





Abstract
The inspiratory-to-total lung capacity ratio or “inspiratory fraction” (inspiratory capacity(IC)/total lung capacity (TLC)) may be functionally more representative than traditional indices of resting airflow limitation and lung hyperinflation in patients with chronic obstructive pulmonary disease (COPD).
In the present retrospective study, a comparison was made of the individual performance of post-bronchodilator IC, IC/TLC and forced expiratory volume in one second (FEV1) in predicting a severely reduced peak oxygen uptake (V′O2; <60% predicted) in 44 COPD patients Global Initiative for Chronic Obstructive Lung Disease stages II-III (post-bronchodilator FEV1 ranging from 31–79% pred).
Patients with lower IC/TLC values (≤0.28) showed increased lung volumes and reduced exercise capacity as compared with other subjects. Following a multiple linear regression analysis, only IC/TLC and FEV1 remained as independent predictors of V′O2 (r2 = 0.33). A receiver operating characteristic (ROC) curve analysis revealed that an IC/TLC ≤0.28 had the highest specificity (89.6%), positive predictive value (80%) and overall accuracy (86.3%) in identifying patients with V′O2 <60% pred. In addition, the area under the ROC curve tended to be higher for IC/TLC than IC.
In conclusion, post-bronchodilator total lung capacity-corrected inspiratory fraction provides useful information in addition to forced expiratory volume in one second and inspiratory capacity, to estimate the likelihood of chronic obstructive pulmonary disease patients to present with severely reduced maximal exercise capacity.
- Chronic obstructive pulmonary disease
- dyspnoea
- exercise
- inspiratory fraction
- lung hyperinflation
- lung volumes
Exercise intolerance is the hallmark of chronic obstructive pulmonary disease (COPD), being ascribed to complex interactions between ventilatory, cardiovascular and peripheral muscle abnormalities 1. Amongst the pulmonary-ventilatory mechanisms that could contribute to exercise impairment in these patients, dynamic hyperinflation (DH) seems to be of special relevance 1, 2. In this context, inspiratory capacity (IC) at rest and during exercise have been shown to be superior to traditional measures of airflow obstruction (such as forced expiratory volume in one second (FEV1)) in predicting exercise impairment and improvement in tolerance to effort after bronchodilators, especially in patients with more advanced disease 3–5. However, IC measurements in isolation may provide insufficient information about the actual elastic load during exercise and, therefore, patients' ability to sustain exercise. Casanova et al. 6 have argued that IC correction for the total lung capacity (TLC) would provide a better characterisation of the volume fraction available for inspiration than IC alone. In fact, this so-called “inspiratory fraction” (IC/TLC) has been found to constitute an important prognostic factor in moderate-to-severe COPD. Another prospective study 7 showed that air trapping, expressed as increased residual volume (RV)/TLC ratio, was a powerful predictor of mortality in patients with COPD. To the current authors’ knowledge, however, no previous study has systematically evaluated the value of resting IC/TLC in predicting maximal exercise tolerance in this patient population.
Therefore, the primary objective of this study was to investigate whether the inspiratory fraction would be useful in predicting maximal exercise capacity in COPD patients presenting with increased static lung volumes at rest.
METHODS
Subjects
The study population comprised 44 patients (33 males and 11 females) who had participated in an unpublished investigation on the effects of neuromuscular electrical stimulation on peripheral muscle function and structure. All subjects had a clinical and functional diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria (stage II = 24 and stage III = 20) 8, presenting with FEV1/forced vital capacity (FVC) ratio <0.7 and FEV1 <80 but >30% predicted. In addition, all patients were required to present with increased static lung volumes at rest. Patients were clinically stable for ≥4 weeks and were optimised in terms of medical therapy, including short- and long-acting β2-adrenergics, short- and long-acting anticholinergics and inhaled steroids. Exclusion criteria were as follows: suspected asthma; other systemic conditions that could contribute to dyspnoea or exercise limitation, such as heart failure or metabolic disorders; and resting arterial oxygen saturation measured by pulse oximetry (Sp,O2; <90%). Patients gave informed consent and the study protocol was approved by a Medical Ethics Committee.
