotes
-
This manuscript has supplementary data accessible from www.erj.ersjournals.com
- Received August 3, 2007.
- Accepted January 23, 2008.
- © ERS Journals Ltd
References










