





Abstract
The aim of the current study was to investigate the prevalence and clinical associations of nontuberculous mycobacteria (NTM) in a well-characterised cohort of patients with adult-onset bronchiectasis.
The sputum of all patients attending a tertiary referral bronchiectasis clinic between April 2002 and August 2003 was examined for mycobacteria as part of an extensive diagnostic work-up. NTM-positive patients subsequently had further sputa examined. A modified bronchiectasis scoring system was applied to all high-resolution computed tomography (HRCT) scans from NTM-positive patients, and a matched cohort without NTM.
Out of 98 patients attending the clinic, 10 had NTM in their sputum on first culture; of those, eight provided multiple positive cultures. Three patients were treated for NTM infection. A higher proportion of NTM-positive than -negative patients were subsequently diagnosed with cystic fibrosis (two out of nine versus two out of 75). On HRCT scoring, more patients in the NTM-positive group had peripheral mucus plugging than in the NTM-negative group.
In the current prospective study of a large cohort of patients with bronchiectasis, 10% cultured positive for nontuberculous mycobacteria in a random clinic sputum sample. Few clinical parameters were helpful in discriminating between groups, except for a higher prevalence of previously undiagnosed cystic fibrosis and of peripheral mucus plugging on high-resolution computed tomography in the nontuberculous mycobacteria group.
Nontuberculous mycobacteria (NTM), also known as opportunistic, environmental or atypical mycobacteria, are ubiquitous in the environment and have been isolated from soil, tap water, dust and clinical laboratories 1. Guidance has been produced for the diagnosis and treatment of NTM infection 1, 2, which requires satisfaction of clinical, microbiological and radiological criteria. In pre-existing lung disease, especially where there may be frequent exacerbations, such as in bronchiectasis, achieving a definition of clinical and radiological criteria specific for NTM infection is difficult. In such patients, radiographical criteria favouring a diagnosis of NTM infection include pleural disease, pneumonic changes, cavitating nodules, tree-in-bud (TIB) changes away from the main sites of bronchiectasis, and mosaic perfusion 3.
While there is little published information on the prevalence and significance of NTM in bronchiectasis, there are data in cystic fibrosis (CF), where NTM have been cultured from the sputum of 4–24% of screened patients 4, 5. In a large multicentre study from the USA, culture-positive patients were older, had better lung function and were more likely to be colonised with Staphylococcus aureus, but not with Pseudomonas aeruginosa 5. These findings had not been reflected in an earlier UK study, in which NTM-positive sputum cultures were associated only with increased requirement for intravenous antibiotics 4. Further analysis of the cohort from the USA found that lung-function decline was no different in patients with multiple NTM-positive sputum cultures versus those with one or no positive cultures, but that NTM-positive patients did have more characteristic features on high-resolution computed tomography (HRCT) 6.
The current authors therefore prospectively investigated a cohort of patients with adult-onset bronchiectasis to determine the prevalence of NTM in this group. It is the current authors’ practice to screen all patients for NTM on referral to their tertiary referral bronchiectasis clinic. Clinical indices were also compared with those of bronchiectasis patients who did not grow NTM over that time, to discover whether there was any association with disease severity, antibiotic usage, radiographical changes or microbiology.
METHODS
Subjects
Consecutive patients attending the Papworth Hospital Lung Defence Clinic (Cambridge, UK) between April 2002 and August 2003 were enrolled in the current prospective study. All subjects had a clinical diagnosis of bronchiectasis, confirmed by HRCT. Patients’ full history was taken and a clinical examination performed, with selected tests to further elucidate the cause of the bronchiectasis. Investigations included: α1-antitrypsin levels; CF genetics and subsequent sweat-testing if positive; immunoglobulin levels (including specific antibody responses); microscopic examination of the nasal cilia; and fibreoptic bronchoscopy. These investigations were performed according to methodologies previously described 7.
Measurements
As part of the current authors’ routine clinical practice, sputum was collected for microscopy and bacterial culture at every clinic visit. Colonisation was defined when the same organism was cultured from sputum on at least two occasions separated by 3 months within 1 yr. At the initial visit, sputum was also sent for mycobacterial culture. This was repeated at subsequent visits in those patients who had grown NTM on first culture. As this was the current authors’ routine clinical practice, neither approval from the Research Ethics Committee nor written patient consent were sought. All patients were further characterised using spirometry, in accordance with American Thoracic Society (ATS) guidelines 8.
