





Figures
- Fig. 1—
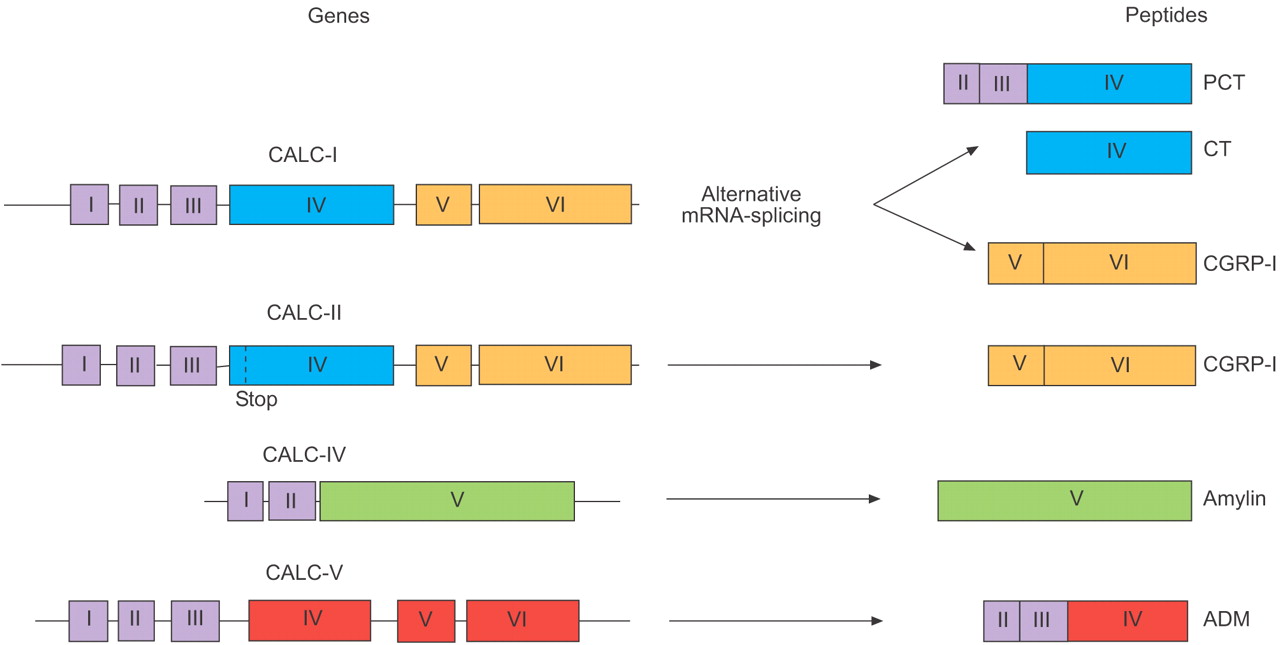
CALC genes and the calcitonin (CT) superfamily of peptides. Members of the CT gene peptide superfamily are prototypes of hormokines but may serve as a model for the better understanding of the pluripotency of other molecules (hormones and cytokines) and cells. The CALC-I gene gives rise to two different so-called mature peptides: CT and CT gene-related peptide (CGRP)-I. Circulating procalcitonin (PCT) consists of 114 amino acids, in which the mid-portion consists of the 33-amino acid immature CT. No CT is expressed from CALC-II due to a stop codon in exon IV. CALC-III (not shown) is a nontranslated pseudogene. Amylin is also referred to as islet amyloid polypeptide. The amino-terminal peptides of adrenomedullin (ADM), encoded by exons II and III, also have some bioactivity (e.g. pro-ADM amino-terminal 20 peptide, PAMP). The common structural features and marked amino acid homology within the CT peptide superfamily suggest gene duplication of a common ancestral gene.
- Fig. 2—
Schematic representation of the CALC-I gene. The presence of a microbial infection-specific transcriptional activation in many, if not all, cell types has been postulated. The presence of one or several stimulus-specific sepsis-response elements in the promoter could explain the specific transcriptional activation found in microbial infections. Calcitonin (CT) mRNA is the default splicing variant. CT gene-related peptide (CGRP) mRNA is spliced in the presence of a sepsis-inducible ubiquitous repressor. MISRE: microbial infection-specific response elements; UTR: untranslated region; PCT: procalcitonin; RAMP: receptor activity-modifying protein.
