





Abstract
Haemoglobin (Hb) abnormalities in chronic obstructive pulmonary disease (COPD) are not well characterised. The present authors investigated the prevalence and association of abnormal Hb with clinical outcomes.
Analysis of a prospective cohort of stable COPD outpatients (n = 683) in a USA Veterans Administration pulmonary clinic was undertaken. Patients were classified as anaemic (Hb <13 g·dL−1), polycythemic (Hb ≥17 g·dL−1 and ≥15 g·dL−1 for males and females, respectively) or normal. Demographic characteristics and physiological/functional outcomes were compared between groups. Regression models adjusting for confounders examined the independent association of anaemia with clinical outcomes.
Anaemia was present in 116 (17%) patients and polycythemia in 40 (6%). While the only values that differed between polycythemic and nonpolycythemic patients were mean body mass index and Hb, anaemic patients showed a significantly higher modified Medical Research Council dyspnoea scale score (2.8 versus 2.6), lower 6-min walk distance (265 versus 325 m) and shorter median survival (49 versus 74 months) than nonanaemic patients. In regression models, anaemia independently predicted dyspnoea and reduced exercise capacity.
Anaemia in chronic obstructive pulmonary disease was an independent risk factor for reduced functional capacity. Polycythemia prevalence was low and had no association with worsened outcomes. Further work is required to evaluate the effect of anaemia correction on outcomes in chronic obstructive pulmonary disease.
Chronic obstructive pulmonary disease (COPD) is highly prevalent and associated with substantial morbidity and mortality. In the USA, an estimated 11.4 million adults were reported to have COPD in 2004 1. The forced expiratory volume in one second (FEV1) after bronchodilators has been traditionally viewed as the most accurate predictor of death in these patients 2. However, COPD produces systemic manifestations not reflected by the FEV1 and, indeed, a number of other factors predictive of COPD-related mortality have been identified. These include malnutrition, poor exercise capacity, increased dyspnoea and presence of comorbidity 3–7. Recent studies indicate that a composite index consisting of markers of COPD severity (body mass index (BMI), airflow obstruction, dyspnoea and exercise capacity (BODE) index) is a more accurate predictor than FEV1 alone of all-cause and respiratory mortality 8.
Anaemia, a well-recognised comorbidity in many chronic illnesses, is associated with reduced health-related quality of life (HRQL), increased morbidity and mortality in chronic kidney disease 9, 10, congestive heart failure 11–13, HIV infection 14, 15, hepatitis-C virus infection 16 and cancer 17. Anaemia is also associated with disability, impaired physical performance and lower muscle strength in individuals of ≥65 yrs of age 18.
There is limited information in the current literature describing the distribution of haemoglobin (Hb) and its impact on outcomes in the COPD population. Polycythemia, traditionally thought to be highly prevalent in COPD, occurs less frequently nowadays with more rigorous correction of hypoxaemia 19. Conversely, recent reports suggest that anaemia in patients with COPD is highly prevalent and associated with increased mortality 20, 21. Although the association between anaemia and dyspnoea is generally well established 22, the contribution of Hb to breathlessness and other clinical manifestations in patients with COPD is unknown, and may be of great interest as a potential target for directed therapy 23. The purpose of the present study was to determine the prevalence of abnormalities in Hb levels in patients with COPD attending a pulmonary clinic, as well as to explore the associations between Hb levels and clinical outcomes.
MATERIALS AND METHODS
Study subjects
The present study was a retrospective analysis of data prospectively collected at one of the sites (Bay Pines Veterans Affairs Medical Centre, Bay Pines, FL, USA) of the multicentre BODE study cohort 8. COPD was defined by a history of smoking >20 pack-yrs and a ratio of FEV1 to forced vital capacity <0.7 measured 20 min after administration of albuterol. Outpatients with a wide range of COPD severity were included. All patients were clinically stable and receiving appropriate therapy for COPD. Exclusion criteria were: 1) an illness other than COPD likely to result in death within 3 yrs; 2) asthma (defined as an increase in FEV1 >15% above the baseline value or of 200 mL after administration of a bronchodilator); 3) inability to complete the lung function test or 6-min walking distance (6MWD) test; and 4) myocardial infarction within the preceding 4 months, unstable angina or congestive heart failure (New York Heart Association class III or IV). Full methodology and results from the prospective study have been previously reported elsewhere 8.