Measurements
Anthropometry
Height was obtained to the nearest 0.5 cm with subjects standing barefoot; body mass was measured with subjects in light clothing and was established to the nearest 0.1 kg. Body mass index (BMI; kg·m-2) was then calculated.
Pulmonary function
Spirometric tests were performed by using the CPF SystemTM (Medical Graphics Corp., St Paul, MN, USA), with airflow measured by a calibrated Pitot tube (PreVent PneumotachTM; Medical Graphics Corp.). The subjects completed at least three acceptable maximal forced and slow expiratory manoeuvres: in order to assess exercise capacity under improved ventilatory conditions, the patients were tested 20 min after the inhalation of 400 μg of salbutamol via a metered-dose inhaler. FVC, FEV1 and IC were recorded in body temperature and pressure, saturated conditions. Predicted values were those for the adult Brazilian population 9.
The diffusing capacity of the lung for carbon monoxide (DL,CO) was measured by the modified Krogh technique (single breath); subjects performed two acceptable and reproducible tests, with the results being within 10% or 3 mL·CO·min-1·mmHg-110. TLC (L) and RV (L) were obtained by constant-volume, different-pressure body plethysmography and expressed as a percentage of the predicted value according to Brazilian standards 11. Air trapping was defined as increased RV/TLC and RV (>0.4 and >140% pred, respectively), TLC values >120% pred were assumed to be indicative of lung hyperinflation 12. Arterial partial pressure for oxygen (Pa,O2) and carbon dioxide (Pa,CO2) were measured (mmHg) in anaerobic conditions.
Cardiopulmonary exercise test
Symptom-limited, ramp-incremental cycle ergometer exercise tests were performed on a digital computer-based exercise system (CardiO2 System; Medical Graphics Corp.) with breath-by-breath analysis of metabolic, ventilatory and cardiovascular variables. The rate of power increment was individually selected (usually 5–10 W·min-1) to provide an exercise duration of >8 but <12 min. The following data were recorded as mean of 15 s: pulmonary oxygen uptake (V′O2; mL·min-1); minute ventilation (V′E; L·min-1); respiratory rate (RR) and tidal volume (VT; L). Peak V′O2 was the highest value found at exercise cessation; predicted values were in line with those of Neder et al. 13 for the adult Brazilian population. In the present study, a peak V′O2 <60% predicted was considered indicative of a severely-reduced maximum aerobic capacity 13. Cardiac frequency (ƒC, bpm) was determined using the R-R interval from a 12-lead online electrocardiogram. Subjects were also asked to rate their “shortness of breath” at peak exercise using the 0–10 Borg's category-ratio scale 14. Dyspnoea ratings were also corrected for the ongoing level of total ventilatory stress (dyspnoea/V′E; Borg units·L-1·min-1).
Statistical analysis
Data are presented as mean and sd for normally distributed variables (Kolmogorov–Smirnov), and median (range) otherwise. Pearson's correlation coefficient was used to assess the level of association between continuous variables. Backward stepwise multiple linear regression was performed to define the independent predictors of peak V′O2 (% pred); resting variables that were significantly related to peak V′O2 at the 10% level (p<0.10) were considered for inclusion in the model. In the regression analysis, however, only variables independently related to peak V′O2at the 5% level (p<0.05) were allowed to remain in the final model. One-way ANOVA with post-hoc Scheffe test was used to compare variables between the IC/TLC groups. Receiver operating characteristic (ROC) curves were obtained for selected resting physiological variables, in order to predict a severely reduced maximal exercise capacity (peak V′O2 <60% pred). The areas under the ROC curves were then compared according to Delong et al. 15 for pairwise differences. Sensitivity, specificity, positive and negative predictive values, positive and negative likelihood ratios, and accuracy were calculated for the cut-offs derived from the ROC curves. The level of statistical significance was set at 5% for all hypothesis tests (p<0.05).
RESULTS
Population characteristics
Resting and exercise characteristics are presented in table 1⇓. On average, patients had moderate-to-severe airflow obstruction with evidence of air trapping (n = 44) and lung hyperinflation (n = 18). Maximal exercise capacity (peak V′O2) was below the lower limit of normal in 38 patients (86.3%) 12 and 16 subjects (36.3%) had a severe reduction in peak V′O2 (<60% pred). Pulmonary-ventilatory limitation, as indicated by increased V′Emax/maximal voluntary ventilation ratio (>0.8), was found in all subjects; accordingly, dyspnoea was the main exercise limiting symptom (table 1⇓).
