





Abstract
Patients with acute pulmonary embolism (PE) presenting with haemodynamic instability have the worst prognosis. However, what is understood by haemodynamic instability has not been clearly defined.
The Registro Informatizado de la Enfermedad Tromboembólica (RIETE) is an ongoing registry of consecutive patients with symptomatic, objectively confirmed, acute deep vein thrombosis or PE. The present authors compared the predictive value of a systolic blood pressure (SBP) value of <100 mmHg and <90 mmHg and the shock index (cardiac frequency divided by SBP) on 30-day mortality in consecutive patients with PE.
As of May 2006, 6,599 patients with PE were enrolled in the study. Of these, 417 (6.3%) died within 30 days: 153 of the initial PE, 29 of recurrent PE and 235 due to other causes. Of the 417 individuals who died, 127 (30%) had a positive shock index, 60 (14%) had SBP <100 mmHg and 33 (7.9%) had SBP <90 mmHg. On multivariate analysis any of the three parameters were independently associated with an increased mortality. The shock index had a higher sensitivity (30.5 versus 14.4 and 7.9% for SBP <100 mmHg and <90 mmHg, respectively) but lower specificity (86.3 versus 93.0 and 96.6).
All three measures of haemodynamic instability are independent predictors of 30-day mortality. However, while the shock index had the highest sensitivity, a systolic blood pressure value <90 mmHg had the highest specificity.
The Seventh American College of Chest Physicians consensus guidelines 1 recommend initial therapy with heparin for patients with acute nonmassive pulmonary embolism (PE), and suggest the use of thrombolytic therapy for those who are haemodynamically unstable. The British Thoracic Society (BTS) guidelines for the management of acute PE 2 recommend outpatient treatment for patients who are clinically stable. The most important criterion to characterise acute PE as massive is systemic arterial hypotension 3; however, this term is not clearly defined in the literature. Indeed, definitions for haemodynamic instability or massive PE varied among the studies: some used the criterion of a systolic blood pressure (SBP) value <90 mmHg 4, 5; others used SBP <100 mmHg 6–10; and others used the shock index (cardiac frequency divided by SBP) 11. In some studies no definition was provided.
The Registro Informatizado de la Enfermedad Tromboembólica (RIETE) initiative is an ongoing, international (Spain, France, Italy, Israel and Argentina), multicentre, prospective registry of consecutive patients presenting with symptomatic acute venous thromboembolism (VTE) confirmed by objective tests 12–16. The aim of the present study was to compare the predictive value of the three clinical parameters (shock index, SBP <100 mmHg and SBP <90 mmHg) on 30-day mortality in all patients with acute PE.
PATIENTS AND METHODS
Patient entry criteria
Participating hospitals in the RIETE Registry (see Acknowledgements) prospectively enrol consecutive patients with symptomatic, acute deep vein thrombosis (DVT) or PE, confirmed by objective tests, as previously reported. All patients provided oral consent to participate in the Registry, according to the requirements of the ethics committee within each hospital.
Study end-points
The primary end-point was defined as a 1-month mortality. SBP and cardiac frequency were measured at presentation to the emergency department, and the shock index (cardiac frequency divided by SBP) was calculated in all PE patients for further stratification. A positive shock index was defined as ≥1 (haemodinamically unstable patients) and a negative shock index as <1 (haemodinamically stable patients).
Study variables and definitions
The following parameters were recorded: baseline characteristics; clinical status, including any coexisting or underlying conditions, such as chronic heart or lung disease; risk factors for PE; type and dose of treatment received upon PE diagnosis; and outcome during the first 30 days of therapy. Immobilised patients are defined in the present analysis as nonsurgical patients who had been immobilised (i.e. total bed rest with bathroom privileges) for ≥4 days in the 2-month period prior to PE diagnosis. Surgical patients are defined as those who had undergone an operation in the 2 months prior to VTE diagnosis. Creatinine clearance was estimated with the formula by Cockcroft and Gault 17. The first creatinine measured after PE diagnosis was used to calculate creatinine clearance. The causes of death were determined by the attending physicians. In case of doubt, the case report was addressed to the Adjudication Committee of the RIETE Registry.