- Fig. 3—
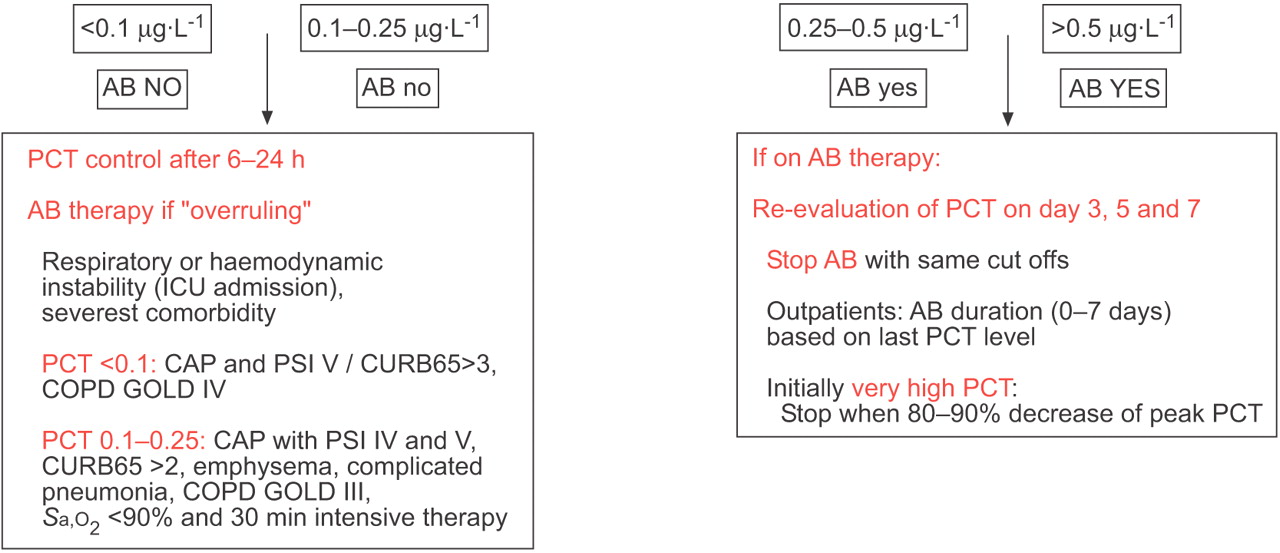
Procalcitonin (PCT)-guided antibiotic (AB) stewardship. Cut-off ranges of PCT were derived by calculating multilevel likelihood ratios and optimised for the setting of an emergency room and hospital. The use of a sensitive assay (Kryptor® PCT; Brahms, Hennigsdorf, Germany) assured adequate sensitivity. Briefly, use of antibiotics was more or less discouraged (<0.1 μg·L−1 or <0.25 μg·L−1) or encouraged (>0.5 μg·L−1 or >0.25 μg·L−1) based on a range of PCT levels. The same cut-offs were used regardless of whether or not patients had been pre-treated with antibiotics prior to admission to the emergency department. In patients with very high PCT values on admission (e.g. >10 μg·L−1), discontinuation of antibiotic therapy was encouraged if levels decreased to <80–90% of the initial value. In patients with an initial PCT level >10 μg·L−1 and smaller reductions during follow-up, continuation of antibiotic treatment was encouraged. Re-evaluation of the clinical status and measurement of serum PCT levels was recommended after 6–24 h in all persistently sick and hospitalised patients in whom antibiotics were withheld. As indicated above, the PCT algorithm should be overruled in patients with immediately life-threatening disease. However, in these patients, despite the immediate administration of intravenous broad-spectrum antibiotic therapy, a much more likely noninfectious differential diagnosis responsible for the critical illness must be strongly considered and actively sought, especially if PCT levels remain very low during follow-up. Physicians were advised that persistently elevated PCT levels may indicate a complicated course, while PCT levels may remain relatively low in localised infections (e.g. empyema or abscess). PCT levels were reassessed on days 3, 5 and 7 in hospitalised patients with ongoing antibiotic therapy, and in patients showing a worsening or delayed recovery of signs and symptoms, and antibiotic was discontinued using the PCT cut-offs defined above. For antibiotic stewardship in a medical or, especially, surgical intensive care unit (ICU), modified cut-off ranges might be necessary. Because mean PCT levels are increased in a cohort of critically ill patients as compared with patients in an emergency room or hospital setting, the optimal thresholds of the cut-off range are likely to be higher, especially in a immediately post-operative or post-traumatic situation. CAP: community-acquired pneumonia; PSI: pneumonia severity index; CURB65: severity score for CAP based on confusion, urea nitrogen, respiratory rate, blood pressure and age ≥65 yrs; COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung Disease staging system for COPD; Sa,O2: arterial oxygen saturation.