Patient characteristics at rest and maximal exercise
Relationship between resting parameters and maximal exercise capacity
Maximal exercise capacity (peak V′O2, % pred) was significantly related to a number of resting variables, including: IC/TLC (r = 0.45, fig. 1⇓), IC (r = 0.26), TLC (r = 0.38), RV (r = 0.48), and FEV1 (r = 0.58). After multiple regression analysis, which considered all of these variables, only IC/TLC and FEV1 remained as independent predictors in the final model: peak V′O2 (% pred) = 78.9 IC/TLC+26.1 FEV1 (% pred)+29.4 (p<0.01; r2 = 0.334).
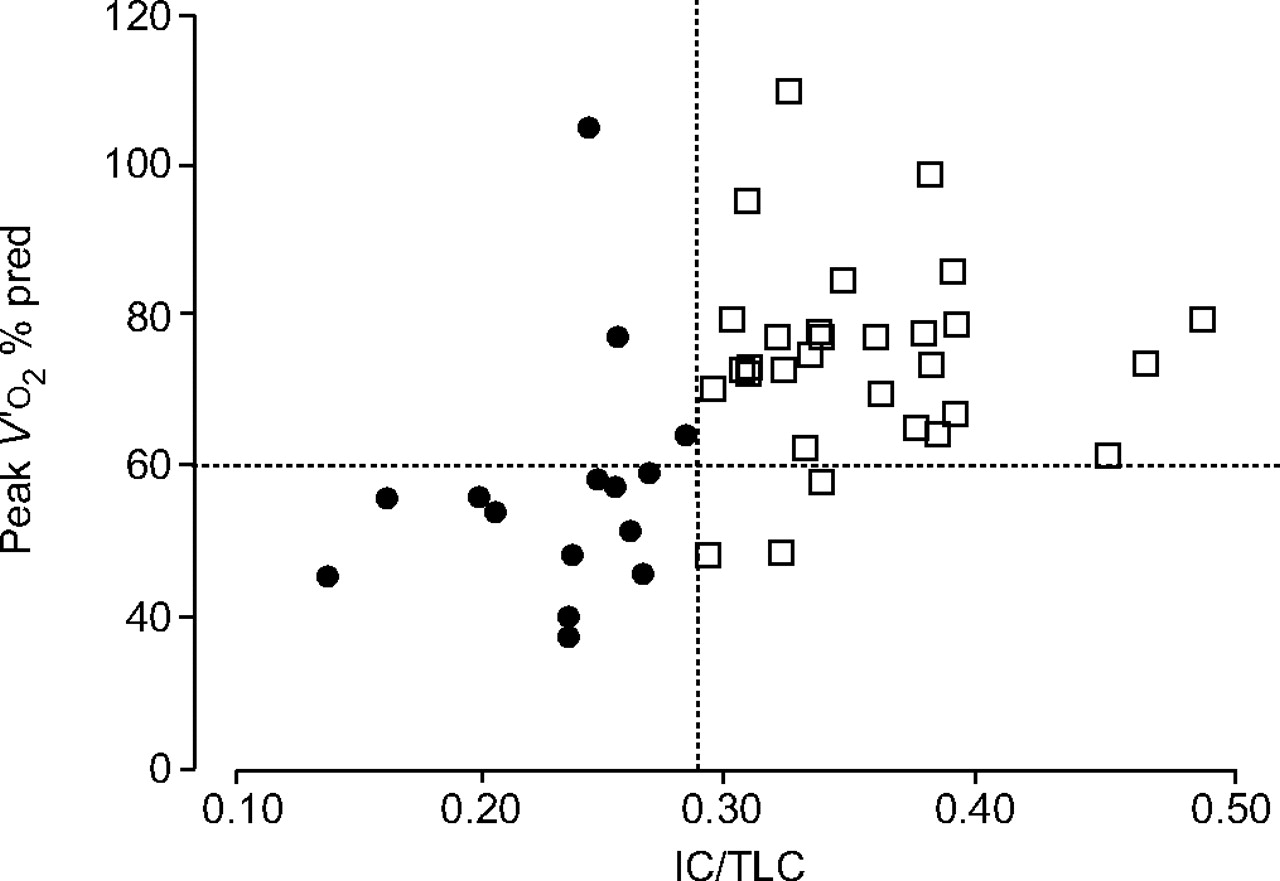
Relationship between inspiratory capacity (IC)/total lung capacity (TLC) ratio and maximal exercise capacity (peak oxygen uptake, V'O2) in a group of 44 patients with chronic obstructive pulmonary disease. % pred: percentage of predicted. •: group 1 IC/TLC <0.28; □: group 2 IC/TLC >0.28.
