





Abstract
The aim of the present study was to evaluate airway disease progression assessed by chest radiology, expiratory interrupter resistance (Rint,exp) and spirometry in young children with cystic fibrosis (CF) over a 3-yr period.
Two chest radiographs combined with two Rint,exp measurements were performed with a 3-yr interval in 21 preschool children (age (mean±sd) 3.2±0.9 yrs) and 30 schoolchildren with CF (age 7.2±1.9 yrs). Chest radiographs were scored using five different CF scoring systems and Rint,exp measurements were expressed as height-adjusted Z-scores. Spirometry was assessed in schoolchildren and the results were expressed as a percentage of predicted values.
Chest radiograph scores worsened significantly over the 3-yr period and a tendency towards more pronounced changes was observed, especially for the Wisconsin score, in preschool children. Most preschool and schoolchildren had Rint,exp Z-scores within the normal range at start and follow-up, and the annual change in Rint,exp Z-score was not significant. In schoolchildren, only the forced expiratory volume in one second as a percentage of forced vital capacity declined significantly during the study period.
In summary, in young children with cystic fibrosis, chest radiograph scores worsen significantly over time even while lung function remains stable.
Chronic airway infection and inflammation in cystic fibrosis (CF) lung disease lead to structural lung damage, pulmonary dysfunction and, eventually, to respiratory insufficiency. CF lung disease starts at a very young age and, ideally, treatment should also start at, or even before, the onset of lung disease. Therefore, sensitive measures of structural and functional lung damage are needed to objectively assess lung disease progression and to evaluate the effect of treatment.
Structural lung damage in CF can be assessed by chest radiology and high-resolution computed tomography (HRCT) scanning. An annual chest radiograph and the use of chest radiograph scoring systems are recommended by the European CF Consensus Committee 1, and several different CF chest radiograph scoring systems 2–6 have been developed. In older children with moderate-to-severe CF, there is good correlation between pulmonary function tests (PFTs), especially forced expiratory volume in one second (FEV1), and chest radiograph scores in cross-sectional studies 4, 6, 7. Longitudinal evaluation of bronchopulmonary disease in children with CF using chest radiology showed disease progression from the age of ∼5 yrs, even when spirometry results still remained stable 8–10. However, in preschool children the sensitivity of chest radiographs as a measure of disease progression and the relationship with functional parameters is unclear.
Lung function can be assessed according to PFTs (especially spirometry) and, although FEV1 is still considered the gold standard in daily CF practice, peripheral flows such as mean forced expiratory flow between 25 and 75% of forced vital capacity (FEF25–75%) seem more sensitive in young CF children 11 . Spirometry is feasible in most children aged 4–6 yrs, but standards for quality control are lacking for preschool children 12–14. Therefore, alternative PFTs, such as the expiratory interrupter resistance (Rint,exp) measurement, have been developed for this age group 15–20. Rint,exp measurements can be performed without sedation, are easily applicable in general practice, are effort-independent and reference values for children aged 3–13 yrs are available 18. Rint,exp measurements may be of use in detecting early lung function abnormalities in children with CF. However, data on the value of interrupter resistance (Rint) measurements in CF patients are not conclusive 12, 17, 18, 20 and longitudinal measurements of Rint have never been related to structural damage assessed by chest radiology.
The purpose of the present study was to evaluate the sensitivity of structural and functional parameters of lung disease progression in young children with CF. Disease progression in preschool (aged <5 yrs) and schoolchildren (aged >5 yrs) was studied prospectively using simple chest radiograph scores, Rint,exp measurements and spirometry.
METHODS
Study population
The Utrecht CF Centre of the University Medical Centre Utrecht (Utrecht, the Netherlands), a tertiary academic hospital, uses annual chest radiographs and PFT measurements, including spirometry and Rint,exp measurements, to monitor lung disease in patients with CF.