- Fig. 5—
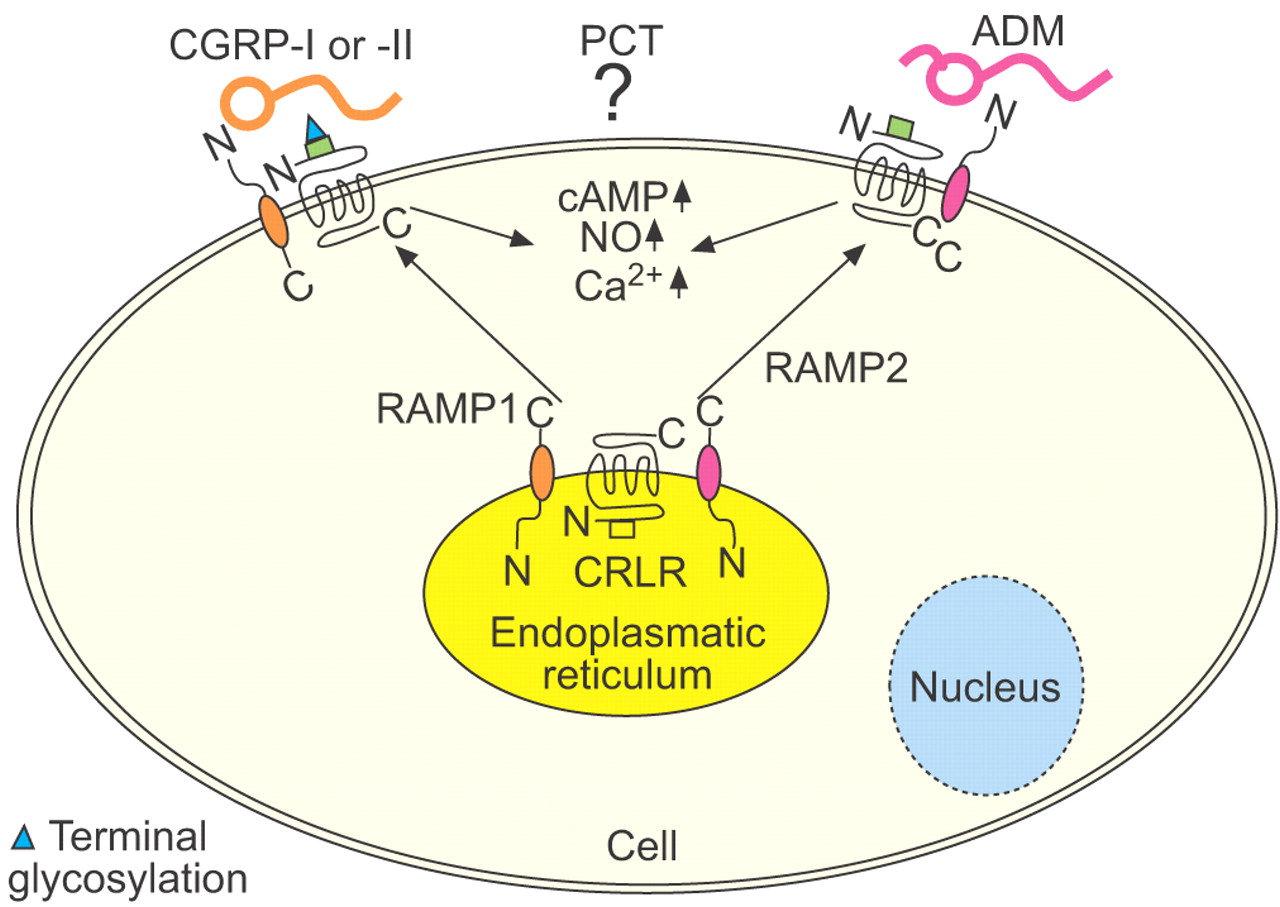
Receptors for calcitonin (CT) peptides. Based on the structural homologies, different CT peptides have overlapping bioactivities, which they exert by binding to the same family of receptors 16. There are two subgroups of these G protein-coupled receptors with seven transmembrane domains: CT receptors and CT receptor-like receptors (CRLR). Three accessory proteins, which are called receptor activity-modifying proteins (RAMP-1, -2 and -3), act upon these receptors, thus altering their specific responsiveness and ligand affinity, and hence modifying the physiological profile of the CT-peptide superfamily 146. Depending on which of the different RAMPs is associated with the receptor, each member of the CT-gene family of peptides binds with differing affinities. Whether procalcitonin (PCT) and other CT precursor peptides from the other CALC genes are also ligand for these receptors is currently unknown. CGRP: calcitonin gene-related peptide; ADM: adrenomedullin; NO: nitric oxide; N: amino terminal; C: carboxyl terminal.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1—
Trimodal pattern of CALC-I gene expression occurring in neuroendocrine cells, parenchymal cells and monocytes
Thyroid Parenchymal tissue Monocytes mRNA Constitutive Regulated Regulated Protracted, sustained by cytokines and LPS Rapid, transient upon adhesion Detectable after >6 h Detectable after >2 h Protein Regulated Constitutive Constitutive Detectable after >10 h Detectable after >4 h Persistent (>24 h) Transient (<18 h) Tissue mass Low High Low Main function Mature CT, e.g.↓ P-Ca2+ Sepsis-associated PCT increase Local vasodilation (CGRP, PCT?) LPS: lipopolysaccharide; CT: calcitonin; ↓P-Ca2+: lowering of circulating plasma ionised calcium levels; PCT: procalcitonin; CGRP: CT gene-related peptide. Adapted from 3.
