





Abstract
Rapid oxygen consumption by markedly increased numbers of hypermetabolic leukocytes in leukaemic patients resulting in the apparent diagnosis of hypoxaemia on arterial blood gas analyses is termed leukocyte larceny.
In the present report, a case of polycythaemia vera, extreme thrombocytosis, normal leukocyte counts and arterial hypoxaemia in the absence of clinical, radiological or physiological evidence of lung disease is described.
This pseudohypoxaemia case was established by pulse oximetry, as well as by incubation of a blood specimen with potassium cyanide, and became less significant after the use of cytoreductive agents showed a proportionate increase in arterial oxygen tension as platelet counts decreased on serial arterial blood gas analyses.
The present case report demonstrates spurious hypoxaemia due to extreme thrombocytosis and shows that, beside significant leukocytosis, even markedly elevated platelet counts can cause larceny of arterial blood oxygen.
In 1979, Hess et al. 1 showed that arterial oxygen tension (Pa,O2) fell at a faster rate in patients with leukocytosis than in control subjects, and that this fall was great enough to result in an incorrect diagnosis of hypoxaemia. This artefactual phenomenon has been described primarily in association with oxygen consumption by the increased numbers of hypermetabolic leukocytes in various types of leukaemia 2–5 and has been termed leukocyte larceny 6. Recognising this pseudohypoxaemia avoids errors in the interpretation of results and prescription of inappropriate diagnostic and therapeutic interventions 7. True oxygenation status can be ascertained with pulse oximetry, correction of hypoxaemia by the addition of potassium cyanide (KCN) to the blood specimen or continuous blood gas analysis 4–6.
In the present report, a case of polycythaemia vera (PV), extreme thrombocytosis, normal leukocyte counts and arterial hypoxaemia in the absence of clinical, radiological or physiological evidence of lung disease is described. The pseudohypoxaemia was confirmed by the addition of KCN to the blood specimen, and became less significant after successful reduction of platelet counts following myelosuppressive chemotherapy. This case suggests that pseudohypoxaemia due to the in vitro consumption of oxygen by significantly elevated numbers of platelets should be included in the differential diagnosis of patients with extreme thrombocytosis being evaluated for arterial hypoxaemia.
CASE REPORT
A 72-yr-old female, who never smoked tobacco, was evaluated at the Cleveland Clinic (Cleveland, OH, USA) for unexplained hypoxaemia on arterial blood gas (ABG) analysis. Her history had begun 3 months previously, when she underwent complete blood count analysis for symptoms of fatigue, revealing a leukocyte density of 8.3×103 leukocytes·μL−1 (normal 4–11×103 leukocytes·μL−1), a haematocrit of 56% (normal 37–47%), a haemoglobin concentration of 18.7 g·dL−1 (normal 12–16 g·dL−1) and platelet density of 2,168×103 platelets·μL−1 (normal 150–350×103 platelets·μL−1). Radioactive chromium-51-labelled red blood cells (RBCs) revealed an increased RBC mass of 38 mL·kg−1 (normal <32 mL·kg−1) and reduced serum erythropoietin levels of 4 mU·mL−1 (normal 5–25 mU·mL−1). ABG analyses performed in room air (table 1⇓) identified severe arterial hypoxaemia, with a Pa,O2 of 6.2 kPa (47 mmHg; normal 10.6–13.3 kPa (80–100 mmHg)).
Comparison of platelet counts and oxygen measurements at various times before and after phlebotomy and cytoreductive chemotherapy
Peripheral blood smears demonstrated increased numbers of erythrocytes with normal morphology along with several normoblasts. Leukocyte numbers were normal without suggestions of cytological atypia. There was thrombocytosis, and giant and hypogranular platelet forms were occasionally observed. Bone marrow biopsy showed hypercellularity with trilineage hyperplasia demonstrating hyperplastic normoblastic erythropoiesis, maturing granulopoiesis without dysplasia and increased megakaryopoiesis with several hyperlobulated megakaryocytes. There was also evidence of intravascular haematopoiesis and absent bone marrow iron stores, and there were no findings of fibrosis. These features were suggestive of the polycythaemic phase of PV.