A total of 21 preschool children and 30 schoolchildren who attended the CF Centre for their annual check-up between April 2002 and June 2003 were studied. A routine chest radiograph and a Rint,exp measurement were performed on the same day both that year and 3 yrs later. All schoolchildren performed spirometry at visits 1 and 2. Measurements were performed when children were clinically stable. Informed consent was obtained from the parents of all participating children.
Chest radiographs
Chest radiographs (anteroposterior and lateral view) were blinded and scored in random order by two different observers (H.G.M. Arets and C.K. van der Ent) according to the following five cystic fibrosis chest radiograph scoring systems: Chrispin–Norman scoring (range 0–38, with 0 as the best score) 2; adjusted Chrispin–Norman scoring (range 0–42, with 0 as the best score) 3; Wisconsin scoring (range 0–100, with 0 as the best score) 4; Northern scoring (range 0–20, with 0 as the best score) 5; and Brasfield (Birmingham) scoring system (range 4–25, with 25 as the best score) 6.The systems score different abnormalities, such as hyperinflation, linear markings, nodular cystic lesions and large lesions (segmental or lobar atelectasis or consolidation). In order to establish intra-observer variability, both observers randomly scored eight chest radiographs for a second time after 3 months. Prior to assessment it was agreed that a cut-off value of 5 for the Wisconsin score and 21 for the Brasfield score would be associated with mild, but potentially irreversible, lung damage 10.
Rint,exp and spirometry
Airway resistance was measured in all children using the MicroRint® (Micro Medical Ltd, Chatham, UK), as described in previous studies 15, 16, 19. A successful Rint,exp measurement consisted of the median Rint,exp value of at least five out of 10 interruptions. Rint,exp was calculated using the back extrapolation technique to t = 0 ms after shutter closure during 100 ms 15, 21. Rint,exp values in children with CF were expressed as height-adjusted Z-scores, using data from a Dutch healthy control population 19.
All schoolchildren performed spirometry at visits 1 and 2 (Masterlab, Hochberg, Germany). Spirometry results were obtained for FEV1, forced vital capacity (FVC), maximal instantaneous forced flow when 50% of the FVC remains to be exhaled (MEF50%), forced expiratory flow at 75% of FVC and FEF25-75%. These results were expressed as a percentage of predicted values using data from Zapletal 22. FEV1 was also expressed as a percentage of FVC (FEV1/FVC). Abnormal lung function was defined as an FEV1 <85% pred.
Lung structure and lung function over time
The average of the chest radiograph scores from the two observers was used. Data obtained at the first visit are reported as chest radiograph1, Rint,exp Z-score1 and PFT1, and at the second visit as chest radiograph2, Rint,exp Z-score2 and PFT2. Δchest radiograph is the annual change for a chest radiograph scoring system (chest radiograph2–chest radiograph1/time interval); ΔRint,exp Z-score is the annual change for Rint,exp Z-score (Rint,exp Z-score2–Rint,exp Z-score1/time interval); and ΔPFT is the annual change for PFTs (PFT2-PFT1/time interval). To compare the annual changes of the five chest radiograph scoring systems, Δchest radiograph was also expressed as a percentage of the maximal obtainable score for that system except for the Brasfield scoring system, since the best score for this system is 25 and the worst score is 4. A positive value for Δchest radiograph indicates an increase in structural abnormalities for all chest radiograph scoring systems except for the Brasfield scoring system, where a negative value for Δchest radiograph indicates an increase in structural abnormalities. A positive value for ΔRint,exp Z-score indicates an increase in resistance and thus a worsening of lung function. A negative value for ΔPFT indicates a decline in lung function.
Statistical analysis
Intra- and interobserver variability of composite chest radiograph scores was calculated using intraclass correlation coefficients. To determine whether chest radiograph scores and/or Rint,exp Z-score and/or PFTs changed significantly over time in preschool and in schoolchildren, paired t-tests were performed for ΔRint,exp Z-score, ΔPFT and Δchest radiograph. Mean differences between the parameters at visits 1 and 2 were expressed as the mean annual decline, calculated by dividing the mean difference by the time interval. The relationships between chest radiographs, Rint,exp Z-scores and PFTs, and between Δchest radiograph, ΔRint,exp Z-score and ΔPFT were evaluated using Spearman correlation coefficients. Finally, changes in chest radiograph scores and Rint,exp Z-score over time were compared between preschool and schoolchildren using SAS PROC mixed models. A p-value <0.05 was considered to be statistically significant. Data are presented as mean±sd.
