





Abstract
For expert pulmonologists, advanced procedures in medical thoracoscopy are the nonroutine and more complex applications of the method. The main current indications are the treatment of infected pleural space, forceps lung biopsy and sympathectomy.
In parapneumonic effusions and empyema, medical thoracoscopy is as a drainage procedure, intermediate between tube thoracostomy and video-assisted thoracoscopic surgery (VATS), which is efficient, significantly lower in cost and avoids surgical thoracoscopy under general anaesthesia. It is essential that it is performed early in the course of the disease and is particularly advisable for frail patients at high surgical risk.
The efficacy of forceps lung biopsy has been demonstrated in diffuse lung diseases, whereas results in localised lung diseases and chest-wall lesions have been less positive. However, VATS is currently the preferred approach for these indications. The technique still maintains its efficacy for visceral pleura and peripheral lung biopsy, in particular in the presence of pleural effusion and lung disorders.
At the present time, thoracoscopic sympathectomy is minimally invasive and is an accepted intervention for patients with a variety of autonomous nervous system disturbances. Essential hyperhidrosis patients, and well-selected patients with other disorders, can be helped with this procedure, which can also be performed by interventional pulmonologists.
SERIES “INTERVENTIONAL PULMONOLOGY”
Edited by J.P. Janssen, M. Noppen and K.F. Rabe
Number 5 in this Series
According to the present authors, the term “advanced techniques” refers to the less frequent and more complex applications of medical thoracoscopy. These applications are part of interventional pulmonology following the direction of modern medicine in which various mini-invasive techniques have become part of different medical fields.
In a way, these applications represent a return to the origins, because thoracoscopy performed by an internist, as was its inventor H.C. Jacobaeus, has, from the onset, dealt with complex interventions, such as the lysis of pleural adhesions, to obtain a therapeutic pneumothorax in tuberculosis, later called “Jacobaeus’ operation” 1, 2.
The current article attempts to give an overview of methods that can be described as nonroutine and represent the areas of application in medical thoracoscopy for expert pulmonologists. These applications can be an objective for those who, having learned and applied the basic techniques, wish to develop them further.
CURRENT INDICATIONS
Thoracoscopic management of the infected pleural space
Complicated parapneumonic effusion and empyema are significant clinical problems. Annually, pleural infection affects ∼60,000 individuals in the USA and carries a mortality of ∼15% 3, 4. They are more common in the elderly and in childhood 3. Risk factors for development include diabetes mellitus, alcohol abuse, aspiration and poor dental hygiene, gastro-oesophageal reflux, rheumatoid arthritis, chronic lung disease and intravenous drug abuse 4, 5. Approximately one-third of cases occur in the absence of any identifiable risk factors 4, suggesting that variation in bacterial virulence or host immune defence may also play important roles in empyema development.
Empyema may develop as a complication of pneumonia, or may follow surgery, trauma, iatrogenic procedures, or, rarely, bronchial obstruction from a tumour or foreign body 6. Pleural infection may also occur as a “primary” infection, without evidence of lung parenchymal infection.
Comprehensive reviews and evidence-based guidelines for the management of complicated parapneumonic effusion and empyema are available 3, 5–7, but they do not deal comprehensively with the role of thoracoscopy, apart from considering it an acceptable approach 3 through surgery 5–7.
In reality, thoracoscopy under local anaesthesia, nowadays called medical thoracoscopy, has been used in Europe since 1910 to diagnose and treat pleurisies, including pleural empyema 8–12.
Pathogenesis and rationale for treatment
The development of pleural infection occurs in the following three stages. 1) The initial “exudative” stage occurs in up to 57% of patients with pneumonia and consists of the formation of a sterile, “simple parapneumonic effusion” 3. Mechanisms likely to be important in effusion formation include increased vascular permeability and leakage following neutrophil migration into the pleural space, and the production of pro-inflammatory cytokines, including interleukin-8 and tumour necrosis factor-α 6. Simple parapneumonic effusions are clear, sterile exudates with a pH >7.3, a normal glucose level and a lactate dehydrogenase (LDH) level <1,000 IU·L-1. The majority of simple parapneumonic effusions resolve with antibiotics and drainage is not usually required 13–15. 2) A subset of patients develop secondary bacterial infection of the pleural effusion, leading to the development of a “complicated parapneumonic effusion”. This results in the characteristic pleural fluid biochemical features of pH <7.2, glucose <35 mg·dL-1 and LDH >1,000 IU·L-1 13–16. Complicated parapneumonic effusions do not usually resolve without drainage of the effusion 16. Persistent pleural infection may eventually result in the accumulation of pus in the pleural space (empyema), which should always be drained. A key feature of this “fibrinopurulent” stage of infection is disturbance of the balance between coagulation and fibrinolysis within the pleural space; inhibition of fibrinolysis and activation of the coagulation cascade results in the formation of fibrin, which coats the pleural surfaces and forms adhesions and fluid loculations, impairing the clinical chest tube drainage of infected fluid 17. 3) The final “organising” stage of pleural infection is characterised by fibroblast growth and proliferation, resulting in the formation of an inelastic, fibrous pleural peel which impairs lung re-expansion. The mechanisms which underlie the development of pleural fibrosis in empyema are poorly understood, although recent work using a rabbit model of empyema has suggested an important role for the fibrogenic transforming growth factor-β1 18.