Sputum processing
Sputum was stained directly for acid-fast bacilli and decontaminated in sodium hydroxide (2% final concentration). It was cultured by an automated liquid method using the Mycobacteria Growth Indicator Tubes (MGIT) system (Becton Dickinson, Sparks, MD, USA) and on solid media (Lowenstein Jensen (LJ) slopes) 9. MGIT tubes were incubated for 42 days and LJ slopes for 8 weeks. Mycobacteria were identified in a central reference laboratory using standard methods 10. After one Mycobacterium sp. was identified from an individual patient, at least two repeat specimens were sent for both culture and identification.
HRCT scan protocol and scoring
Thin (1-mm) collimation computed tomography (CT) images were obtained at 10-mm intervals from lung apices to bases during suspended full inspiration in the supine position. Images were reconstructed using a high spatial frequency reconstruction algorithm and displayed on lung parenchymal window settings (level: -700 Hounsfield units (HU); width: 1200 HU).
HRCT images were scored for the severity and extent of bronchiectasis and airways disease using a modified system by Bhalla et al. 11. Given the good interobserver agreement for the CT features of bronchiectasis previously published 12–14, CTs were evaluated by a single experienced cardiothoracic radiologist.
The extent and severity of bronchiectasis and CT features of airways disease were evaluated at a lobar level, with the lingula considered as a separate lobe. The presence of bronchiectasis was defined using established criteria 15, 16. The severity of bronchial dilatation (0: normal; 1: 1–2×diameter of adjacent artery; 2: 2–3×diameter of adjacent artery; 3: >3×diameter of adjacent artery), and of bronchial wall thickening (0: normal; 1: <0.5×diameter of adjacent artery; 2: 0.5–1×diameter of adjacent artery; 3: >1×diameter of adjacent artery) was scored for each lobe using previously described criteria 14, 17. The extent of bronchiectasis 11, mucus plugging 18, sacculations/abscesses 11, mosaic perfusion 18 and collapse or consolidation were assessed on a lobar basis and the number of segments involved recorded. The extent of TIB opacity was scored according to the proportion of lung involved (0: absent; 1: <25%; 2: 25–50%; 3: >50%). The distribution of bronchiectasis and mucus plugging was described for each case as central (central 50%), peripheral (outer 50%) or mixed.
Total lung scores for each abnormality were defined as the mean score from all lobes in the cases of severity of bronchial dilatation, bronchial wall thickening and TIB opacity and by the total number of involved segments (0: none; 1: 1–5 segments; 2: 6–9 segments; 3: >9 segments) for the extent of bronchiectasis 11, mucus plugging 18, sacculations/abscesses 11 and mosaic perfusion 18. The severity of collapse or consolidation was also scored according to the total number of involved segments (0: normal; 1: 1–3 segments; 2: 4–6 segments; 3: >6 segments). A combined total lung score (0–24) for all CT features was derived by summing the scores for the individual CT features.
HRCT scans were scored as described above for all NTM-positive patients. For each patient, CT scans from two matched NTM-negative patients were also scored. Cases were matched by forced expiratory volume in one second (FEV1), and for the presence of P. aeruginosa in sputum where appropriate. A mean score was then calculated for each NTM-negative pair.
Statistical analysis
Patients were divided into two groups, defined as NTM-positive (those culturing an NTM at first visit), or NTM-negative. These groups were compared using the Chi-squared test for clinical characteristics including number colonised with P. aeruginosa, number on long-term (daily) antibiotics, number with mutations of the CF transmembrane regulator (CFTR) and CT features. Group mean spirometric values and age were normally distributed and compared using the unpaired t-test. CT scores (total and by section) were not normally distributed. Group means were compared by the Mann–Whitney U-test, and pairs (i.e. each NTM-positive case and the mean of its two matched NTM-negative controls) by the Wilcoxon signed ranks test.
RESULTS
A total of 98 patients (66 females) were investigated, with mean±sem age 59.3±1.3 yrs, FEV1 63.5±2.3% predicted, and forced vital capacity (FVC) 85.8±1.9% pred. Of these, 10 grew NTM on first sputum culture; none were smear-positive. These patients were followed up over median (range) 58 (16–88) weeks, and are summarised in table 1⇓.
Clinical characteristics of the 10 subjects sputum culture-positive for nontuberculous mycobacteria (NTM)
Patient characteristics of the NTM-positive and -negative groups are shown in table 2⇓. There was no difference between groups in terms of age, sex, spirometry, or numbers with CFTR mutations, culturing P. aeruginosa or on long-term antibiotics.
