





Abstract
The incidence of asthma has been reported to be associated with obesity. An alternative analysis, of net change in prevalence, does not require exclusion of those with asthma at baseline.
Follow-up data were obtained from 9,552 participants in the European Community Respiratory Health Survey and the Swiss cohort Study on Air Pollution and Lung Disease in Adults. Incidence of asthma was analysed by proportional hazards regression, and net changes in symptoms and asthma status by generalised estimating equations, by obesity group.
Incidence and net change in ever having had asthma were greater in females than in males, and in participants who remained obese compared with those who were never obese (hazard ratio 2.00, 95% confidence interval 1.25–3.20; excess net change 2.8%, 0.4–5.3% per 10 yrs). The effect of being obese on net change in diagnosed asthma was greater in females than in males, but for net change in wheeze without a cold it was greater in males.
The present results are consistent with asthma being more frequently diagnosed in females, especially obese females. These findings may help to explain the reports of a stronger association between asthma and obesity in females than in males.
Despite numerous reports of an association between asthma and obesity, the nature of the association is still controversial 1. Several possible mechanisms have been suggested 2, but no consensus has been reached, and among the unresolved issues is the question of whether the association is stronger in females than in males 3.
If obesity is a cause of asthma then change in body mass index (BMI) should be associated with asthma incidence. Not all longitudinal studies have analysed the effects of both change in BMI and baseline BMI 4–8. Results have been inconsistent 3, with significantly greater incidence reported with greater increase in weight in two studies 9, 10, but not in four other studies 11–14.
Most of the previously mentioned studies adjusted for baseline smoking 4, 5, 7–9, 11, 12, 14 and some reported greater incidence in those who smoked 4, 10, 12, although others found no statistically significant difference in incidence with smoking status 7, 8, 11. However, none of these studies examined the effect of change in smoking habits.
It has been shown that measurement of the incidence of asthma is dependent on the exclusion criterion for cases prevalent at baseline 15, a more sensitive criterion leading to lower estimates. Conversely, an insensitive criterion can give biased estimates of relative risk 16, due to undiagnosed cases in the denominator. Net change in asthma, which is not dependent on exclusion criteria and does not require an age of onset, was previously used by the European Community Respiratory Health Survey (ECRHS) 17.
Data including BMI and smoking were collected in the clinical stage of the ECRHS 18, 19, and in the Swiss cohort Study on Air Pollution and Lung Diseases in Adults (SAPALDIA) 20, 21. SAPALDIA was developed at the same time as the ECRHS and used mostly identical methods and instruments. The current authors estimated incidence of asthma in relation to sex, change in obesity and change in smoking using a sensitive criterion to exclude possible cases at baseline. Net change in symptoms was then analysed in relation to the same factors. Results for net change in asthma were compared with results relating to incidence.
METHODS
Subjects
The ECRHS was a population study carried out in 1991–1993, which included a random sample in centres in most western European countries 18. Each ECRHS survey had a self-completed postal questionnaire (stage 1), followed by stage 2, which included an administered questionnaire and measurement of lung function. Participants in ECRHS I stage 2 were eligible for ECRHS II. The majority of the centres that participated in ECRHS I stage 2 took part in ECRHS II. The first SAPALDIA survey was conducted in a random population sample in eight centres in Switzerland in 1991. Survey II took place in the ECRHS study from 1998–2002 19, and in SAPALDIA from 2001–2003 21. The eight centres in SAPALDIA were chosen to represent the variety of environmental conditions within Switzerland 20. All centres in the first SAPALDIA survey participated in the second survey 11 yrs later, and all participants were invited to the second examination. SAPALDIA participants were aged 20–59 yrs at baseline, but only those aged 20–44 yrs were included in these analyses, for comparability with the ECRHS.