Study design
Hb data were collected retrospectively, while all other data had been included in the prospective data collection. For each patient, the Hb value closest in time, prior to or following, BODE testing was collected and analysed. Patients were categorised into three groups according to Hb thresholds: 1) anaemic, with Hb levels <13 g·dL−1 for males and females 24; 2) polycythemic with Hb levels ≥17 g·dL−1 and ≥15 g·dL−1 for males and females, respectively 25; and 3) normal. Although the Hb threshold for anaemia in females is defined by the World Health Organization as <12 g·dL−1, a threshold of <13 g·dL−1 was chosen for all patients in the present study, since the issue of appropriate Hb threshold for anaemia definition in post-menopausal females remains controversial 26. In addition, the vast majority (96%) of patients in the dataset were males. Since the number of polycythemic patients was small and their baseline characteristics and outcomes were not significantly different from the nonpolycythemic group, only the descriptive data on the polycythemia subset are presented. For the analytical portion of the present study, polycythemic patients were included in the group with normal Hb levels.
Clinical variables evaluated for each group consisted of dyspnoea, exercise capacity, mortality and healthcare resource utilisation. Functional dyspnoea was measured using the Medical Research Council (MRC) dyspnoea scale, a validated instrument that quantitatively assesses the severity of COPD-related disability 27. Scores on the MRC dyspnoea scale range 0−4, with a score of four indicating that the patient is too breathless to leave the house or becomes breathless when dressing or undressing. Exercise capacity was measured according to the 6MWD test, a standardised, validated test that is a predictor of functional status and death 28. Mortality and cause of death were determined through family contact followed by review of medical records and death certificates.
Scores on the Charlson comorbidity index (CCI) and the BODE index were also evaluated for each group of patients. The CCI is a validated method for classifying comorbid conditions that can alter the risk of mortality 29 and has been shown to predict mortality 30. Scores on the CCI range 0−33, with higher scores indicating more coexisting conditions.
Statistical analyses
Between-group differences in baseline demographic, physiological and disease characteristics were expressed as mean±sd values. The between-group differences were calculated using a two-sided paired t-test or Chi-squared statistic where appropriate. A p-value <0.05 was considered statistically significant. Linear regression analyses controlling for age, FEV1, CCI and BMI were performed to identify the independent association of anaemia with the MRC dyspnoea scale and the 6MWD test. Median survival and the overall probability of survival between anaemic and nonanaemic patients were calculated using Kaplan–Meier estimates. A logistic regression analysis and a Cox proportional hazards model were run to adjust the estimate of Hb association with mortality for age, CCI and BODE index.
RESULTS
Patient characteristics
Of the 683 patients in the dataset (656 males, 27 females; mean±sd age 67±9 yrs), 677 were eligible for analysis (650 males, 27 females; 70±9 yrs). The remaining 6 male patients (74±5 yrs) were excluded due to missing Hb values. The mean±sd Hb for all patients was 14.4±1.7 g·dL−1. Anaemia was present in 116 (17.1%) patients, while polycythemia was recorded in 40 (5.9%) patients. Applying the Hb threshold of 13 g·dL−1, as opposed to 12 g·dL−1, for anaemia definition among females in the present study resulted in potential misclassification of three subjects, whose Hb values were ≥12–<13 g·dL−1. Mean Hb levels for anaemic and nonanaemic patients were 11.8±1.0 g·dL−1 and 15.0±1.2 g·dL−1, respectively (p<0.0001). There was no difference in the mean Hb between patients receiving supplemental oxygen and those who did not receive it (14.4±1.8 g·dL−1 and 14.5±1.6 g·dL−1, respectively; p = 0.49), and there was no correlation between arterial oxygen tension and Hb (Pearson r = -0.06). Overall, anaemic patients were significantly older and more chronically ill than their nonanaemic counterparts, as manifested by significantly higher CCI and BODE index scores (table 1⇓). Conversely, except for higher mean Hb and BMI in the group with polycythemia, there were no significant differences in the baseline characteristics or outcome measures between polycythemic and nonpolycythemic groups (table 2⇓).
Patient demographics and clinical characteristics
Characteristics of patients with and without polycythemia
Dyspnoea and functional impairment
Dyspnoea and functional status differed significantly between anaemic and nonanaemic patients. Mean MRC values were significantly higher (2.8±0.9 versus 2.6±0.8; p = 0.04) and mean 6MWD was significantly shorter (265±122 m versus 325±124 m; p<0.0001) in anaemic compared with nonanaemic patients (table 1⇑). When MRC and 6MWD were evaluated as a function of Hb ranges, there was a linear relationship between declining Hb and increasing dyspnoea and functional impairment (figs 1⇓ and 2⇓). In regression models controlling for age, FEV1, CCI and BMI, anaemia remained an independent predictor of increased MRC and reduced 6MWD (table 3⇓).