Despite the bone marrow findings and low serum erythropoietin levels, further testing was conducted in order to identify the aetiology of hypoxaemia, since concerns regarding secondary erythrocytosis existed. Chest radiography and contrast-enhanced computed tomography of the chest, abdomen and pelvis did not identify any abnormalities. Pulmonary function tests revealed normal findings and a 3% shunt fraction (normal <5%) was obtained from ABG measurements using the 100% oxygen method. Transthoracic bubble-contrast echocardiography identified normal left and right ventricular function without suggestions of pulmonary hypertension or intracardiac shunting. In order to rule out a high-affinity haemoglobinopathy, measurement of the Pa,O2 corresponding to an arterial oxygen saturation (Sa,O2) of 50% gave a value of 3.47 kPa (26.1 mmHg; normal 3.15–3.95 kPa (23.7–29.7 mmHg)). The patient was sent to the Cleveland Clinic for further evaluation.
The initial evaluation revealed an elderly female with normal vital signs and an Sa,O2 measured by pulse oximetry (Sp,O2) of 98%. On physical examination, there was splenomegaly that extended 3 cm below the costal margin, no cyanosis, and normal heart and lung tones on auscultation. The ABG analyses were repeated with simultaneous pulse oximetry (table 1⇑) and the results corroborated previous findings. ABG analyses were repeated after incubating the sample with KCN (1 mM final