Patient characteristics for patients with and without nontuberculous mycobacteria(NTM) cultured from their sputum during the study period
Four out of the six patients heterozygous for CFTR mutations had high sweat sodium concentrations (range 60–107 mM), consistent with a diagnosis of CF. Of the remaining two, one was unable to complete the test for technical reasons and the second was unwilling to undergo the test. Cause of bronchiectasis by group is shown in figure 1⇓ and table 3. Of the patients tested for both CFTR gene mutations and, if positive, by subsequent sweat test, a higher proportion of NTM-positive than -negative patients had a diagnosis of CF (two out of nine versus two out of 75; p<0.01).

Cause of bronchiectasis in patients positive (░) and negative (□) for nontuberculous mycobacteria (NTM). ABPA: allergic bronchopulmonary aspergillosis; CF: cystic fibrosis; RA; rheumatoid associated; TB: tuberculosis; GORD: gastro-oesophageal reflux disease; IBD: inflammatory bowel disease. *: p<0.01 NTM positive versus NTM negative.
Trends in FEV1 for the period before and after first positive NTM culture for the NTM-positive group are shown in figure 2⇓. There was no significant difference in FEV1 before and after NTM was first cultured, either in the NTM-positive group as a whole, or in the three patients who were subsequently treated.
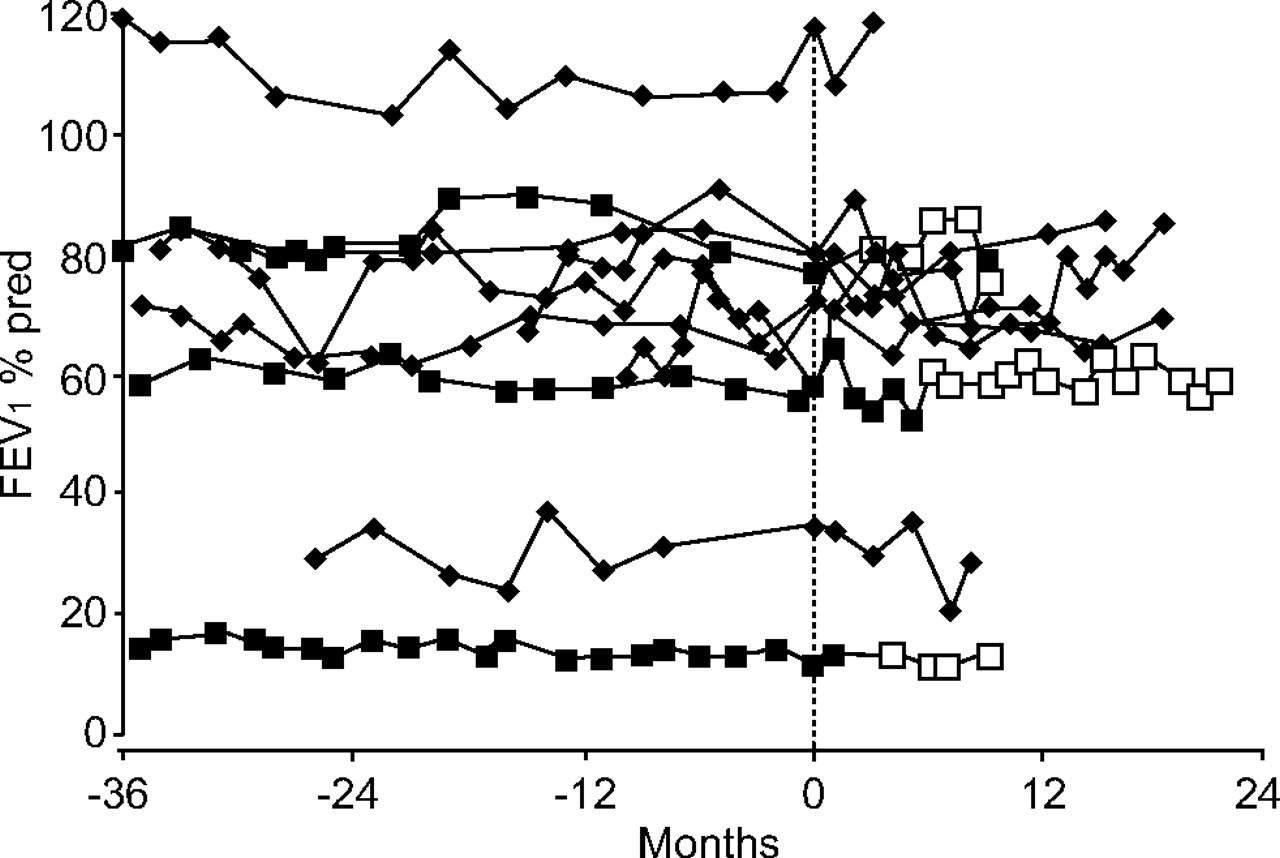
Forced expiratory volume in one second (FEV1) trends before and after first sputum culture positive for nontuberculous mycobacteria (NTM; month 0). ♦: patients not treated for NTM infection; ▪: patients yet to be treated for NTM infection; □: patients post-treatment for NTM infection. % pred: percentage of predicted value.