The treatment of pleural infection is based on antibiotic therapy and complete drainage of the liquid to allow total lung re-expansion. In many cases, treatment with antibiotics alone allows a rapid improvement with cessation of fever, reabsorption of the liquid and recovery. Lack of response to antibiotics, however, demonstrated by the identification of organisms on pleural fluid Gram stain or culture, or a pleural fluid pH <7.2 in the clinical setting of a pneumonic illness, or by the aspiration of frankly purulent pleural fluid 5, 16, is a strong indication for chest tube drainage. Drainage may also be undertaken for symptomatic relief in very large simple parapneumonic effusions. The optimal size of chest tube and duration of drainage remain controversial. In many cases, small-bore (12–14 F) drains are easier to insert, more comfortable and adequate for the drainage of infected pleural collections 19, 20. This is not the case in the presence of frank pus, where larger tubes (>28 F) are needed. The role of therapeutic thoracentesis as an alternative to formal chest tube placement in pleural infection remains unclear. Treatment with serial thoracentesis is attractive, as it may avoid the complications of chest drainage and perhaps allow outpatient management of selected cases 21. Successful treatment of empyema with therapeutic thoracentesis and antibiotics has been reported, but has not yet been compared with formal drainage in randomised controlled trials 4, 22.
The presence of loculations, which are characteristic of complicated parapneumonic effusion and fibrinopurulent empyema, frequently make the effusion resistant to drainage with a single chest tube. In these situations, either intrapleural fibrinolytics 23–27, medical thoracoscopy, video-assisted thoracoscopic surgery (VATS) or, in advanced cases of chronic fibrotic empyema, open surgical decortication is used. There are considerable differences in using these approaches between different hospitals, regions and countries, based more on individual clinical choice than on scientific data.
THORACOSCOPY
For years, thoracoscopy has largely been used in pleural effusion due to lung infection, as an alternative to thoracotomy 12, 28, 29, because it allows the mechanical removal of infected material and permits lung re-expansion 9, 30–32. It is possible to open multiple loculations and aspirate the purulent liquid, removing the fibrinous adhesions, including the layer on visceral pleura. Therefore, it is possible to have a single cavity in which, using an accurately positioned chest tube, subsequent local treatment is facilitated with antiseptic solutions or fibrinolytics. Moreover, the possibility to perform pleural biopsies allows the precise aetiological definition of the disease and aids the diagnosis of occult infections (e.g. tuberculosis) or tumours causing pleural effusion.
Most thoracoscopic empyema treatments are performed and described by surgeons using classical three-entry port intervention under general anaesthesia and double-lumen intubation 28, 29. However, it is important to remember that thoracoscopy in empyema may also be performed by expert medical thoracoscopists 12, 33, 34.
Indications
Generally accepted indications for the use of thoracoscopy in infected pleural space have yet to be agreed 28, 29. Some authors maintain that it should be used before positioning a chest tube, when chest tube insertion is indicated 12. Others consider that it should be used only when a large-calibre chest drain does not bring about reduction of fever and complete radiological resolution of the effusion after 2–3 days 35, 36. When the presence of multiple loculations is observed in the effusion, multiloculated pleural effusion 34, 37 and multiloculated empyema in a fibrinopurulent stage 28, 34, 38, 39 are indicated, and thoracoscopy is appropriate. More recently, the indication for surgical treatment using VATS has been extended to chronic organising empyema, both for debridement before thoracotomic decortication 40 and for thoracoscopic decortication 41.