concentration) due to the discrepancy between Sp,O2 and Sa,O2, and normal Pa,O2 and Sa,O2 were demonstrated (table 1⇑), thereby establishing the initial values as pseudohypoxaemia. Pulse oximetry was prescribed in order to further monitor the patient’s oxygenation status.
Treatment for PV was instituted utilising phlebotomy and myelosuppressive therapy with hydroxyurea. On returning 6 weeks after treatment initiation, the patient noted resolution of fatigue and the haematocrit and platelet counts were reduced to 46% and 985×103 platelets·μL−1, respectively. Pulse oximetry continued to give an Sp,O2 of 98%, and repeat ABG analyses showed an increase in Pa,O2 and Sa,O2 (table 1⇑). At her 20-week visit, the haematocrit and platelet counts were 41% and 721×103 platelets·μL−1, respectively, and ABG analyses showed further increases in Pa,O2 and Sa,O2 towards normal values (table 1⇑; fig. 1⇓).
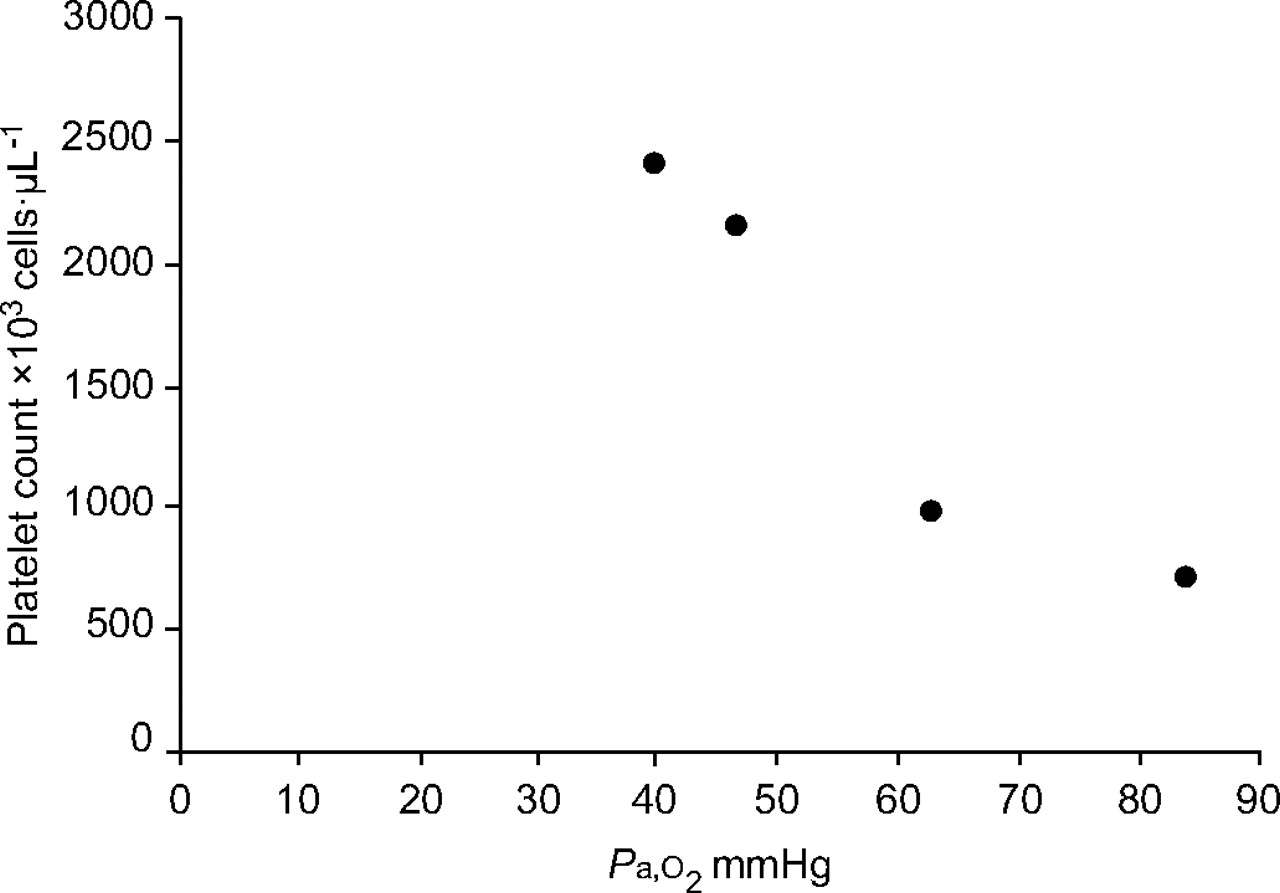
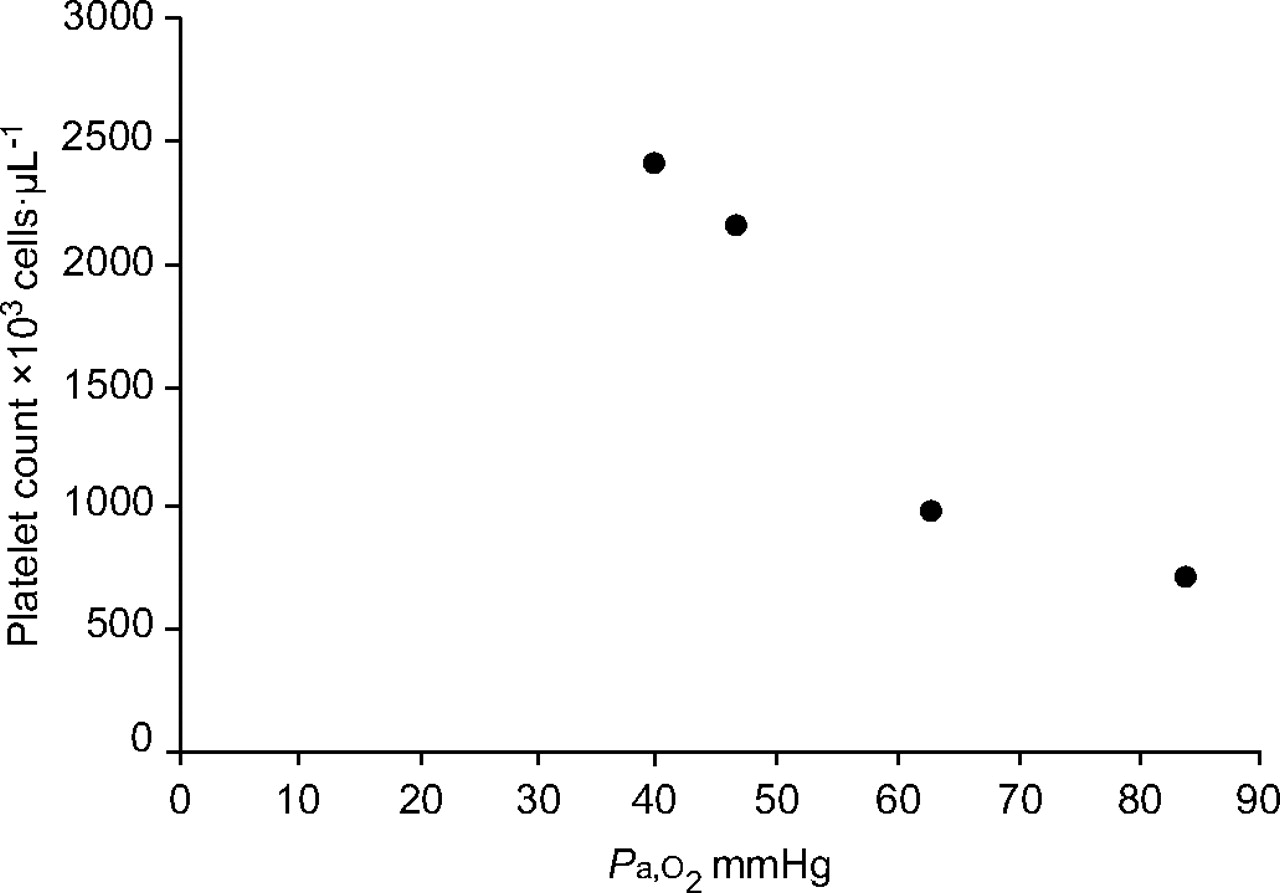{kind=link}
Relationship of arterial oxygen tension (Pa,O2) to platelet count. Platelets were anticoagulated with EDTA. 1 mmHg = 0.133 kPa.
DISCUSSION
In the original description of Hess et al. 1, the mean leukocyte and platelet counts that demonstrated the rapid fall in Pa,O2 of arterial blood stored in a syringe at room temperature were 117×103 cells·μL−1 and 331×103 cells·μL−1, respectively. It was noted that the type and maturity of the proliferating leukocytes appeared to be important in this rate of fall in Pa,O2. Since then, several case reports 2–6 have described this phenomenon of leukocyte larceny in various types of leukaemia, based on the postulation that primitive leukaemic cells exhibit higher metabolic rates and cause larger drops in Pa,O2 than do normal leukocytes 1, 6.
Reticulocytes, platelets and leukocytes are among the constituents of blood that affect Pa,O2 in shed blood, since oxygen consumption by mature erythrocytes and plasma is negligible, with leukocytes and platelets accounting for most of this phenomenon 1, 6, 8, 9. In 1911, Onaka 10 was the first to demonstrate that respiration occurred in plasma after the erythrocytes and leukocytes had been spun down, and correctly attributed this oxygen consumption to blood platelets. Since then, the concept of platelet function has dramatically evolved from that of artefacts and organisms in blood to their being complex integral cells that utilise both aerobic and anaerobic metabolic pathways to generate sufficient amounts of adenosine triphosphate (ATP) for optimal participation in various phases of haemostasis 11, 12. This intimate coupling of energy metabolism with stimulation and execution of platelet responses, as well as the significantly elevated turnover of cytoplasmic ATP compared with that of most other cells, results in the elevated oxygen consumption of these tiny cells 12–14.