Respiratory symptoms and asthma diagnosis
Symptom data, referring to the last 12 months, were taken from the interview-administered questionnaires; the relevant questions were identical in the two studies. Participants were asked: “Have you had wheezing or whistling in your chest at any time in the last 12 months?”, and, if yes, “Have you been at all breathless when the wheezing noise was present?”, and “Have you had this wheezing or whistling when you did not have a cold?”. In addition, responses to the questions “Have you ever had asthma?” and, for those who answered positively, “Was this confirmed by a doctor?”, “How old were you when you had your first attack of asthma?”, “Have you had an attack of asthma in the last 12 months?” and “Are you currently taking any medicines, including inhalers, aerosols or tablets, for asthma?” were included. Participants were also asked “Have you had an attack of shortness of breath that came on following strenuous activity at any time in the last 12 months?” and “Have you been woken by shortness of breath at any time in the last 12 months?”. The latter two questions were used only to exclude undiagnosed asthmatics from the incidence analysis.
BMI
BMI was calculated for each participant at each survey as weight in kilogram divided by the square of height in metres. Height and weight were recorded prior to lung function assessment. Measurement of height was to the same or better standard in the follow-up surveys; therefore, height at follow-up was used in each calculation of BMI. Categories of BMI at each survey were defined as underweight (BMI <20), normal weight (BMI 20–<25), overweight (25–<30) and obese (≥30). A priori, the current authors decided to analyse change in BMI in four categories, due to the stronger relationship of incident asthma with obesity than with “overweight but not obese” in most studies. Calculations demonstrated that despite the smaller size of the obese category the study had greater power to detect a relationship with obesity than with being overweight. The categories were: 1) not obese at either survey; 2) obese at both; 3) change from not obese to obese; and 4) change from obese to not obese.
Smoking
Information on smoking history was collected in the interviewer-administered questionnaire at each survey. For participants who answered “yes” to the lead question (“Have you ever smoked for as long as a year?”), additional questions were asked on age at starting, amount smoked currently, whether they had stopped or cut down, and amount smoked previously. Seven categories of change in smoking status were derived from data that were unambiguous 22. Participants with ambiguous information were excluded from the analyses. The number of new smokers and those who started and stopped again between surveys were too few for analysis. Never-smokers, sustained quitters (stopped before first survey), smokers (at each survey), quitters (stopped between surveys) and re-starters were included 22.
Statistical analysis
Incidence of asthma was estimated with ever-asthma as the outcome, and the following criterion to exclude those with diagnosed and undiagnosed asthma at baseline 16: all those who answered at the first survey that they had ever had asthma or had any of following three symptoms in the last 12 months, wheeze, woken with shortness of breath or an attack of shortness of breath following strenuous exercise. Analysis of incidence was by Cox proportional hazards regression survival analysis, to allow for variable follow-up, in relation to obesity category, smoking, sex, and age group (20–24, 25–34 and 35–44 yrs at survey I), with clustering by centre and robust standard errors. The timescale was number of years from survey I to reported age of first attack, or to survey II in those without incident of asthma. When age of onset was missing for an incident case it was assumed to be at mid follow-up. Incident cases who reported at survey II that age of onset was at an age prior to age at survey I were treated in two ways. In the first analysis, time of onset was set to 0.1 yrs, and in the second they were treated as having asthma at baseline and omitted. No participant stated that onset was at an age greater than that at survey II.
Absolute change in wheeze and asthma per year of follow-up was estimated using population-averaged, generalised estimating equations for a binomial outcome with identity link, with participants identified as the clustering factor and length of follow-up as an independent variable 17. Associations of change in wheeze and asthma outcomes with sex, smoking group and obesity group were investigated by including interaction terms with length of follow-up, with adjustment for centre or country and age group where possible. Due to problems of convergence of the model when numbers were low, full adjustment and tests of interactions could not be carried out for all outcomes. Results are expressed as unadjusted net change per 10 yrs of follow-up, stratified as necessary, and as unadjusted and adjusted differences between obesity groups. Interactions of sex with smoking group or obesity group were tested when at least one of the main effects was statistically significant at the 1% level.