Statistical analysis
A p-value <0.05 was considered to be statistically significant. First, the influence of a number of variables on the risk of 1-week and 30-day mortality was tested by bivariate analysis with Chi-squared test. Candidate variables were based on published literature. Multivariate analysis was carried out using a logistic regression analysis in the former case and a Cox proportional hazard analysis in the latter, in order to identify predictors of mortality and the independence of the three variables. Then, a receiver operating characteristic (ROC) curve analysis was performed 18. Finally, the sensitivity, specificity, and positive and negative predictive values were compared in order to assess the accuracy of the three variables to predict mortality.
RESULTS
As of May 2006, 6,599 consecutive patients with acute, symptomatic PE had enrolled in RIETE: 3,042 males and 3,557 females, aged 14–99 yrs (mean 68 yrs). PE diagnosis was confirmed in 4,138 patients with a positive computed tomography scan, 2,801 with a high-probability ventilation–perfusion lung scan, 69 with a positive angiogram, 36 with visualisation of a thrombus on the echocardiogram and 124 patients with intermediate-probability lung scan plus evidence of DVT in the lower limbs.
A total of 417 (6.3%) patients died during the first 30 days. The causes of death were: the initial PE event in 153 (37%) patients; recurrent PE in 29 (7.0%); and other causes in 235 (56%) patients. Of the 417 patients who died, 127 (30%) had a positive shock index, 60 (14%) had SBP <100 mmHg and 33 (7.9%) had SBP <90 mmHg.
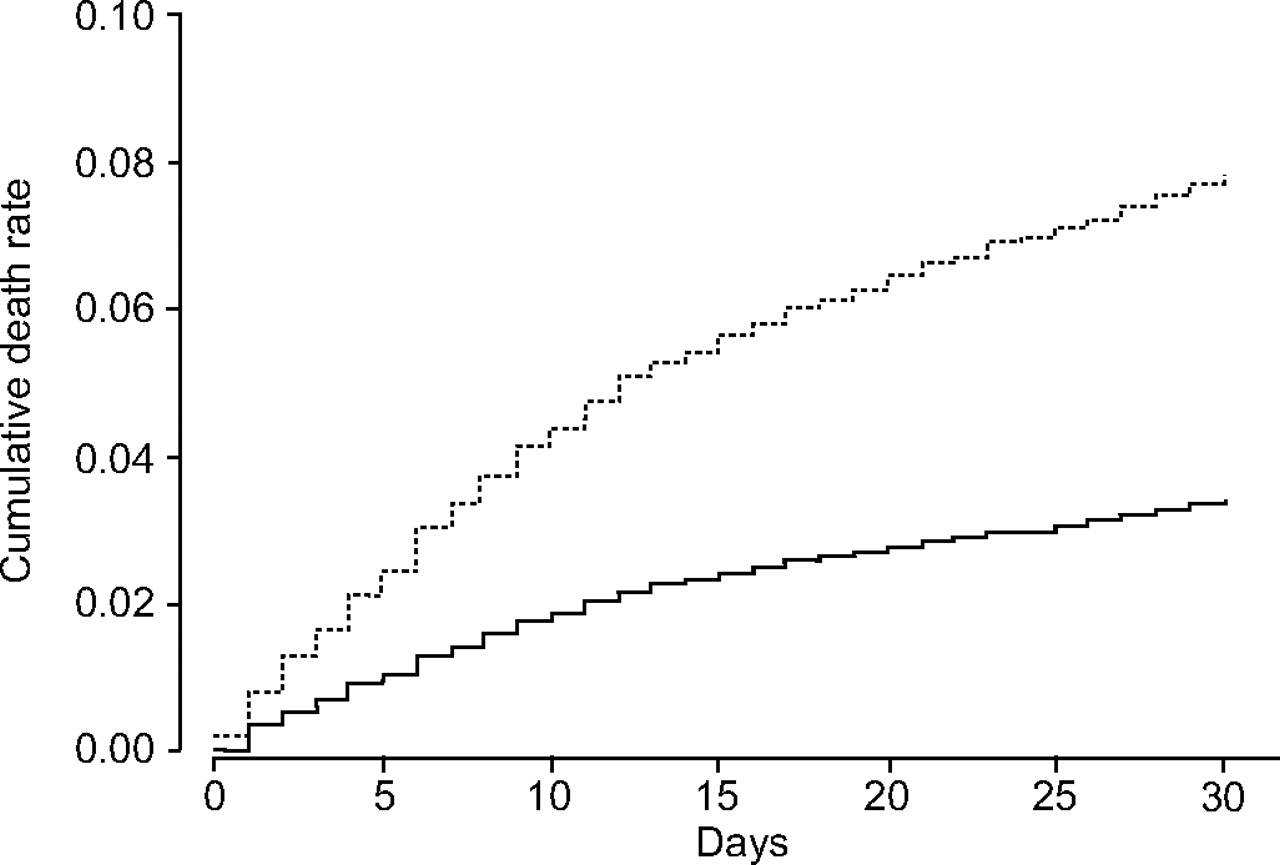
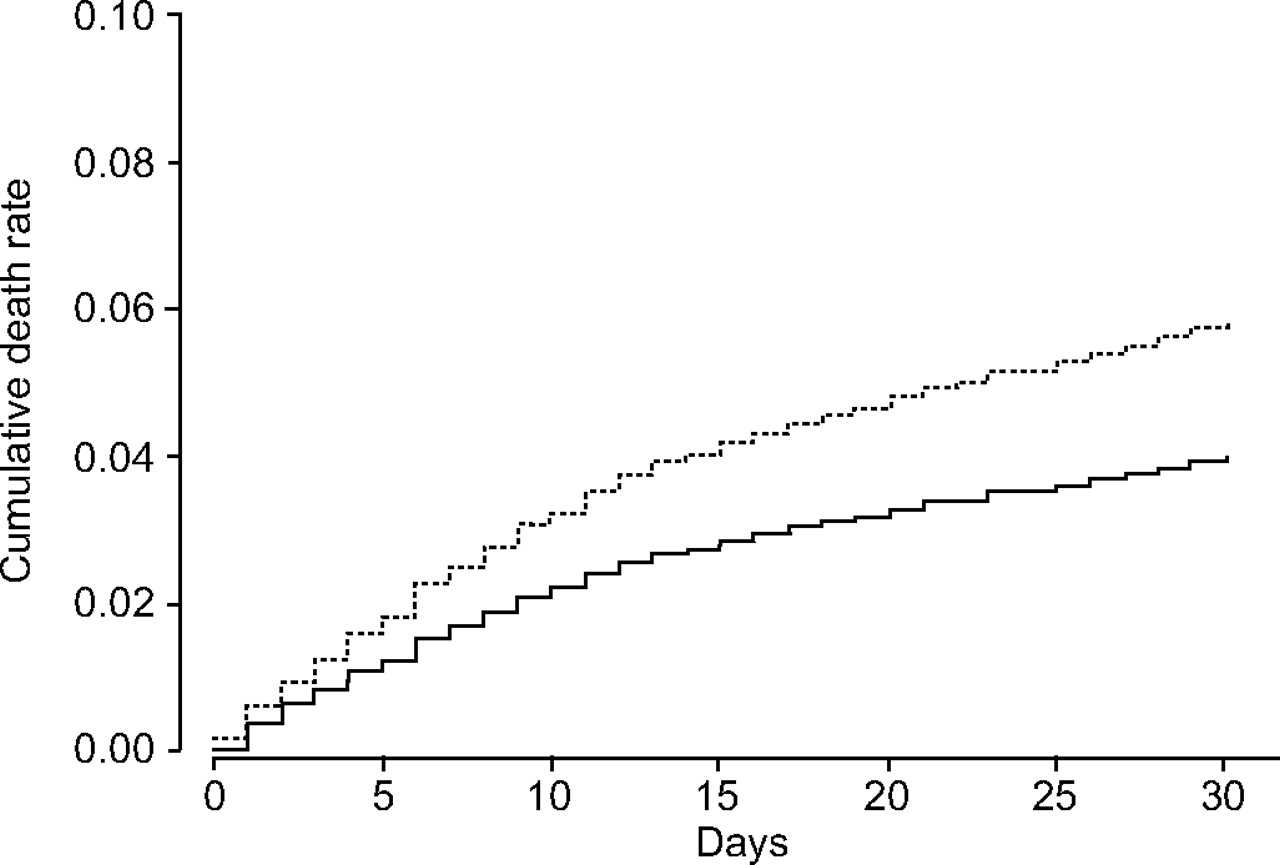
The patients who died were significantly older, more often in-patients and weighed less than those who survived (table 1⇓). More often they also had cancer, immobility for ≥4 days, renal insufficiency, chronic heart failure or recent major bleeding, but less often, a prior episode of VTE or recent surgery. As for their clinical presentation, patients who died were more often those who had tachycardia, hypotension, atrial fibrillation or hypoxaemia at presentation. On multivariate analysis, the hazard ratios (95% confidence interval (CI)) for 1-month mortality were 2.3 (1.5–3.6) for positive shock index, 1.6 (1.0–2.5) for SBP <100 mmHg and 1.7 (0.9–3.2) for SBP <90 mmHg, as shown in table 2⇓ and in figures 1⇓–⇓3⇓.