Lung function predictors of a severely reduced maximal exercise capacity
As IC/TLC was an independent predictor of peak V′O2, this relationship was examined more carefully. As shown in figure 1⇑, all but three patients with an IC/TLC ≤0.28 (group I) had peak V′O2 values <60% pred. However, only three patients with an IC/TLC >0.28 (group II) had peak V’O2values <60% pred. In fact, there were several between–group differences either at rest or during exercise (table 2⇓). Group 1 patients had reduced BMI, worse lung function (airflow obstruction, air trapping and lung hyperinflation) and, as expected, lowest exercise capacity (p<0.05). Importantly, these patients tended to present with reduced VT and increased ventilation-corrected dyspnoea scores (table 2⇓).
Resting and exercise parameters of patients according to inspiratory fraction(inspiratory capacity (IC)/ total lung capacity (TLC))
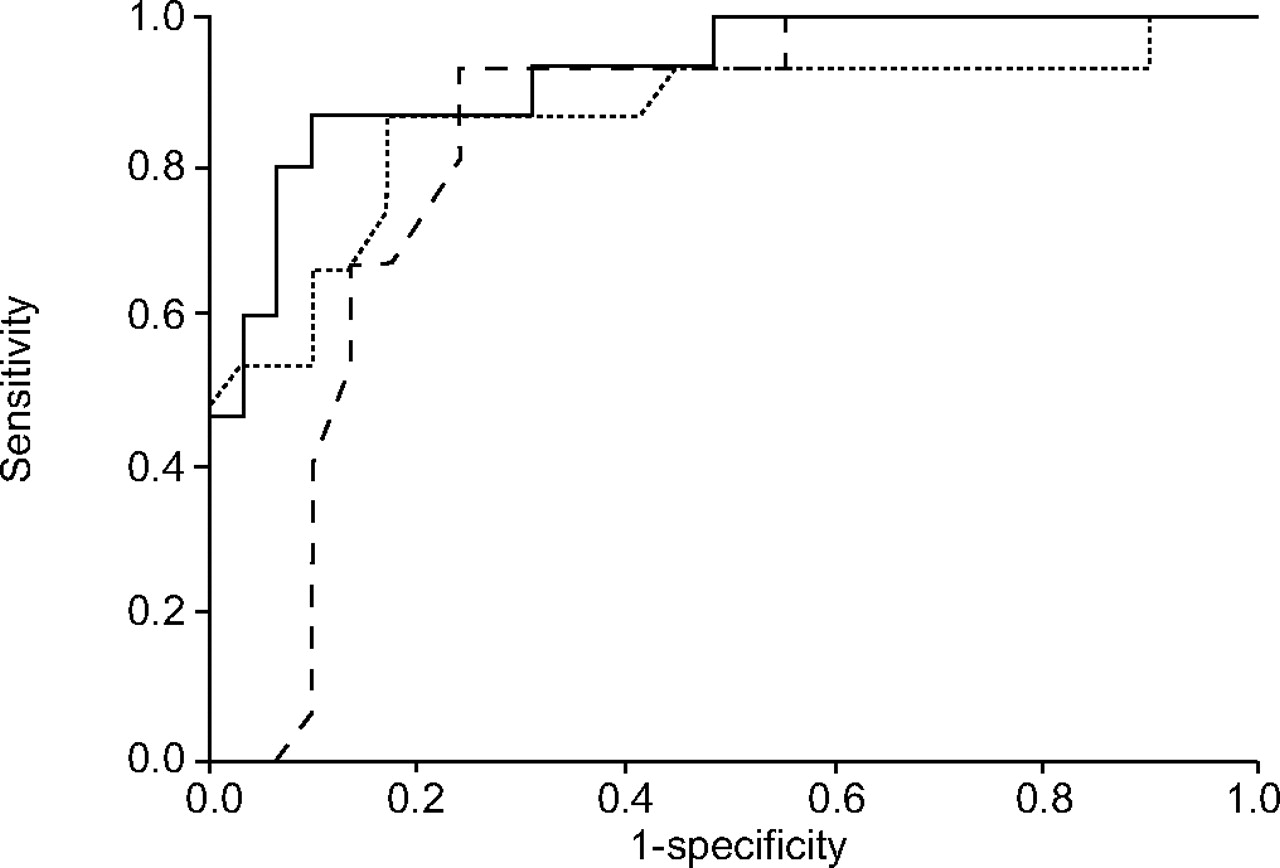
In order to compare the resting physiological variables in their ability to predict a severely reduced peak V′O2, the area under the ROC curves (AUC) for IC/TLC, IC (% pred) and FEV1 (% pred), were compared. As shown in figure 2⇓, IC/TLC had the highest AUC (0.92); this value, however, showed a trend towards statistical difference (p = 0.06) from IC only. Based on this analysis, the cut-off points with the best sensitivity and specificity for each functional variable were selected 14: IC/TLC = 0.28, IC = 75% pred, and FEV1 = 50% pred. As shown in table 3⇓, an IC/TLC ≤0.28 was associated with the highest specificity, positive predictive value, likelihood ratio for positive and negative test results, and overall accuracy to predict a peak V′O2 <60% pred as compared with other variables.

{kind=link}
{kind=link}
Receiver operating characteristic curves of inspiratory capacity (IC)/total lung capacity (TLC; –––), IC % predicted (– – –) and forced expiratory volume in one second (FEV1) % pred (····), as related to a severely reduced maximal exercise capacity (peak oxygen uptake, V’O2, <60% pred). The best cut-off values were 0.28, 75% pred and 50% pred, respectively. The area under the curve (AUC; 95% confidence interval) was 0.92 (0.84–1.00), 0.83 (0.70–0.95) and 0.86 (0.73–0.99) for IC/TLC, IC % pred and FEV1, respectively. Differences between AUCs were IC/TLC versus FEV1, p = 0.30; IC/TLC versus IC, p = 0.06; and FEV1 versus IC, p = 0.66.