Relationship between haemoglobin (Hb) level and the Medical Research Council (MRC) dyspnoea scale. ░: <12 g·dL−1 (n = 49); ▒: ≥12–<13 g·dL−1 (n = 67); □: ≥13–<14 g·dL−1 (n = 127); ▓: ≥14 g·dL−1 (n = 434).

Change in the 6-min walking distance (6MWD) test as a function of haemoglobin (Hb) level. ░: <12 g·dL−1 (n = 49); ▒: ≥12–<13 g·dL−1 (n = 67); □: ≥13–<14 g·dL−1 (n = 127); ▓: ≥14 g·dL−1 (n = 434).
Multivariate regression analysis for risk of dyspnoea and functional impairment
Mortality
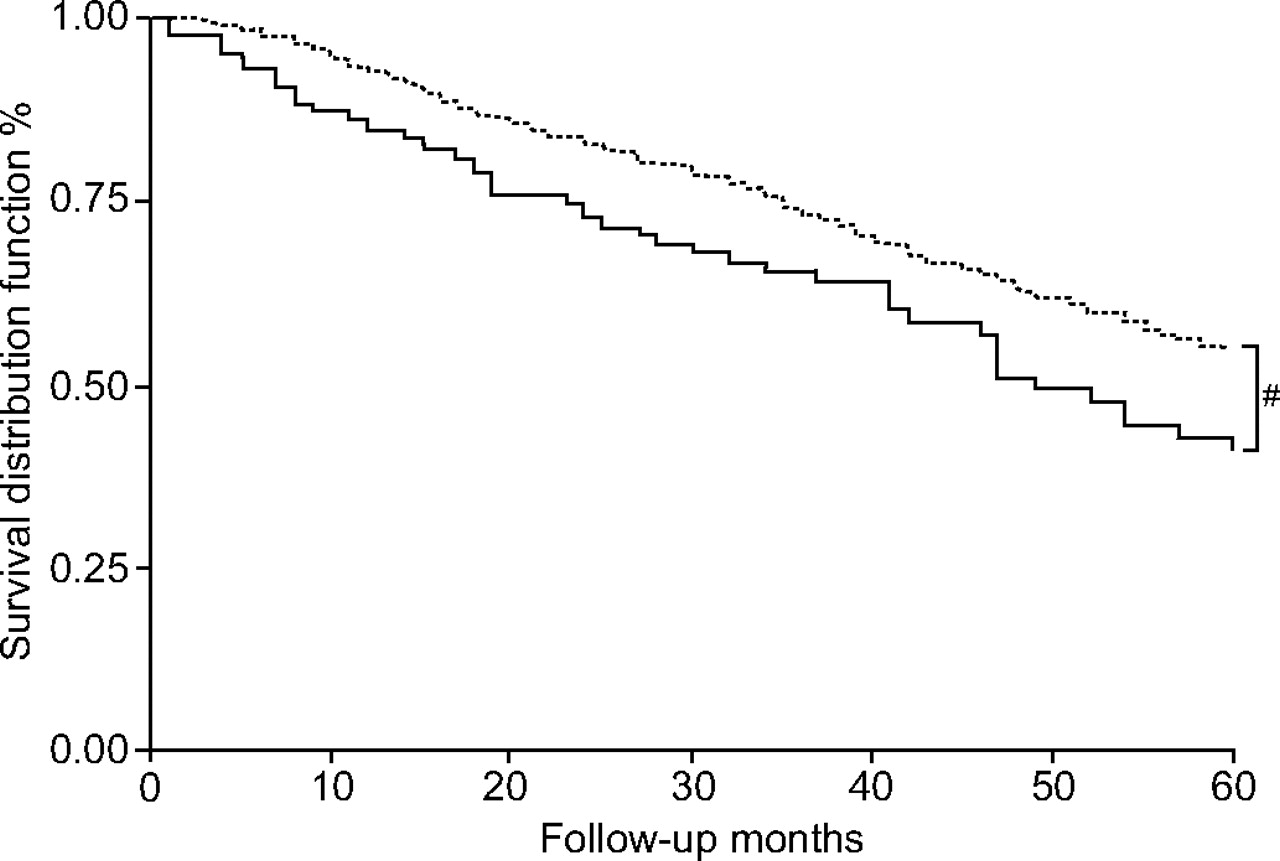
A total of 53 (46.8%) anaemic and 187 (31.2%) nonanaemic patients died (p = 0.01) during the study (mean follow-up 34±22 months and 37±22 months, respectively; p = 0.15). Age (p<0.01), Hb (p<0.01), CCI (p<0.0001) and BODE score (p<0.0001) differed significantly between survivors and nonsurvivors (table 4⇓). The median survival was 49 months in anaemic patients and 74 months in nonanaemic patients (p<0.01; fig. 3⇓). While the BODE index and the CCI were significantly associated with increased mortality in both the Cox model and the multivariate logistic regression analysis (table 5⇓), anaemia was not identified as a significant independent predictor of mortality.