CT scores for the NTM-positive group versus the matched cohort are shown in table 4⇓. There were no significant differences in individual or total scores either when analysed as group means (i.e. 10 NTM-positive versus 20 NTM-negative patients) or pairwise (i.e. 10 pairs of NTM-positive versus the average of the two matched NTM-negative patients’ scores). The NTM-positive group did include more individuals with peripheral mucus plugging than the NTM-negative group (nine out of 10 versus five out of 20; p<0.001). An example of a CT image demonstrating peripheral mucous plugging is shown in figure 3⇓.

{kind=link}
{kind=link}
{kind=link}
Computed tomography image demonstrating bilateral lower-lobe bronchiectasis, with peripheral mucus plugging and “tree-in-bud” opacities seen particularly in the left lower lobe.
Cause of bronchiectasis
Mean high-resolution computed tomography (CT) scores for patients with and without nontuberculous mycobacteria (NTM) cultured from their sputum during the study period
When the data were re-analysed, excluding the two patients in the NTM-positive group who cultured NTM only on the first occasion, members of the NTM-positive group had more segments affected by mucus plugging than members of the NTM-negative group (p = 0.019 as group means; 0.026 pairwise). Otherwise, the results were unaffected (data not shown).
DISCUSSION
The current authors cultured NTM from the sputum of 10 patients with bronchiectasis, out of a screened sample of 98. NTM were subsequently re-cultured in sputum from eight of these 10 patients. The prevalence of NTM in patients in whom CF had been definitely excluded was seven (9%) out of 80. In a recent prospective cohort, Wickremasinghe et al. 19 reported multiple isolates in one out of 50 screened patients with non-CF bronchiectasis and a further single isolate in one patient. Several groups have reported the prevalence of NTM infection in patients with CF, with results ranging from 2–4% in the UK 4, 20, and 6–24% in the USA 5, 21, 22. It is also worth noting that all of the current authors’ NTM culture-positive specimens were smear-negative. This compares with ∼25% of culture-positives that were smear-positive in the CF-bronchiectasis study by Olivier et al. 5. The clinical relevance of this is not clear, but it demonstrates that the mycobacterial load in the current authors’ patients was low.
The patients in the current study were seen in a tertiary referral bronchiectasis clinic and, as such, may have features of more severe bronchiectasis than is typical for the UK, in terms of recurrent infections, immune deficiencies or symptoms, although this is not apparent from the lung-function data; patients in the current study had a mean FEV1 of 64% pred and FVC of 86% pred. There were no significant differences between NTM-positive and -negative groups in terms of age, sex, spirometry, coexistent sputum bacteriology or use of long-term antibiotics. In CF, Torrens et al. 4 noted that NTM-positive cases had received more courses of intravenous antibiotics than controls, but that there were no differences in respiratory function, or use of nebulised antibiotics. In the USA, Olivier et al. 5 found that CF patients with NTM were older, with better lung function, and were more likely than controls to culture S. aureus, but less likely to culture P. aeruginosa. In a subgroup followed over 15 months, no difference in annual rate of FEV1 decline versus NTM-negative controls was seen 6. The investigators reported increased use of intravenous antibiotics in the NTM-negative group, in contrast to Torrens et al. 4. However, an increased frequency of NTM-positive patients sputum-positive for S. aureus was again reported. It is recognised that NTM are particularly difficult to culture in sputum colonised with P. aeruginosa 23, which may explain this finding. In the present study, six out of 10 NTM-positive subjects were colonised with P. aeruginosa, so this is less likely to be a factor.