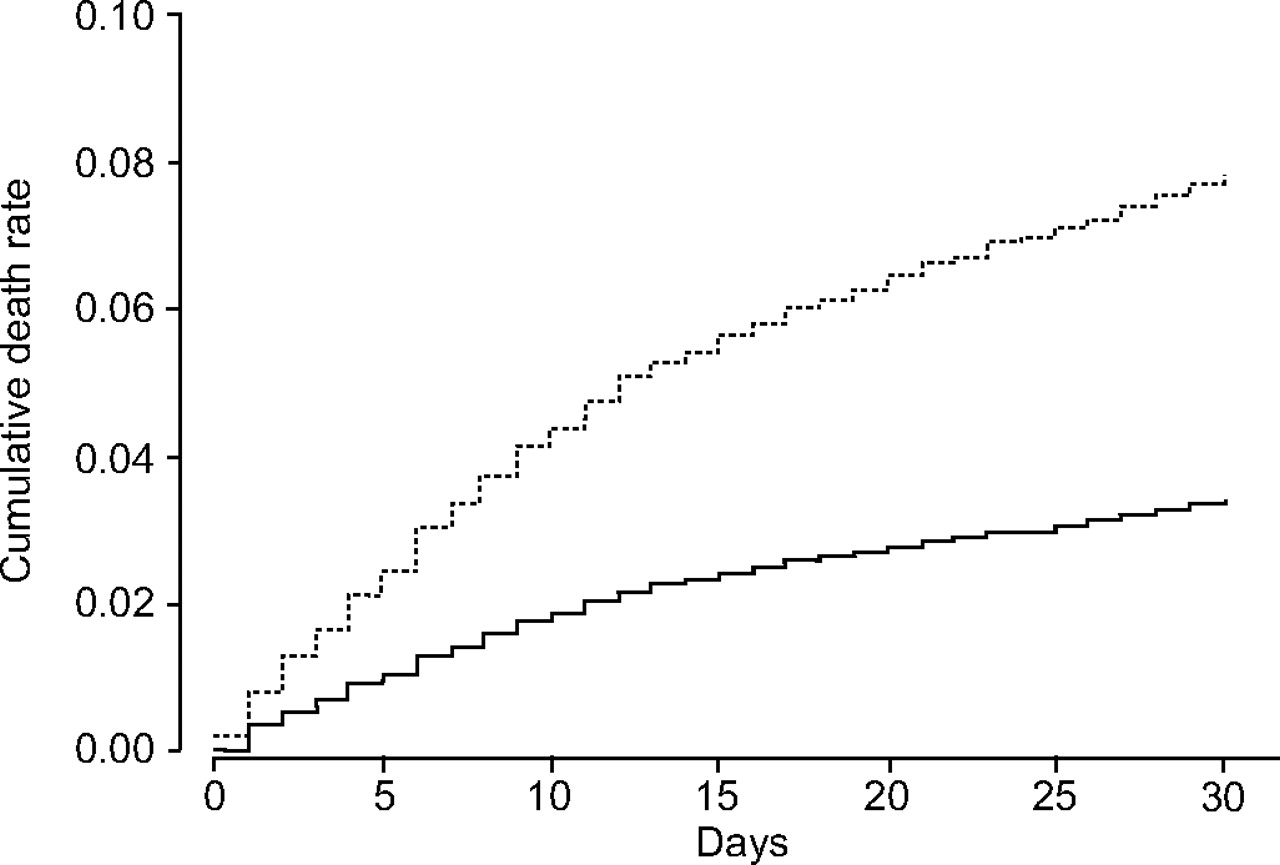
Kaplan–Meier survival curves using the Cox model for patients with (·······: shock index ≥1.0) and without (——: shock index <1.0) positive shock index.

Kaplan–Meier survival curves using the Cox model for patients with (·······) and without (——) systolic blood pressure <100 mmHg.