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier probability of overall survival in anaemic (——) and nonanaemic patients (·······). The number of anaemic and nonanaemic patients at baseline was 116 and 561, respectively. During follow-up, the predicted number of anaemic patients was 99, 75, 53, 49, 31 and 20 at 10, 20, 30, 40, 50 and 60 months, respectively. During follow-up, the predicted number of nonanaemic patients was 528, 397, 292, 217, 150 and 101 at 10, 20, 30, 40, 50 and 60 months, respectively. #: p = 0.0091.
Significant differences in patient characteristics between survivors and nonsurvivors
Multivariate logistic regression analysis for risk of death
DISCUSSION
In the current study, anaemia was prevalent (17%) among patients with COPD attending a Veterans Affairs pulmonary clinic and was independently associated with increased dyspnoea and reduced exercise capacity as measured by the 6MWD. In contrast, there was a very low prevalence of polycythemia and, when present, it carried no clinical relevance.
Although anaemia has been associated with dyspnoea and reduced exercise capacity in patients with pre-dialysis chronic kidney disease 31, cancer 32 and heart failure 33, the present study is the first to demonstrate that anaemia is a strong independent predictor of dyspnoea and reduced exercise capacity in patients with COPD. The exact mechanism by which anaemia may decrease exercise capacity is complex and not fully understood. However, oxygen carrying capacity depends directly upon the level of haemoglobin and oxygen delivery is crucial for the maintenance of oxidative metabolism. Anaemia may result in limited oxygen supply and early onset of anaerobic threshold, with the consequent increase in ventilatory drive. Given the decreased ventilatory reserve among patients with COPD, the accompanying increased ventilatory demand may result in dyspnoea.
In the current study, polycythemia was present in 6% of the COPD patients and did not appear to be associated either with an increased COPD severity or with altered outcomes. The use of long-term oxygen therapy has been reported to control polycythemia in patients with COPD 19. Thus, the fact that more than one third of the patients received supplemental oxygen therapy may at least partially account for the low prevalence of polycythemia observed in the present study.
The prevalence of anaemia identified in the present study (17%), while somewhat higher than the 10.6% prevalence observed among community-dwelling elderly 26, is similar to that reported in recent studies of COPD patients 20, 21. In general, anaemic patients were somewhat older and carried a higher physiological dysfunction burden, as evidenced by a higher mean CCI and BODE index scores. Even after adjusting for the unequal disease burden distribution, anaemia was strongly and independently associated with worse MRC dyspnoea scores and reduced 6MWD, indicating a possible link between Hb and functional status.
Anaemia of inflammation or anaemia of chronic disease 34 are likely to play a major role in the setting of COPD, particularly since it has been identified as the cause of one third of all anaemia cases observed in the community-dwelling elderly population 26. One recent study 20 has documented that anaemia in COPD is, at least in part, due to inflammation and resistance to elevated levels of serum erythropoietin. This is not surprising, given the systemic inflammatory state that has been documented in patients with COPD 35. However, more research is needed to gain a better understanding of the potential causes of anaemia in COPD.