A diagnosis of CF, based on the presence of a CFTR mutation together with a positive sweat test, was more frequent in NTM-positive than in NTM-negative patients in the current study. No other specific cause of bronchiectasis was associated with NTM isolation in patients. NTM infection per se is a cause of bronchiectasis and it is possible that, in the two patients who were clinically deteriorating (patients 8 and 9), underlying NTM infection was a previously undiagnosed factor. The current authors feel that NTM infection is less likely to have been a factor in the other eight patients, as nontreatment of NTM infection causing bronchiectasis would be expected to result in further clinical deterioration, which was not evident in these cases.
Three patients were treated for NTM infection. In two cases (patients 8 and 9) there was a significant clinical deterioration that could not be explained by factors other than NTM infection. The third patient (No. 7) was under consideration for lung transplant for bronchiectasis and the transplant team had recommended an attempt be made to eradicate the NTM. ATS microbiological criteria for NTM infection 1 require that three separate sputa test positive for NTM, although the time between sample collections is not specified. Two out of the three (patients 7 and 8) therefore clearly met ATS microbiological criteria for NTM infection. It is not clear from the ATS statement, although it seems sensible, that the three NTM should be of the same species. This is relevant to the third case (patient No. 9), where Mycobacterium avium intracellulare was cultured on two occasions only, but three further sputa grew NTM that could not be further identified. As the ATS radiographical criteria for diagnosis include “multifocal bronchiectasis” as one defining characteristic, and all the patients in the current study had known bronchiectasis, this criterion becomes largely redundant in this population.
On HRCT, more NTM-positive patients than their matched controls had peripheral mucus plugging. Furthermore, when the two subjects who cultured NTM on only one occasion were excluded, the NTM-positive group scored higher than the NTM-negative group for the component of the CT scoring system that assessed the extent of mucus plugging. Otherwise, no difference was seen in the validated CT score in terms of either individual features or overall score. Even in the two patients with a clinical deterioration and multiple NTM positive cultures (patients 8 and 9), there were no unique features when compared with the other 28 CT scores. In CF NTM-positive patients, Torrens et al. 4 also found no differences in Northern chest radiograph scores. This reinforces the view that, in pre-existing structural lung disease, it is difficult to define features with sufficient specificity to aid in the diagnosis of NTM infection.
It is notable that even in patients with multiple NTM-positive sputum cultures, 58 (74%) out of 78 samples were negative. The current authors would therefore support the recommendation that a minimum of three sputum samples should be collected from a patient suspected of being infected with NTM, to minimise the risk of a false-negative result. Indeed it is likely that a proportion of the current NTM-negative group would in fact have cultured NTM subsequently had their sputum been screened for NTM throughout the study period.
There are geographical variations in both the prevalence and causative organisms of NTM infection in CF, and it is very likely that these regional and national differences apply in non-CF bronchiectasis. A recent study by Wickremasinghe et al. 19, based at the Royal Brompton Hospital (London, UK), reported that one patient out of 50 screened met ATS microbiological criteria for NTM infection, and one more tested positive on a single isolate. While the former prevalence (2%) is similar to the present study (3%; patients 2, 7 and 8), many more patients in the current study cultured NTM on more than one occasion, but for various reasons did not fulfil the criteria for infection (patients 4, 5, 6, 9 and 10). This latter difference is difficult to explain, although it may be due partly to geographical variability. It would be very interesting to know the prevalence of NTM in patients with bronchiectasis in other parts of the UK and internationally. Furthermore, NTM can be difficult to culture, especially in the presence of other colonising organisms, so regional differences in technique could account for a degree of variability.
In conclusion, the current authors have reported a 10% prevalence of nontuberculous mycobacteria (3% meeting American Thoracic Society microbiological criteria for infection) in the sputum of screened patients with bronchiectasis in a specialist clinic. No clinical features were identified that were specifically associated with nontuberculous mycobacteria isolation, except for the diagnosis of cystic fibrosis, which warrants further investigation. Previously reported radiographic hallmarks of nontuberculous mycobacterial infection in bronchiectasis 3 did not appear to identify infected individuals in the current population, although the presence of peripheral mucus plugging had 90% sensitivity and 75% specificity for the isolation of nontuberculous mycobacteria. Large prospective studies are required to provide further information to assist diagnosis and management in this difficult area. It would also be interesting to know whether the marked geographical difference in nontuberculous mycobacterial prevalence seen in cystic fibrosis is also evident in non-cystic fibrosis bronchiectasis. In both cases, standardisation of microbiological assays is essential.
Acknowledgments
The authors would like to thank F. Cafferty for statistical advice.
- Received December 20, 2005.
- Accepted June 12, 2006.
- © ERS Journals Ltd
References