RESULTS
Study population
Characteristics of the preschool and schoolchildren are shown in table 1⇓. Mild, but potentially irreversible lung damage (Wisconsin score >5, Brasfield score <21) was found at visit 1 in: five (24%) of the 21 preschool children for the Wisconsin score; seven (33%) of the 21 preschool children for the Brasfield score; 12 (40%) of the 30 schoolchildren for the Wisconsin score; and 15 (50%) of the 30 schoolchildren for the Brasfield score.
Patient characteristics of the preschool# and schoolchildren¶ with cystic fibrosis at visits 1 and 2
Most preschool children had Rint,exp Z-scores that were within normal range (mean±2×Z-scores) both at visit 1 (9.5% had a Rint,exp Z-score >2×sd) and at visit 2 (19% had a Rint,exp Z-score >2×sd). In schoolchildren, 13% had a Rint,exp Z-score >2×sd at visit 1 and 23% at visit 2 (figs. 1a⇓ and 1b⇓). Only seven (23%) of the 30 schoolchildren had abnormal lung function (FEV1 <85%) at visit 1.
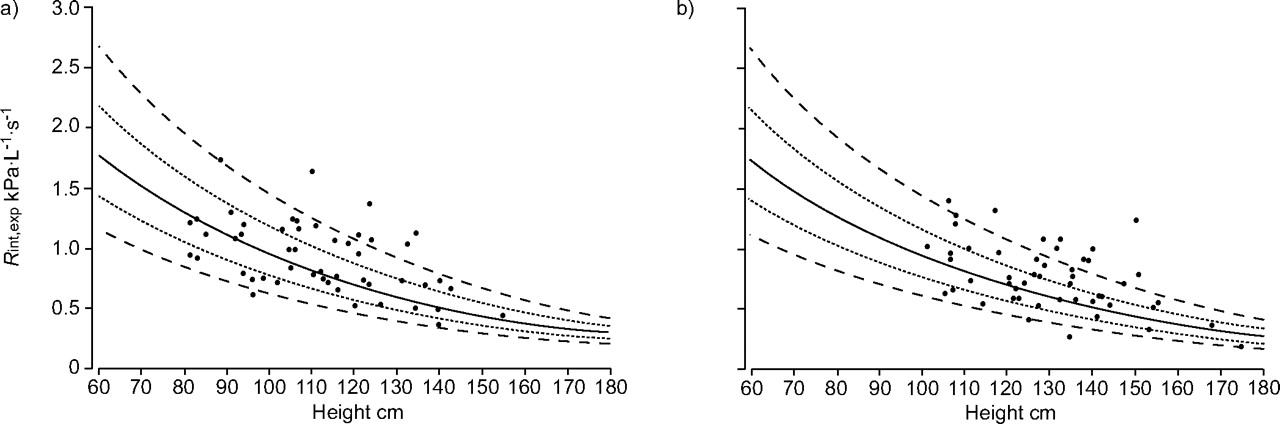
Absolute expiratory interrupter resistance (Rint,exp) values in preschool and schoolchildren with cystic fibrosis compared with the regression line (—: 10 log Rint,exp = 0.645–0.00668×standing height (in cm), showing ±Z-score (·····) and ±2×Z-score lines (----)) of the Dutch healthy control group at a) visit 1 and b) visit 2.
Reproducibility of the scoring systems
Intraclass correlation coefficients (r-values) between both observers for the different scoring systems were moderate (r ranging 0.60–0.65). Intraclass correlation coefficients for intra-observer variability were moderate to good (H.G.M. Arets varying from r = 0.57 for the Northern scoring system to r = 0.88 for the adjusted Chrispin–Norman scoring system, and C.K. van der Ent varying from r = 0.78 for the adjusted Chrispin–Norman scoring system to r = 0.91 for the Wisconsin scoring system).