Aetiology notwithstanding, anaemia in COPD has been shown to be associated with adverse outcomes in recent clinical studies. In a study by Chambellan et al. 21 of 2,524 patients with severe COPD receiving long-term oxygen therapy, anaemia was associated with a lower long-term survival rate, a higher hospital admission rate and a longer duration of hospital stay compared with nonanaemic patients. The relative risk of death decreased by 14% with every 5% increase in haematocrit (p<0.001) and haematocrit was the strongest predictor of mortality next to age. In addition, haematocrit was inversely correlated with both the rate (r = -0.091; p = 0.001) and duration (r = -0.095; p<0.001) of hospitalisation. In contrast to the study by Chambellan et al. 21, the current analyses did not confirm a significant independent association between anaemia and survival. This is perhaps best explained by the fact that the study by Chambellan et al. 21 represents patients with more severe COPD compared with those in the present cohort. Additionally, comorbidity or COPD severity scores, such as the BODE index, were not included as covariates. It is likely that these tools already incorporate factors that may be associated with anaemia and thereby dilute the predictive power of anaemia per se on mortality. Future studies, however, need to continue to examine the association of anaemia with worsened outcomes, including mortality, in patients with COPD.
The relationship between anaemia and adverse clinical outcomes in patients with COPD is consistent with findings in other chronic disease states. Increased morbidity, mortality and decreased HRQL are well established in chronic kidney disease 10, 36, cancer 17, 32, 37, congestive heart failure 11, 13 and HIV infection 12, 14 with concomitant anaemia. Furthermore, numerous studies have demonstrated that correction of anaemia improves outcomes in these populations, resulting in improved functional and exercise capacity, reduced dyspnoea and improved quality of life 14, 37. In COPD, several small studies have suggested how correction of anaemia may affect outcomes in COPD. Schönhofer et al. 38 demonstrated that correction of anaemia with blood transfusions among 20 patients with severe COPD significantly reduced disease-related elevations in minute ventilation and work of breathing, suggesting that anaemia correction may be beneficial in alleviating dyspnoea and improving exercise capacity. In a separate study, Schönhofer et al. 39 demonstrated that among five patients with severe anaemia, successful treatment of anaemia resulted in an increased ability to wean patients from mechanical ventilation. While the current study did not attempt to answer the question of how anaemia correction affects outcomes, the results support the hypothesis that anaemia is associated with adverse consequences in patients with COPD. Although anaemia, a possible systemic manifestation of COPD, may be an epiphenomenon identifying sicker patients, it is reasonable to hypothesise, based on others' and the present authors’ findings, that correction of anaemia may result in improved outcomes. This hypothesis requires rigorous testing in a well-designed clinical trial.
The current study is limited by its retrospective design and is, therefore, subject to the general biases inherent in such designs. For example, the Hb data, which were incomplete or unavailable in the prospectively collected dataset, had to be retrospectively collected for the present analysis. As a result, the temporal relationship between Hb values and other variables is not consistent. The present authors attempted to minimise the effect of a random Hb selection on the outcomes of interest by choosing the Hb value temporally closest to the BODE index evaluation. This, however, does not eliminate the cross-sectional nature of the relationship of Hb and MRC and 6MWD outcomes, although the temporal relationship of Hb measurement and mortality end-point is preserved. Another potential limitation of the present study is that most patients were male; thus, the results may not be generalisable to females. However, other studies 40 have demonstrated adverse effects of anaemia among elderly females, although not specifically in the setting of COPD. Likewise, because elderly veteran patients have been shown to have a poorer health status and higher disease burden than nonveterans 41, these data may not be generalisable to patients with COPD seen outside of a Veterans Affairs pulmonary clinic. Nevertheless, the current study serves as a basis for evaluating the relationship between anaemia and clinical and functional outcomes in patients with COPD.
Although no inference of causality is possible, the present results suggest that anaemia is prevalent and associated with poor clinical and functional outcomes in patients with chronic obstructive pulmonary disease, and provide support for the evaluation and monitoring of anaemia in these patients. Since inflammation and erythropoietin suppression are likely to be at least in part responsible for anaemia in the chronic obstructive pulmonary disease population, future study designs need to incorporate evaluation of inflammatory mediators and their relationship to anaemia in chronic obstructive pulmonary disease. Prospective studies and controlled trials are warranted to confirm the present authors’ observations and to test the hypothesis that correction of anaemia can improve these clinical outcomes of patients with chronic obstructive pulmonary disease.
Statement of interest
C. Cote and B. Celli served as paid consultants for Ortho Biotech Clinical Affairs (Bridgewater, NJ, USA). M.D. Zilberberg and S.H. Mody are full-time employees and stockholders of Ortho Biotech Clinical Affairs.
- Received October 22, 2006.
- Accepted January 8, 2007.
- © ERS Journals Ltd
References