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curves using the Cox model for patients with (·······) and without (——) systolic blood pressure <90 mmHg.
Clinical characteristics and treatment details of 6,599 patients with acute pulmonary embolism according to 30-day mortality
Multivariate analysis(Cox proportional hazard models) on the risk of death at 30 days
The shock index had a higher sensitivity than either SBP <100 mmHg or SBP <90 mmHg but a lower specificity, as shown in table 3⇓. There were no significant differences in sensitivity, specificity and positive or negative predictive value, whether the cause of death was the initial PE event, recurrent PE or other reasons (table 3⇓). The area under the ROC curve (95% CI) was 0.79 (0.77–0.82) for the positive shock index, 0.78 (0.75–0.80) for SBP <100 mmHg and 0.77 (0.75–0.80) for SBP <90 mmHg.
Predictive value of the three variables in the prediction of 30-day mortality
DISCUSSION
The present data, obtained from a large prospective series of consecutive patients in the RIETE Registry, confirm that any of the three mentioned parameters (shock index, SBP <100 mmHg and SBP <90 mmHg) are independent predictors of 30-day mortality in patients with acute PE. The observation that haemodynamic instability at presentation predicts an adverse outcome in acute PE is certainly not new but confirms previous data from recent decades 3–11. In the present authors’ experience, the three shock parameters examined are equally good (or equally inadequate) in predicting an adverse outcome, since they all appear significant in the Cox model but do not possess high sensitivity or specificity. However, some differences were found among them in terms of sensitivity and specificity that may be relevant in clinical practice.
Two of the most controversial and unsolved issues in the treatment of acute PE are the selection of patients for outpatient therapy and the role of thrombolysis. There is growing evidence that outpatient therapy with low-molecular weight heparin is effective and safe for most patients with PE 19, 20. Based on this evidence, the BTS guidelines for the management of acute PE 2 recommend outpatient treatment for clinically stable patients. However, this was not defined. Of the 417 patients who died in the current series, 30% had a positive shock index and 7.9% had SBP <90 mmHg. This higher sensitivity of the shock index makes it more useful when trying to identify a subgroup of patients at low risk of death. Of course, the shock index alone is not sensitive or specific enough to decide which candidates should receive home therapy but, combined with other independent variables (i.e. age, body weight, immobility, cancer, hypoxaemia or renal insufficiency), it should be preferred over SBP alone.
In the other extreme, the benefit of thrombolysis or other aggressive therapies over heparin appears only in PE patients at high risk for death 21–27. However, since thrombolytic therapy doubles the risk for major bleeding 21, careful and rapid risk assessment is paramount in selecting the appropriate treatment strategy in these patients. In the current study, only 3.4% of those who survived had SBP <90 mmHg, while 14% had a positive shock index. In the present authors’ opinion, this higher specificity of SBP <90 mmHg would better help identify the subgroup of patients at high risk for death.
The present study has some limitations. First, the 6.3% death rate in the current series is slightly lower than the 5.0–15% rates observed in other studies 6, 7, 11, 28, 29. These differences may be attributed to either different observation periods (30 days in the present study) or the need for objective confirmation of PE diagnosis in RIETE. Some patients with severe PE may have died before getting an objective confirmation or were not enrolled as they could not give informed consent. Secondly, the shock index, as a ratio, is subject to many problems (e.g. inappropriate relative bradycardia with a low SBP can still give a patient a positive shock index, clearly undesirable). Thirdly, although the shock index had a higher sensitivity than either of the SBP parameters, it remains quite low (30.5%), and the positive predictive values are very low and very close. Thus, a negative shock index does not guarantee an uncomplicated hospital course since the overall mortality rate at 30 days in these patients was 5.2% (95% CI 4.6–5.8). Physicians should also consider the utility of other methods to detect patients at high risk of dying (i.e. echocardiography, cardiac biomarkers). Finally, as an observational study, RIETE is not designed to answer questions regarding the relative efficacy and safety of different modalities of therapy. Data from the Registry are hypothesis generating and provide feedback from real-world clinical situations which may be of value when designing new randomised clinical studies.