Lung structure over time
All chest radiograph scores except the Northern score worsened significantly over time in preschool children (p<0.05 for the Wisconsin score and p<0.001 for all the other scores; table 2⇓). Figure 2⇓ shows the changes in Chrispin–Norman score with increasing age. There was no statistically significant difference in change in Chrispin–Norman score over time between preschool and schoolchildren (fig. 2⇓). The mean changes in radiograph scores expressed as a percentage of the maximal scores in preschool children were 2.2, 2.6, 0.4 and 1.7%·yr−1 for Chrispin–Norman, adjusted Chrispin–Norman, Wisconsin and Northern, respectively. In schoolchildren, only the Chrispin–Norman and adjusted Chrispin–Norman scores worsened significantly over time (table 2⇓). The mean changes in radiograph scores expressed as a percentage of the maximal scores in schoolchildren were 1.3, 1.5, 0.0 and 0.5%·yr−1 for Chrispin–Norman, adjusted Chrispin–Norman, Wisconsin and Northern, respectively. Preschool children showed a tendency towards more pronounced changes in chest radiograph scores over time, but this was only statistically significant for the Wisconsin score (p = 0.04). Individual progression of lung disease over time scored according to the Chrispin–Norman score is illustrated in figure 3⇓.

Chrispin–Norman score plotted against age for the whole group at visit 1. Slopes are shown for the group as a whole (—) and for both preschool (·····) and schoolchildren (----). The regression equation for the group as a whole was y = 0.445x+7.02.

Individual changes in Chrispin–Norman score versus age at both visits. The regression equation was Chrispin–Norman score at visit 2 = 0.51×(Chrispin–Norman score at visit 1)+6.36.
Mean annual change for different parameters in preschool# and schoolchildren¶
Lung function over time