In this context of differing opinions, an attempt to clarify approaches to the medical and surgical treatments of parapneumonic effusions was given by the American College of Chest Physicians in their guidelines 7 using evidence-based methods. They considered the role of VATS, categorising patients by their risk of poor outcome. These guidelines limit VATS to patients defined as higher risk for poor outcome (categories 3 and 4). Category 3 defines effusions occupying more than half the hemithorax; they may be loculated and have thickened parietal pleura. Category 4 is characterised by the presence of pus in the pleural cavity (“true” empyemas).
These recommendations are, however, based on a single randomised study of only 20 patients 38 and on a historically controlled series of 64 patients 42. The guidelines do not mention medical thoracoscopy, even though the recommendations on VATS could be extended to include it.
Equipment and technique
Equipment and technique are different for medical and surgical (VATS) thoracoscopy 11. Medical thoracoscopy can be performed in an endoscopy suite, under local anaesthetic or conscious sedation, with one or two points of entry and reusable instruments. VATS is a surgical procedure requiring an operating room, general anaesthesia with double-lumen intubation, various points of entry and disposable instruments.
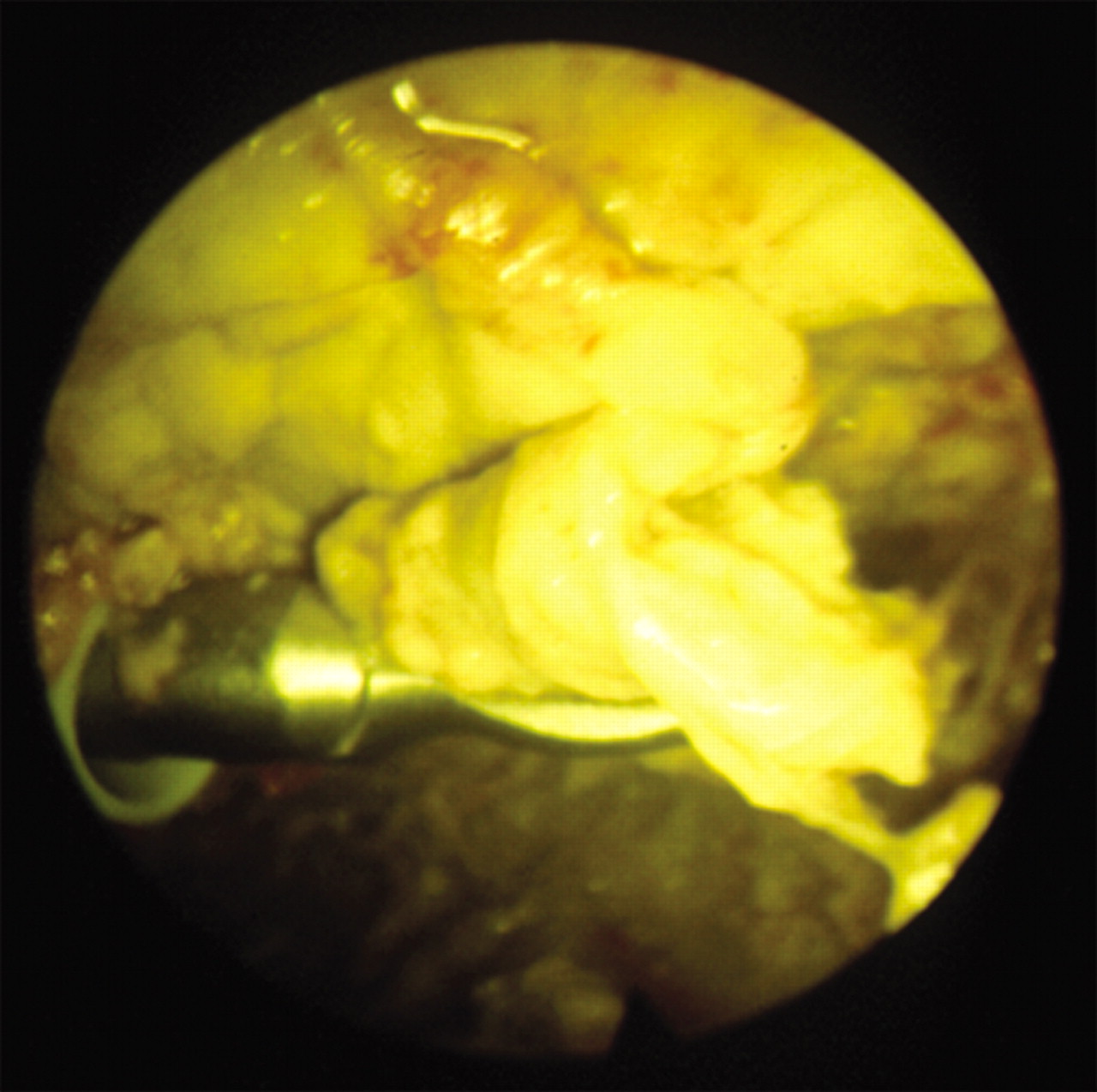
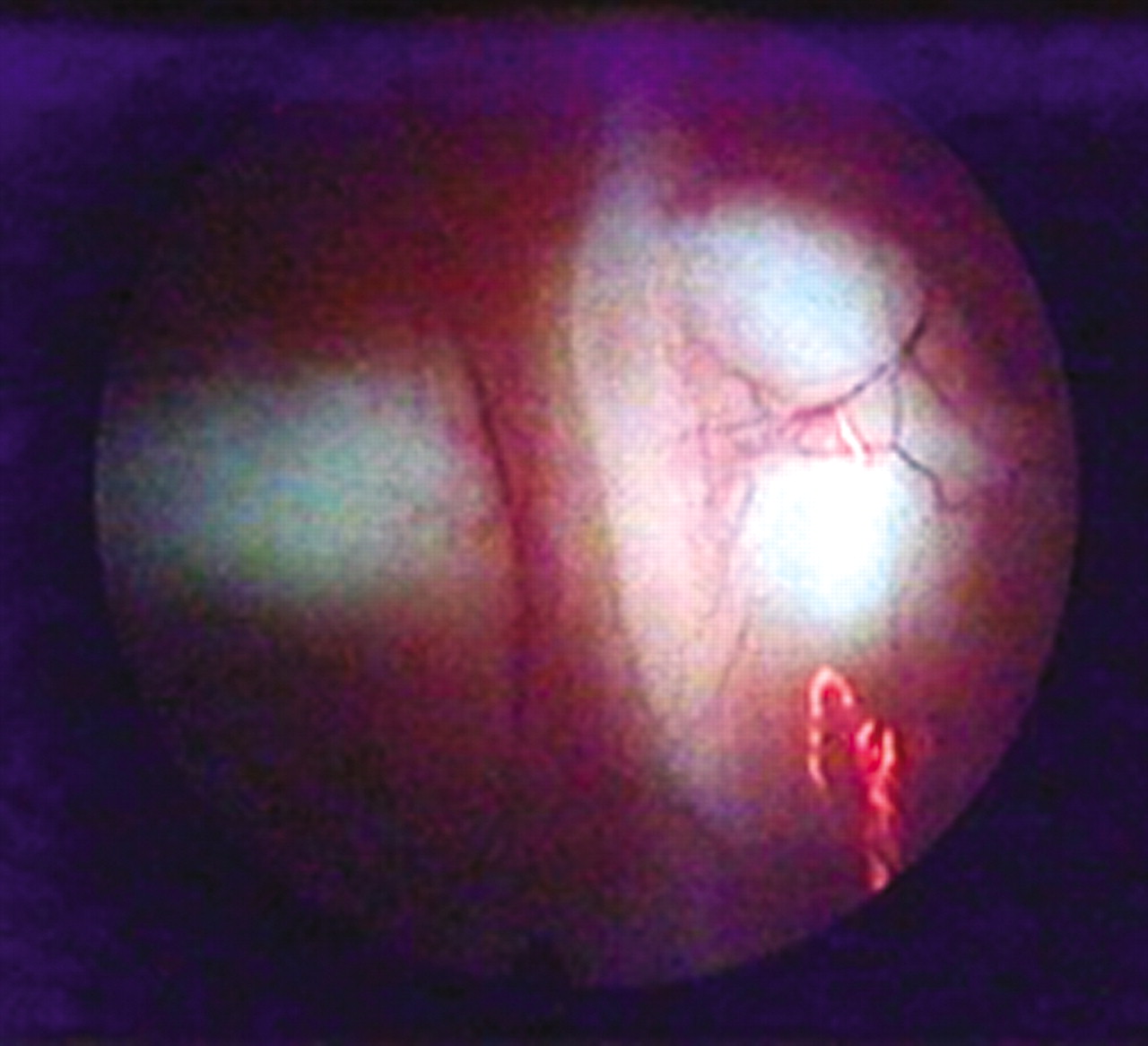
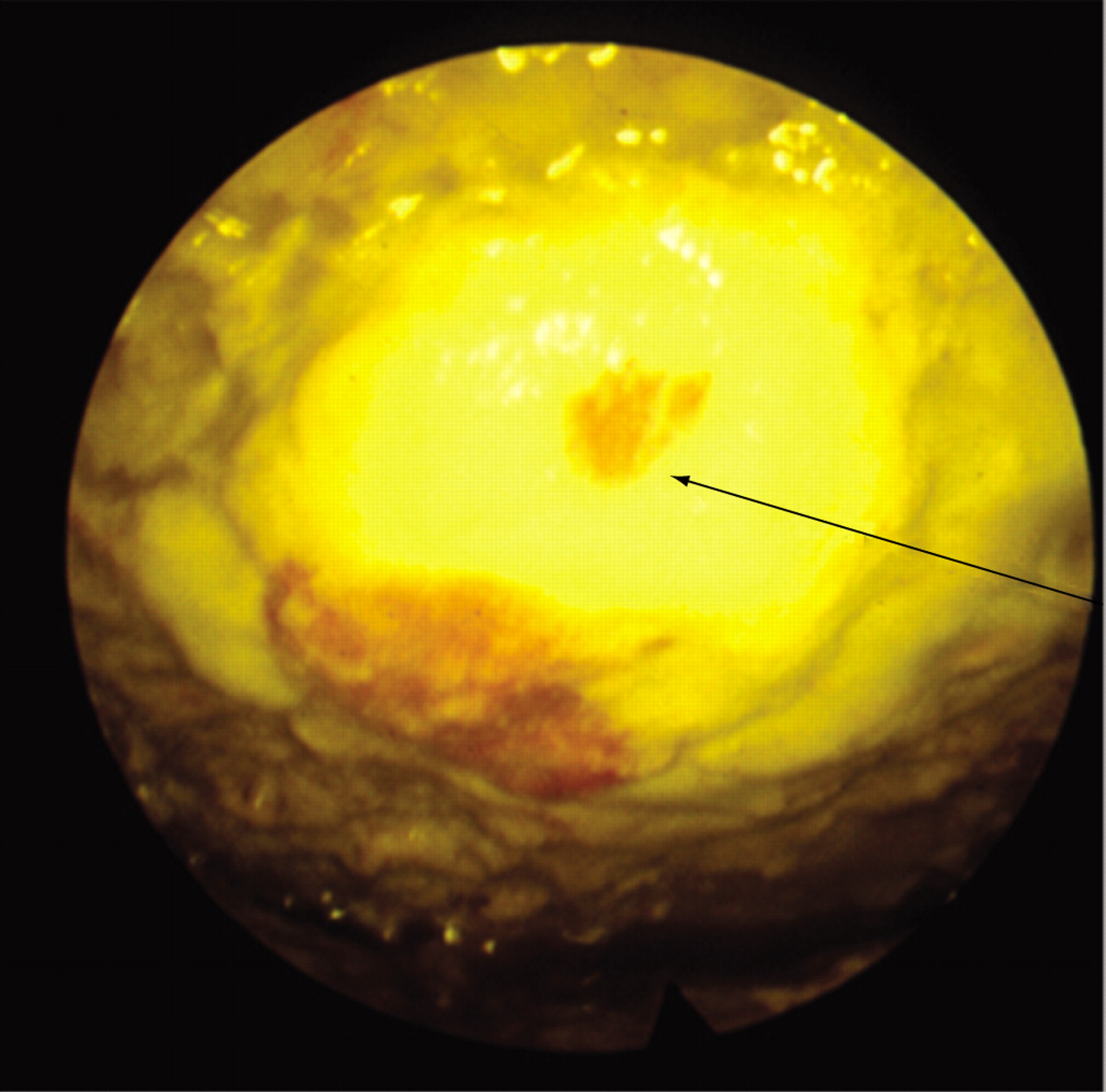
For medical thoracoscopy in pleural space infection, it is advisable to choose the trocar point of entry by ultrasonography to identify the point where the pus collection is largest and the position of the diaphragm, which is often elevated. The examination takes place in the following steps: 1) aspiration of the liquid; 2) exploration of the thoracic cavity to identify loculations (fig. 1⇓) or, less frequently, neoplastic nodules (fig. 2⇓) and, very rarely, foreign bodies (fig. 3⇓); 3) opening the loculations; 4) removal of fibrinopurulent membranes (figs 4⇓ and 5⇓) from the cavity and from parietal and visceral surfaces; and 5) cleansing of the pleural space with saline solution. When the thoracic cavity has been emptied a careful exploration of the pleural surfaces is carried out and, if necessary (fig. 3⇓), biopsies performed. Finally a large-bore chest drain (≥28 F) is introduced, possibly under visual control, to remove dense and viscous pus or fibrin debris.