- Table 2—
Evidence from intervention studies of respiratory tract infections with procalcitonin(PCT)-guided antibiotic (AB) therapy
ARTI Bronchitis Pneumonia Study ProRESP ProCOLD ProCAP Setting Emergency dept Hospital Design Intervention studies Patients n 243 226 302 Median PCT μg·L−1 0.25 0.1 0.5 AB initiation ↓ % 44 40 14 Duration ↓ 13 to 6 days Hospitalisation % 78 80 97 Adverse events % 10 16 20 In the ProRESP study, PCT guidance reduced AB prescription in 243 patients with lower respiratory tract infections by almost 50% 19. In the ProCAP study, PCT-guided AB duration was shortened by 65% from 12.9 to 5.8 days, with a similar outcome in patients with all severities of community-acquired pneumonia 20. In the ProCOLD study, the current authors demonstrated long-term safety with a similar re-admission rate over 6 months in >200 acute exacerbations of chronic obstructive pulmonary disease with markedly reduced PCT-guided AB use 21. ARTI: acute respiratory tract infection.
- Table 3—
Calcitonin(CT) peptides, as hormokines, are a functional entity
CT CGRPs Amylin ADM Receptor CR CRLR CR CRLR RAMP (2)# 1 1 or 3 2 or 3 Second messenger cAMP, Ca2+ NO ? NO, NF-κB Metabolic effects Insulin resistance – + + – Effect on β-cells ± + ++ – Anorectic ++ + ++ + Gastric protection – ++ + – Effects on calcium/bone ++ ± + ± Inflammatory effects Increase plasma in infections PCT + With insulin + Toxic in sepsis PCT +? – +? Vasodilation ± ++++ ++ ++ Pro-inflammatory ± ++ – + Thermoregulation – + + + Chrono- and ionotropic – ++ ++ + Analgesic ++ – + – Host defence Bactericidal activity ? – – ++ Data represent predominantly experimental results obtained in vitro or in animals (mostly rodents) using supra-physiological dosages. The 114-amino acid form of human procalcitonin (PCT), circulating in high levels during sepsis, is not yet available for experimental purposes. +: positive effect; –: negative effect; ±: mixed effect; +?: questionable positive effect; ?: questionable effect; ++: clear positive effect; ++++: powerful effect. CGRP: CT gene-related peptide; ADM: adrenomedullin; CR: CT receptors; CRLR: CT receptor-like receptors; RAMP: receptor activity-modifying protein; Ca2+: calcium homeostasis NF: nuclear factor. #: not on absolute prerequisite for function of the colcitonin receptor. Compiled and adapted from 2.











Jump To
- Article
- Abstract
- CALCITONIN PEPTIDES ARE PROTOTYPES OF HORMOKINES
- ASSAYS TO MEASURE “PCT”
- PCT IN THE DIAGNOSTIC ASSESSMENT OF SEVERE INFECTIONS
- PCT FOR ANTIBIOTIC STEWARDSHIP OF RESPIRATORY TRACT INFECTIONS
- PCT IN VENTILATOR-ASSOCIATED PNEUMONIA
- BIOMARKERS FOR THE PROGNOSTIC ASSESSMENT OF CAP
- BIOMARKERS FOR PROGNOSTIC ASSESSMENT IN SEPSIS
- THE CENTRAL ROLE OF HORMOKINES IN HOST DEFENCE
- HOW DO HORMOKINES MEDIATE THEIR EFFECTS?
- HORMOKINES AS THERAPEUTIC TARGET IN SEVERE INFECTIONS
- CONCLUSION
- References
- Figures & Data
- Info & Metrics