Rint,exp Z-scores did not change significantly over time in preschool and schoolchildren. Changes in Rint,exp Z-scores were also assessed in CF patients with no, or only mild signs of, pulmonary hyperinflation on their chest radiograph. Only 15 children showed no or only mild hyperinflation. The difference in progression of Rint,exp Z-score between children with no or only mild hyperinflation versus moderate-to-severe hyperinflation was 0.02±0.92 versus 0.37±1.6 (p = 0.51). When comparing preschool children with schoolchildren, Rint,exp Z-scores appeared higher in schoolchildren but this difference was not statistically significant.
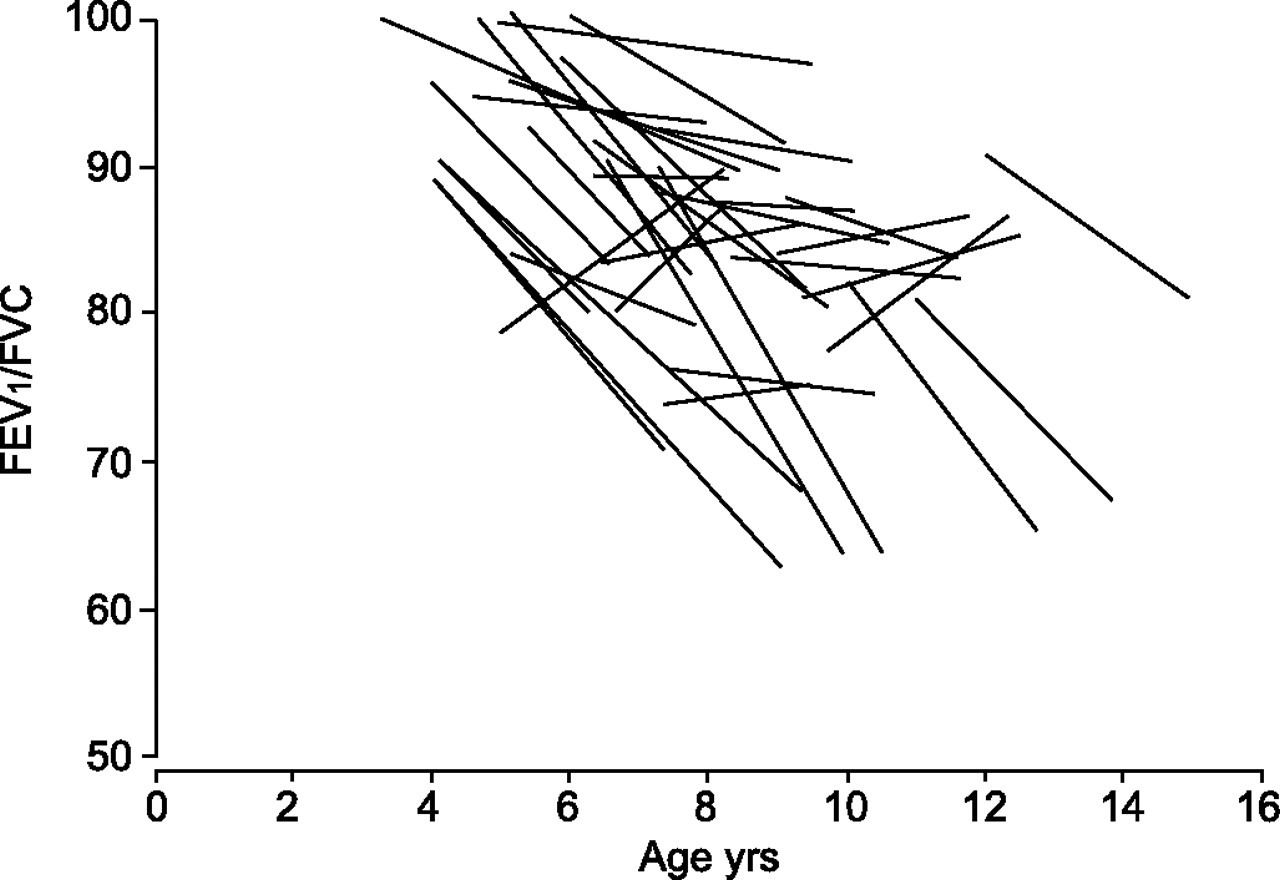
In schoolchildren, only FEV1/FVC worsened significantly over time (annual decline 1.94%; p<0.01). Individual changes in FEV1/FVC were plotted versus age over time for all schoolchildren and eight preschool children that were able to perform spirometry at both visits, as shown in figure 4⇓.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual changes in forced expiratory volume in one second as a percentage of forced vital capacity (FEV1/FVC) over time for 30 schoolchildren and eight preschool children. The mean/average regression equation was FEV1/FVC at visit 2 = 0.553×(FEV1/FVC at visit 1)+33.38.
Correlation between lung structure and lung function
In preschool children, there was no significant correlation between chest radiograph and Rint,exp Z-score at visits 1 and 2 at cross-sectional data analysis. Longitudinal data analysis also showed no significant correlation between Δchest radiograph scores and ΔRint,exp Z-score. In schoolchildren, no significant correlation was found between chest radiograph and Rint,exp Z-score at visits 1 and 2, or between chest radiograph and PFT at visit 1. There was, however, a significant but moderate correlation between the Chrispin–Norman and adjusted Chrispin–Norman scores and FEV1, MEF50%, FEF25–75% and FEV1/FVC at visit 2. The Wisconsin score correlated significantly but weakly with FEV1, FEV1/FVC and FEF25-75% and the Brasfield score correlated significantly but weakly with FEV1 and MEF25-75% at visit 2.