Results and complications
Cases on the use of thoracoscopy in pleural space infections are mainly related to empyema and are principally surgical. They generally describe favourable results, with primary success rates (complete recovery without the need for subsequent thoracotomy or conversion of VATS to thoracotomy) of 60–100% 29, 39, 43. In the present authors’ experience of medical thoracoscopy, in 69 cases, the primary success rate was 93% and only five patients needed a surgical intervention by VATS or thoracotomy (unpublished data). The best results were obtained when the method was applied early in the course of the disease. The number of patients treated is relatively small and only a few authors 44–47 presented studies with >50 patients.
Surgical studies all agree on the advantages of VATS compared with thoracotomy in terms of less pain, lower costs, shorter hospital stays and better cosmetic results because of the less-invasive technique.
A number of advantages are highlighted for medical thoracoscopy 33, 34, 48. It is mini-invasive, has lower costs compared with VATS and is useful in the treatment of frail patients at high surgical risk. Complications are strictly related to case complexity and are mainly represented by air leaks, which are sometimes prolonged, and by bleeding, with incidences of between 16 42 and 0% 31, 39. In some surgical series comprising patients with heavy comorbidities, some deaths were described 38, 40, 42, 44–46.
Conclusion
Although thoracoscopy has proved useful in the treatment of infected pleural space, in particular in multiloculated empyema where it allows recovery avoiding thoracotomy 28, even today its employment has not been justified by large controlled trials 29. Moreover there are no prospective, controlled studies on the role of medical thoracoscopy in parapneumonic effusions and empyema.
Medical thoracoscopy, as a drainage procedure intermediate between tube thoracostomy and VATS, is significantly lower in cost and can avoid surgical thoracoscopy under general anaesthesia. It is essential that it is performed early on in the course of empyema 12 and it is particularly advisable for frail patients at high surgical risk.
THORACOSCOPIC LUNG BIOPSY
Forceps lung biopsy during thoracoscopy under local anaesthesia has been used for many years by pulmonologists and has been frequently described as an integral technique of the method defined today as medical thoracoscopy 9–11, 49–51. Its employment has been considerably reduced with the advent of VATS, particularly in diffuse lung disease 12, although a study demonstrating its utility was published in 1999 52. Thus, it is important that interventional pulmonologists remain familiar with a technique that can be still relevant.
Indications
Over the years, thoracoscopic forceps lung biopsy has been used in various circumstances in the following situations: 1) in diffuse lung diseases; 2) in localised lung diseases and chest wall lesions; and 3) to sample visceral pleura and peripheral lung in patients with chronic pleural effusions 9, 10, 12.
1) Diffuse lung disease extending to peripheral lung regions, in both immunocompetent and immunocompromised patients, has been an area of application of this technique in the past 53, 54, and was used recently 52 when a diagnosis was not obtained by a simpler method, e.g. bronchoalveolar lavage (BAL) and transbronchial biopsy (TBB). Various diseases, such as granulomatous processes, have been studied 9, in particular sarcoidosis and invasive mycosis, histiocytosis X, idiopathic interstitial pneumonias and carcinomatous lymphangitis. These indications have declined over recent years, as demonstrated by the literature in which there are only two series published after 1990 52, 55. Reduction is also highlighted by the experience of the Lungenklinik Heckeshorn, Berlin, Germany 12, where the use of thoracoscopy for diffuse lung disease, which represented 22% of the examinations performed in the period 1971–1979, fell to 8% in the period 1980–1988 and to 1% in the period 1995–1996. The reasons for this reduction are linked in part to the improvement of imaging techniques, in particular to high-resolution computed tomography, and also to the diffusion of wedge lung biopsy in VATS. In spite of the absence of established guidelines and randomised controlled studies, this has become the procedure of choice to obtain lung tissue when BAL and TBB are nondiagnostic 56–58.
2) The same occurred for the diagnosis of localised lung disease and chest wall lesions, though used infrequently, as demonstrated by the literature 59–62. In the experience of the Lungenklinik Heckeshorn, Berlin, Germany 12, localised lung diseases declined from 12 (1971–1979) to 6 (1980–1988) to 3% (1995–1996), whereas chest wall lesions which were 6 (1971–1979) and 5% (1980–1988), reduced to 2.5% in 1995–1996. For these lesions, VATS is today the procedure of choice as it allows the diagnosis and removal of the lesion 63, 64, sometimes preceded by transthoracic needle aspiration 65.