Diagnosis performance of different lung function parameters in predicting a severely reduced maximal exercise capacity#
DISCUSSION
The main original finding of the present study was that post-bronchodilator IC/TLC ratio or inspiratory fraction, an index of increased lung volumes, was an independent predictor of maximal exercise capacity in patients with COPD. More specifically, an IC/TLC ≤0.28 was likely to be related to a severely reduced peak V′O2(<60% pred); conversely, higher IC/TLC values were commonly found in less disabled patients. These data, in association with those previously reported by Casanova et al. 6, which related to mortality, indicate that the IC/TLC should be valued as a relevant index of prognosis (≤0.25) and disability (≤0.28) in patients with COPD.
Lung hyperinflation and exercise tolerance in COPD
It has long been recognised that the main pathophysiological abnormality during dynamic exercise in COPD is expiratory flow limitation; its consequences, however, are largely inspiratory and elastic as a result of DH 16. Not surprisingly, several authors have found that a decrease in the operating volumes with bronchodilators, especially the end-expiratory lung volume (EELV), are more likely to be related to clinically meaningful changes in this patient population than traditional measures of airflow 17–20. Similarly, improvement in exercise capacity and dyspnoea after lung-volume reduction surgery was better associated with changes in EELV than with FEV1 21. In the present study, measures of increased lung volumes (IC, RV and IC/TLC) were all associated with worsening maximum exercise capacity (table 2⇑). Reduction in exercise tolerance in patients with lower IC/TLC values (group I) tended to be associated with lower VT and increased ventilation-corrected dyspnoea at peak exercise (table 2⇑). These results seem to indicate that with exercise progression, patients breathed at near-maximum (and less compliant) lung volumes, although exercise IC values were not measured in the present study (see Study limitations).