DISCUSSION
In the present study the capability of chest radiograph scores, Rint,exp measurements and spirometry to detect and monitor progression of lung damage in young children with CF was evaluated. Chest radiograph scores worsened significantly over a 3-yr period in both preschool and schoolchildren. In the study group, the annual changes for the Wisconsin score were less than those observed in the large Wisconsin trial cohort previously described elsewhere 8. Comparisons are hampered by the fact that the Wisconsin trial group was subdivided into four groups: screened, nonscreened and patients with or without Pseudomonas aeruginosa. Besides differences between the Wisconsin trial and the present study in the number of children included and the duration of follow-up, the time of inclusion was also different. In the Wisconsin trial, children from the period 1985–1998 were included. In recent years, major changes in the detection techniques and treatment regimen for P. aeruginosa have been implemented in daily CF care, making comparison of the present cohort with the Wisconsin trial cohort more difficult. In the present cohort, five preschool children and six schoolchildren had a positive sputum culture with P. aeruginosa at visit 1. These children did not show faster progression than the children without P. aeruginosa. In the Wisconsin trial, however, children who acquired P. aeruginosa at a young age showed marked progression of the Wisconsin chest radiograph scores after the age of 10 yrs. Follow-up in the present cohort is too short to come to the same conclusion.
Preschool children showed a tendency towards a faster decline in chest radiograph scores than schoolchildren and this difference was statistically significant for the Wisconsin score. The Chrispin–Norman and adjusted Chrispin–Norman scores showed the greatest annual decline in both preschool and schoolchildren. Conversely, Wisconsin, Northern and Brasfield scores did not change significantly in schoolchildren. At inclusion, 24–33% of preschool children and 40–50% of schoolchildren already had a chest radiograph score that resembled mild but potentially irreversible lung damage 10. In the present study, radiograph scores were more sensitive to monitor disease progression than functional parameters, especially in young children. This suggests that chest radiographs can be helpful in the follow-up of CF lung disease progression in young children. Chest radiographs can sensitively measure changes from normality to mild lung disease and these changes already appear in preschool children. The schoolchildren scored in the present study had normal lung function both at visits 1 and 2. In schoolchildren, bronchiectasis became an important morphological change and HRCT of the chest is considered the gold standard for diagnosing bronchiectasis 23. This might, in part, explain why in the present study chest radiograph scores in schoolchildren showed less progression over the 3-yr period than the scores in preschool children.
One of the drawbacks of using CF chest radiograph scores is that the interpretation of the abnormalities seen on a chest radiograph is not always straightforward. For example, increased densities can be interpreted in various ways and this can cause greater interobserver variability of scores. Intra- and interobserver variability of the chest radiograph scores used in the present study was moderate to good. The use of HRCT of the chest has been advocated for several years, since HRCT seems to be more sensitive than chest radiographs in detecting structural abnormalities in children with mild CF 24–26. Even in young children and infants with CF, HRCT can detect structural abnormalities 27, 28. Several cross-sectional studies showed good correlation between HRCT scores and chest radiograph scores 24, 25, 29. Although HRCT is sensitive in detecting structural abnormalities 27, especially in young patients, implementation of sequential HRCT scanning into daily CF care is hampered by several factors. HRCT of the chest causes higher radiation dosage and a subsequent higher risk for cancer compared with chest radiographs 30. It is more expensive and, although scan time of modern scanners has become so short that images can be obtained while the child is spontaneously breathing, HRCT in very young children still requires sedation. Studies comparing changes in HRCT scores with changes in chest radiograph scores in children over a longer period of time are lacking. In the present study it is shown that chest radiograph scores worsen in both preschool and schoolchildren while lung function remains stable. Considering these results and the current limitations in the implementation of HRCT scanning in daily CF care, there still seems to be a valuable role for chest radiograph scores in monitoring structural lung damage in daily clinical practice and possibly in long-term clinical trials, especially since the radiation burden is reduced even further by excluding the lateral film 31. Radiation burden and the increased risk of cancer related to repeated HRCT scans compared with chest radiographs should remain a topic of discussion, since survival in CF has increased significantly over time.