In 1951, DeWardener and Young 15 first studied the oxygen consumption of blood in PV and noted increased oxygen utilisation, which affected the estimation of Sa,O2. They demonstrated that this increased in vitro oxygen consumption was directly proportional to the number of circulating leukocytes, with a mean±sd utilisation of 14.4±4.9 mL O2·100 mL−1 blood·24 h−1 (normal 5.4±0.5 mL O2·100 mL−1 blood·24 h−1). In this study 15, the mean leukocyte and platelet counts were 17×103 leukocytes·μL−1 and 622×103 platelets·μL−1. Interestingly, one patient had a platelet count of 2,000×103 platelets·μL−1 and consumed 18.8 mL O2·100 mL−1 blood·24 h−1. This value remained elevated at 10.8 mL O2·100 mL−1 blood·24 h−1 despite washing out the leukocytes and erythrocytes, suggesting considerable oxygen consumption by the markedly elevated platelet counts 15. In 1968, Kitchens and Newcomb 12 studied normal platelet respiration and found that oxygen consumption was directly proportional to the number of platelets in the density range 40–400×103 platelets·μL−1. They also evaluated the rate of oxygen consumption by platelets from normal donors and from patients with various haematological disorders and obtained similar values 12.
With the advent of pulse oximetry, the problem of pseudohypoxaemia can be circumvented 16. Pulse oximetry measures the in vivo percentage of functional haemoglobin combined with oxygen based on the principle that oxyhaemoglobin and deoxyhaemoglobin absorb light over a range of wavelengths between their peak absorption spectra of 660 nm and 940 nm, respectively. In the present patient, a pronounced discrepancy between the Sa,O2 derived from ABG analyses and the Sp,O2 was observed when platelet counts were as high as 2,425×103 platelets·μL−1. Following successful reduction of platelet counts to 721×103 platelets·μL−1 with phlebotomy and hydroxyurea chemotherapy, there was better correlation between the Sp,O2 and Sa,O2 (table 1⇑). Metabolic inhibitors of cellular respiration, such as KCN, have been shown to immediately inhibit oxygen consumption by platelets to 14% of normal at concentrations of 1 mM 12, 17. This was demonstrated in the present patient by the normalisation of Pa,O2 and Sa,O2 after the addition of KCN, and helped to establish the diagnosis of pseudohypoxaemia.
Pulmonary complications causing hypoxaemia are uncommon in PV and, when they occur, are usually caused by either infections or thromboembolic events 18, 19. Other rare complications include pulmonary or pleural extramedullary haematopoiesis and pulmonary arterial hypertension 19, 20. These complications can easily be excluded by corroborating clinical findings with chest imaging and echocardiographic results. Although secondary erythrocytosis is more common than PV, decreased serum erythropoietin levels accompanied by characteristic bone marrow biopsy features are highly suggestive of PV, even in the presence of arterial hypoxaemia. Nowadays, the diagnosis can be greatly enhanced by performing cytogenetic studies for the JAK2V617F mutation, although this was not undertaken in the present case 21. In the present patient, realisation of this would have limited subsequent tests towards potential pulmonary complications of PV and not towards an exhaustive battery of studies for the evaluation of the various causes of secondary erythrocytosis.
In conclusion, although secondary erythrocytosis due to hypoxaemia is more common than polycythaemia vera and patients with polycythaemia vera may show hypoxaemia secondary to pulmonary complications, caution is suggested with regards to relying on arterial blood gas determination alone for the assessment of true oxygenation status in patients with polycythaemia vera and extreme thrombocytosis, especially with platelet counts of >2,000×103 platelets·μL−1, since spurious hypoxaemia due to oxygen consumption can create difficulty in the interpretation of results. The increased rate of oxygen consumption in these patients is most probably due to elevated numbers of platelets rather than a hypermetabolic clone of malignant cells 12. In this context, pulse oximetry can be a useful tool for establishing and further monitoring true oxygenation status. Metabolic inhibitors of platelet respiration, such as potassium cyanide, can also be helpful in establishing the diagnosis of pseudohypoxaemia.
Statement of interest
None declared.
- Received April 3, 2007.
- Accepted June 28, 2007.
- © ERS Journals Ltd
References