In summary, all three measures of haemodynamic instability are independent predictors of 30-day mortality. This issue is important since these criteria are used when deciding whether a patient with acute pulmonary embolism should be hospitalised or receive thrombolytic therapy. Given their low positive predictive value, they are not particularly predictive of a poor outcome but their absence is highly predictive of a good outcome (given their high negative predictive value). Interestingly, this was true whether the patients died of pulmonary embolism or another cause. Although a shock index of >1 was more sensitive and an systolic blood pressure <90 mmHg more specific, these statistically significant differences were not very important in clinical meaningful terms.
Acknowledgments
The members of the RIETE group are as follows.
Spain. Albacete: J.L. Beato (Hospital de Hellín); Alicante: L. Hernández (Hospital General Universitario de Alicante), A. Maestre (Hospital General Universitario de Elche, Elche); Asturias: I. López (Hospital San Agustín, Avilés); Barcelona: C. Falgá (Consorci Hospitalari de Mataró), M. Monreal (Hospital Universitari Germans Trias i Pujol, Badalona), E. Raguer (Hospital de Terrassa), A. Raventos (Hospital Municipal de Badalona), C. Tolosa (Corporació Sanitària Parc Taulí, Sabadell), M. Valdés (Hospital de Viladecans); Cáceres: J.M. Calvo (Hospital Ciudad de Coria), J.F. Sánchez (Hospital San Pedro de Alcántara); Ciudad Real: J. Portillo (Complejo Hospitalario de Ciudad Real); Córdoba: A. Blanco (Hospital Universitario Reina Sofía), L. López (Hospital Provincial Reina Sofía); Cuenca: J.A. Nieto (Hospital General Virgen de la Luz, Cuenca); Gerona: F. García-Bragado (Hospital Universitari Dr Josep Trueta), S. Soler (Hospital Sant Jaume, Olot); Granada: J.I. Arcelus, I. Casado (Hospital Universitario Virgen de las Nieves); Logroño: M. Barrón (Complejo Hospitalario San Millán y San Pedro); Madrid: R. Barba (Fundación Hospital Alcorcón), C. Fernández-Capitán (Hospital Universitario La Paz), J. Gutiérrez (Hospital Monográfico Asepeyo, Coslada), D. Jiménez (Hospital Ramón y Cajal), O. Madridano (Hospital Universitario La Paz), N. Ruiz-Giménez (Hospital Universitario de la Princesa); Lugo: R. Rabuñal (Complexo Hospitalario Xeral-Calde); Málaga: R. Guijarro, J.J. Martín (Hospital General Universitario Carlos Haya), M. Guil (Hospital Comarcal de la Axarquía, Vélez-Málaga); Murcia: J. Trujillo (Hospital General Santa María del Rosell, Cartagena); Pamplona: R. Lecumberri (Clínica Universitaria de Navarra), M.T. Orue (Hospital de Navarra), G. Tiberio (Hospital Virgen del Camino); Pontevedra: J. Montes (Hospital de Meixoeiro, Vigo), M.J. Núñez (Hospital Comarcal do Salnés, Vilagarcía de Arousa); Santander: R. Valle (Hospital Sierrallana, Torrelavega); Sevilla: R. Otero (Hospital Virgen del Rocío); Tarragona: L. Font (Hospital de Tortosa Vergel de la Cinta, Tortosa); Teruel: J. Vela (Hospital de Alcañiz); Valencia: F. López (Hospital Arnau de Vilanova, Arnau de Vilanova), M.D. Naufall, J.A. Todolí (Hospital Universitario La Fe), P. Román (Hospital General de Requena); Vizcaya: F. Uresandi (Hospital de Cruces); Zaragoza: F. Conget (Hospital Clínico).
France. Saint-Etienne: P. Mismetti, K. Rivron-Guillot (Hospital Bellevue).
Italy. Genoa: R. Poggio (Ospedale Galliera); Naples: P. Di Micco, M.T. Iannuzo (Ospedale Buonconsiglio Fatebenefratelli); Padua: P. Prandoni (Clinica Medical Il University of Padua); Parma: R. Quintavalla (Azienda Ospedaliera Universitaria); Rimini: E. Tiraferri (Ospedale Infermi).
The authors would like to thank S. Ortiz (Universidad Autónoma de Madrid and S&H Medical Science Service; both Madrid, Spain) for statistical analysis of the data and the Registry Coordinating Centre (S&H Medical Science Service) for logistic and administrative support.
- Received June 14, 2007.
- Accepted August 22, 2007.
- © ERS Journals Ltd
References