Despite significant abnormalities of chest radiograph scores, most preschool and schoolchildren had a Rint,exp Z-score within the normal range both at visits 1 and 2, and the annual change in Rint,exp Z-score was not significant. These findings suggest that Rint,exp measurements do not sensitively discriminate between children with CF and healthy children, and that longitudinal evaluation of Rint,exp measurements are not sensitive enough to detect early progression of lung disease in CF. The between-occasion repeatability of Rint is poor and the variation in bronchial tone is high, limiting the usefulness of repeated Rint,exp measurements in monitoring disease progression in CF 32. Furthermore, most patients in the present study had signs of hyperinflation, as was established according to their chest radiograph. CF patients with pulmonary hyperinflation can compensate by elevating their resting end-expiratory level, a pathophysiological feature that is not recognised by Rint measurements. In accordance with the present results, no consistent abnormal levels or increases in Rint were found in a 4-yr prospective study of inspiratory respiratory resistance measured according to the interrupter technique in young children with CF 20.
No correlation was found between structural damage assessed by chest radiograph scores and lung function at visit 1. This is not surprising at all since correlations between functional features and structural alterations of a common origin would not be expected. It would be interesting to compare, for example, pulmonary hyperinflation with functional residual capacity, or nodular cystic lesions with gas exchange. These comparisons are complicated by the fact that most of the children included in the present study were too young to perform PFTs other than Rint measurements and spirometry. Progression of Rint,exp Z-score was compared between children with no or mild signs of hyperinflation on their chest radiograph and children with moderate-to-severe hyperinflation, but no statistically significant difference was found. In schoolchildren no correlation was found between chest radiograph scores and spirometry at visit 1; however, a moderate but significant correlation was observed between most chest radiograph scores and spirometry at visit 2. One possible explanation for the moderate but significant correlation between chest radiograph scores and spirometry at visit 2 is that at visit 2 a larger proportion of children had a FEV1 <85% pred, suggesting more advanced lung disease and, consequently, a better correlation with structural abnormalities, as has been shown previously 7. Other possibilities include a higher inflation level when the chest radiograph was taken and improved technical abilities due to their older age.
Longitudinal analysis of PFT decline in schoolchildren showed no statistically significant worsening except for FEV1/FVC. A significant change in FEV1/FVC ratio (expressed as Z-score) has been described previously by de Jong et al. 33 in a larger group of older children with CF. In a different study by de Jong et al. 27 no significant annual decline in % pred values of FEV1/FVC ratio was described. Significant but slow deterioration of FEV1/FVC % pred ratio was, however, described in a longitudinal study assessing effect of mucoid P. aeruginosa infection on lung disease progression 9. Whether the FEV1/FVC ratio is a sensitive measure in detecting early and mild lung disease in CF remains to be answered, since neither % pred nor FEV1/FVC ratio Z-score is usually considered a primary end-point in CF trials. Depending on the stage of lung disease, different spirometric parameters have different sensitivities in detecting changes 34. FEV1/FVC might thus be a more sensitive spirometric parameter in early CF lung disease than FEV1 and should be included as an end-point in clinical trials in early CF lung disease.
In conclusion, the present study shows that there is a significant annual deterioration of routine chest radiograph scores in young children, especially in preschool children. A proportion of preschool children already have abnormal chest radiographs, while expiratory interrupter resistanceZ-scores are within the normal range in most children with cystic fibrosis. Expiratory interrupter resistance is not a good measure with which to monitor pulmonary disease progression in groups of children with cystic fibrosis. Spirometry (except for forced expiratory volume in one second as a percentage of forced vital capacity) in schoolchildren remained stable in the studied group and correlated only moderately with chest radiographs. Therefore, radiograph scores represent a more sensitive measure than pulmonary function tests to evaluate lung disease progression in young children with mild cystic fibrosis lung disease.
Acknowledgments
The authors would like to thank I. Prins and J. Tersmette (Dept of Paediatric Pulmonology, University Medical Centre Utrecht, Utrecht, the Netherlands) for performing all interrupter resistance measurements.
- Received April 13, 2006.
- Accepted April 7, 2007.
- © ERS Journals Ltd
References