Physiological significance of IC/TLC
The theoretical advantage of IC/TLC over IC in isolation may be related to the fact that a lower IC/TLC seems to better reflect the deleterious combination of air trapping (increased RV and RV/TLC) plus lung hyperinflation (increased TLC; table 2⇑). Therefore, two patients may present with similar IC which is a widely different fraction of their maximal available volume for lung expansion. In this context, the combination of lower IC/TLC with increased TLC (i.e. a very high EELV) is potentially more harmful than the isolated reduction in IC, since the patient should breathe at his/her near-maximum (and increased) TLC, with negative consequences on the elastic work of breathing and dyspnoea.
A noticeable finding of the present study was the close similarity between the IC/TLC cut-off for severe reduction in peak V′O2 described herein, and that found by Casanova et al. 6 for mortality in COPD. Although the exact nature of the relationship between lung hyperinflation and mortality in COPD is still elusive, it is interesting to note that a low IC/TLC was related to reduced BMI, worse exercise capacity and, marginally (p = 0.10), to decreased DL,CO (table 2⇑), all indicators of poor prognosis in COPD 22.
Clinical implications
Exercise capacity has been associated with disability, increased usage of healthcare resources and even mortality in patients with COPD 23. Resting lung function measurements may be useful in estimating the likelihood of a severe reduction in exercise tolerance 5. The present results show that IC/TLC is a readily available alternative for the prediction of severe disability in COPD, with the advantage of also being associated with mortality 6. From a practical point of view, if a COPD patient presents with an IC/TLC ≤0.28 (or ≤0.25), he/she should be considered at increased risk of respiratory-related disability and death.
Study limitations
A major limitation of the present study is related to the sample size. Therefore, it cannot be ruled out that failure to demonstrate a potential superiority of IC/TLC over other physiological variables was due to an insufficient number of patients with severe-to-very severe lung hyperinflation. In fact, the present results should not be extrapolated for patients with more advanced or milder disease. Another relevant limitation was the lack of IC measurements during exercise, a physiological outcome that has been shown to be superior to resting IC in estimating exercise tolerance in patients with COPD 1. It could be speculated, however, that as patients with lower IC/TLC had substantially increased operating lung volumes at rest, as discussed above, they would tend to present with lower exercise IC. However, recent studies using optoelectronic plethysmography have found a variable behaviour of exercise lung volumes in individual COPD patients, DH being poorly related to static lung volumes 24, 25. Future studies are therefore warranted to evaluate how IC/TLC compares to exercise IC in these patients. Also of importance is that, submaximal exercise tolerance has been found to be more closely related to patientś functional capacity than peak exercise; the accuracy of IC/TLC in identifying patients with reduced tolerance to endurance exercise remains to be investigated 26. Moreover, it is currently unknown whether pre-bronchodilator IC/TLC has any functional significance. Finally, as mentioned, exercise intolerance is a multi-factorial construct where pulmonary-ventilatory, cardiovascular and peripheral factors interact in a complex way; IC/TLC (as any lung function variable) should always be used in association with other indices to estimate the degree of effort intolerance in the individual patient.
In summary, the present study has shown, for the first time, that the post-bronchodilator inspiratory fraction (inspiratory capacity/total lung capacity) is an independent predictor of severely reduced maximal exercise capacity in patients with chronic obstructive pulmonary disease. Considering that this variable has also been previously found to constitute a significant prognostic index in chronic obstructive pulmonary disease 6, the inspiratory fraction should be valued in the functional evaluation of this patient population.
Acknowledgments
The authors would like to thank L. de Moura for language revision, L. Maris Nápolis for assistance with data analysis, the Methods in Epidemiologic, Clinical and Operations Research (MECOR) course (provided by the American Thoracic Society), and C. Gross (University of Washington, Washington, WA, USA), for useful insights on data analysis and interpretation.
- Received March 21, 2006.
- Accepted June 29, 2006.
- © ERS Journals Ltd
References