3) The biopsy of visceral pleura and lung in patients with pleural effusion and visceral pleura involvement or associated lung disease (e.g. mesothelioma, metastatic tumour, suspected carcinomatous lymphangitis, suspected asbestosis) 9 still maintains its importance and significance. It should be noted that if pleural effusions today represent ∼90% of medical thoracoscopy 12, there is frequently a coexistence of effusion and associated lung disease. This is especially important for mesothelioma where the identification of involvement of the visceral pleura, necessarily based on lung biopsy, strongly influences the prognosis 66 and defines a different tumour, node and metastasis stage 67.
Equipment and technique
To obtain a sample of tissue without coagulation, the lung is grasped by optical forceps and pulled toward the trocar using a single port of entry 59. It is also possible to use coagulating forceps, connected to an electrocautery, which allows closure of the lung breach (fig. 6⇓), thereby guaranteeing aerostasis and haemostasis 9, 68. In this case, two ports are needed: one for the endoscope and one for the coagulating forceps (fig. 7⇓). More recently 69, the technique of minithoracoscopy has allowed the use of 5-mm forceps and a mini-endoscope through a single 8-mm trocar. Biopsy should be performed in places away from both interlobar fissures, in which there are large vessels and bullous or cystic formations. It is possible to obtain multiple samples from different areas, and lobes of 5–7 mm and 5–20 mg in weight. At the end of the examination it is essential to put a drain in place to check for possible bleeding or air leaks until complete lung re-expansion is demonstrated by chest radiograph.
Results and complications
In diffuse lung diseases, the diagnostic yield of forceps lung biopsy has been high, indeed comparable to VATS 70–72. The sample quality examined in some studies 52, 73 was high, even if vascular structures were less represented and, for this reason, pulmonary lung disorders are a poor indication for forceps lung biopsy 52. The negative consequences of coagulation on lung tissue are not normally a problem (only 14% in a recent series of cases 52) and can be avoided by limiting coagulation time to 1–2 s 9. In localised lung diseases, such as those cited above 59–62, the diagnostic yield was <50%.
In mesothelioma, where staging is based on visceral pleura involvement, forceps lung biopsy gives a diagnostic yield >90% 9, 74. The extension of metastatic tumours to visceral pleura, for which forceps biopsy is essential for diagnosis, is also frequent, occurring in >80% of cases 75, 76. Forceps lung biopsy simultaneously demonstrated the existence of asbestosis in the presence of effusion 9.
The most frequent complications of the method were represented by air leaks occurring in between 4.1 9 and 14% 53 of cases, similar to the VATS series cited previously 70–72. Bleeding incidence was minimal (0.48%) and mortality was exceptionally low 9.
Conclusions
Forceps lung biopsy has demonstrated its efficacy both in diffuse lung diseases and in pulmonary disorders associated with pleural effusion, whereas results in localised lung diseases and chest wall lesions were less positive. Its limited application amongst pulmonologists who perform medical thoracoscopy remains to be explained. For diffuse lung diseases, it is probable that many believe that “bigger is better” 73 with reference to sample size; for localised diseases, the advent of VATS, which for these indications is superior, has been decisive. The efficacy of the method is indisputable for visceral pleura and peripheral lung biopsy, in particular in the presence of pleural effusion and lung disorder. Interventional pulmonologists should therefore continue the practice of this simple, effective and safe technique.
THORACOSCOPIC SYMPATHECTOMY
Thoracoscopic sympathectomy is defined as the anatomical interruption of the thoracic sympathetic chain (figs 8⇓ and 9⇓) by means of thoracoscopic techniques. The level of interruption (e.g. T3) depends upon the indication and the desired therapeutic effects (e.g. treatment of essential hyperhidrosis) 77.
Thoracoscopic sympathectomy techniques are currently standard approaches for sympathectomy. Whereas open surgical approaches have become obsolete, percutaneous ablation approaches are not widely used because of lower efficacy and higher complication rates 78.
Most thoracoscopic sympathectomy techniques are performed and described by surgeons. Classically, unilateral three-entry port interventions using single-lung, double-lumen ventilation, pleural and sympathetic chain dissection and resection, and post-operative chest drainage are proposed 79. Recently, however, there has been a trend towards less cumbersome, less extensive, simplified one-time bilateral surgical approaches using clipping or diathermy cauterisation, single-lumen intubation, and smaller diameter trocars 80–82. It is worth noting that thoracoscopic sympathicolysis using simple medical thoracoscopic instrumentation and techniques can be safely performed by trained interventional pulmonologists 77–83.
Indications
Accepted indications for thoracoscopic sympathectomy include refractory essential hyperhidrosis (palmar, axillar, facial), and, in selected cases, facial flushing, vascular disorders of the upper limbs (Raynaud's phenomenon, acrocyanosis, arterial insufficiency, Buerger's disease), causalgia, thoracic outlet syndrome, some cardiac disorders (e.g. long QT syndrome) and chronic pancreatic pain syndromes 83.
Equipment and technique
No standard guidelines on equipment and technique are available and very few comparative studies on this subject have been performed. Therefore, most authors have developed, and gained experience with, proper technical approaches. At the present time, in general, thoracoscopic sympathetic interventions (whether performed by surgeons or interventional pulmonologists) are performed in a 1-day setting, under total intravenous anaesthesia. A one-time bilateral procedure using 1–3 small-diameter trocars should be the standard approach. The sympathetic chain can be dissected and resected, cauterised, interrupted or clipped. The level and extent of anatomical interruption depends upon the clinical indication, and should also be kept to a minimum; for example, in essential hyperhidrosis, sympathetic interruption can be limited to the T3 level 84.
Results and complications
Although very few comparative studies are available, short- and long-term results are excellent in hyperhidrosis patients; relief of palmar, axillar and/or facial sweating is obtained in 90–100% of cases 77. Recurrence rates vary between 5–10%, but repeat interventions are often successful. Sporadic (<1%) complications include Horner's syndrome, complicated pneumothorax and haemorrhage necessitating conversion to thoracotomy. No procedure-related mortality has been reported. Compensatory sweating occurs in the majority of patients after sympathetic interruption and may be related to the level of interruption (e.g. T2 interruption increasing its likelihood) and extent (e.g. extensive-level interruption increasing its likelihood). Patients should be extensively informed about the probable occurrence of compensatory sweating. In general, however, this is considered not more than a nuisance and does not affect overall patient satisfaction. However, a small percentage (1–2%) of patients regret the intervention afterwards 85–89.
Conclusion
At the present time, thoracoscopic sympathectomy, sympathicotomy or sympathicolysis is a minimally invasive, accepted intervention for patients with a variety of autonomous nervous system disturbances. Essential hyperhidrosis patients and well-selected patients with other disorders can be helped by this procedure, which can be performed by surgeons or interventional pulmonologists. Short- and long-term results are excellent, severe complications are extremely rare, and side-effects are usually limited to a certain (but acceptable) degree of compensatory hyperhidrosis.
CONCLUSIONS
The treatment of infected pleural space, forceps lung biopsy and sympathectomy are undoubtedly established procedures of advanced medical thoracoscopy, as is the treatment of pneumothorax 90. They should definitely be performed by expert and highly trained thoracoscopists 91 and carried out in specialised centres with sufficient expertise in close collaboration with thoracic surgeons 33.

Typical empyema loculations.

Neoplastic nodule (arrow) on parietal pleura in empyema.

Foreign body (gauze, shown by arrow) in a patient with chronic empyema. The patient had been operated on 2 months previously for major abdominal surgery.

Fibrin membranes in the pleural cavity.
Removal of membranes with forceps.

Scar on lung surface (arrow) after biopsy with coagulating forceps.

Coagulating forceps grasping lung tissue, mesothelioma nodules on parietal pleura are visible in the background.

Thoracoscopic view of the posterior chest wall; the sympathetic chain (indicated by forceps) runs caudally over the rib heads.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The sympathetic chain can be visualised more effectively using blue light during thoracoscopy.
Footnotes
-
Previous articles in this series: No. 1: Bolliger CT, Sutedja TG, Strausz J, Freitag L. Therapeutic bronchoscopy with immediate effect: laser, electrocautery, argon plasma coagulation and stents. Eur Respir J 2006; 27: 1258–1271. No. 2: Vergnon J-M, Huber RM, Moghissi K. Place of cryotherapy, brachytherapy and photodynamic therapy in therapeutic bronchoscopy of lung cancers. Eur Respir J 2006; 28: 200–218. No. 3: Rodriguez-Panadero F, Janssen JP, Astoul P. Thoracoscopy: general overview and place in the diagnosis and management of pleural effusion. Eur Respir J 2006; 28: 409–421. No. 4: Tschopp J-M, Rami-Porta R, Noppen M, Astoul P. Management of spontaneous pneumothorax: state of the art. Eur Respir J 2006; 28: 637–650.
- Received January 30, 2006.
- Accepted May 3, 2006.
- © ERS Journals Ltd
References