RESULTS
Response to follow-up
Height and weight were recorded in 27 ECRHS centres at each survey, and in the eight SAPALDIA centres, representing 13 countries in total. There were 20,172 participants in survey I stage 2 of ECRHS or the first SAPALDIA survey, who were therefore eligible for survey II. Of these, 12,829 (33% SAPALDIA) completed the survey II administered questionnaire (6,133 males and 6,696 females). Median follow-up time varied between centres ranging 5.0–11.0 yrs. The overall median was 9.4 yrs with an interquartile range of 8.6–10.8 yrs.
The number of subjects eligible for the study, the number of participants in survey II with BMI and smoking data at each survey in the included groups, and the prevalence of outcomes at baseline are shown in table 1⇓. In total, 9,552 participants had BMI and useful smoking data. Answers regarding presence or absence of symptoms were missing for some subjects, ranging from 12 (0.1%) for wheeze to 112 (1.2%) for current medication, and these subjects were omitted from the analyses of these variables. The prevalence of each outcome at baseline was slightly less in those followed up, and in those who had BMI and unambiguous smoking data at survey II, than in the entire eligible sample. Of participants who reported ever having had asthma, 88% reported that it was doctor diagnosed.
Number and prevalence of symptoms at survey I for all participants in 35 centres, and prevalence at survey I for those with body mass index and smoking data at each survey
Change in BMI
The majority of participants remained in the same BMI category (table 2⇓), 61.6, 63.4 and 59.8% in total, males and females, respectively. A greater percentage of females than males moved to a lower weight category, 4.5% compared with 2.9%, and to a higher weight category, 35.7% compared with 33.6%. Overall, 5.2% of participants remained obese and 7.9% became obese; <1% moved from obese to a BMI <30. Weight gain was substantial in all groups who became obese, including those who were overweight at ECRHS I (table 2⇓).
Change in body mass index(BMI) for participants with smoking data classified by BMI at each survey
Incidence of asthma
There were 208 incident cases of asthma in those without asthma or symptoms at survey I, a rate of 36 per 10,000 person-yrs (95% confidence interval (CI) 32–41). Excluding those who stated, at the second survey, an age of onset prior to the first survey, the rate was 23 per 10,000 person-yrs (95% CI 19–27). Females had a greater unadjusted incidence than males (table 3⇓), and the incidence was greatest in obese females. In the multivariate analysis (table 4⇓), results were qualitatively similar in the two analyses, with some difference in the degree of statistical significance. For all incident cases, the hazard ratio (HR) for females compared with males was 1.47 (95% CI 1.04–2.07, p = 0.028). There was also evidence for differences between the obesity groups (p = 0.01), with greater incidence in those obese at both surveys than those never obese (HR 2.00, 95% CI 1.25–3.20). The interaction between sex and the obesity group was not statistically significant (p = 0.68 adjusted for age and smoking groups; p = 0.61 without adjustment). There was strong evidence for a difference between smoking groups (p = 0.0002), with the greatest incidence in ex-smokers, and lower incidence in other smoking groups compared with never-smokers, with no significant interaction between smoking and obesity groups (p = 0.56), and only weak evidence for an interaction between sex and the smoking group (p = 0.064). However, there was no evidence for increased incidence in those who became obese compared with those who were not obese at either survey (HR 1.12, 95% CI 0.64–1.94).
Incidence of asthma by sex and change in obesity
Asthma incidence by sex, age group, smoking group and obesity group, each mutually adjusted, in participants without asthma or symptoms reported at baseline#
Net changes in asthma and symptoms for males and females
Overall separate net changes for males and females are shown in table 5⇓. Each asthma outcome showed a net increase, “ever had asthma” 3.0% per 10 yrs follow-up (95% CI 2.5–3.5%), as did wheeze with breathlessness and wheeze without a cold (1.1% per 10 yrs, 95% CI 0.3–1.8). The overall net change in nonspecific wheeze was not statistically significant. The increase in wheeze without a cold was confined to males (males 2.1%, females 0.1%, p = 0.009), while females had a greater net increase in ever had asthma (males 2.1%, females 3.9%, p = 0.001) and doctor-diagnosed asthma (males 2.0%, females 3.4%, p = 0.003).
Net change in prevalence of symptoms and asthma per 10 yrs of follow-up in total and by sex
Net changes in relation to obesity groups
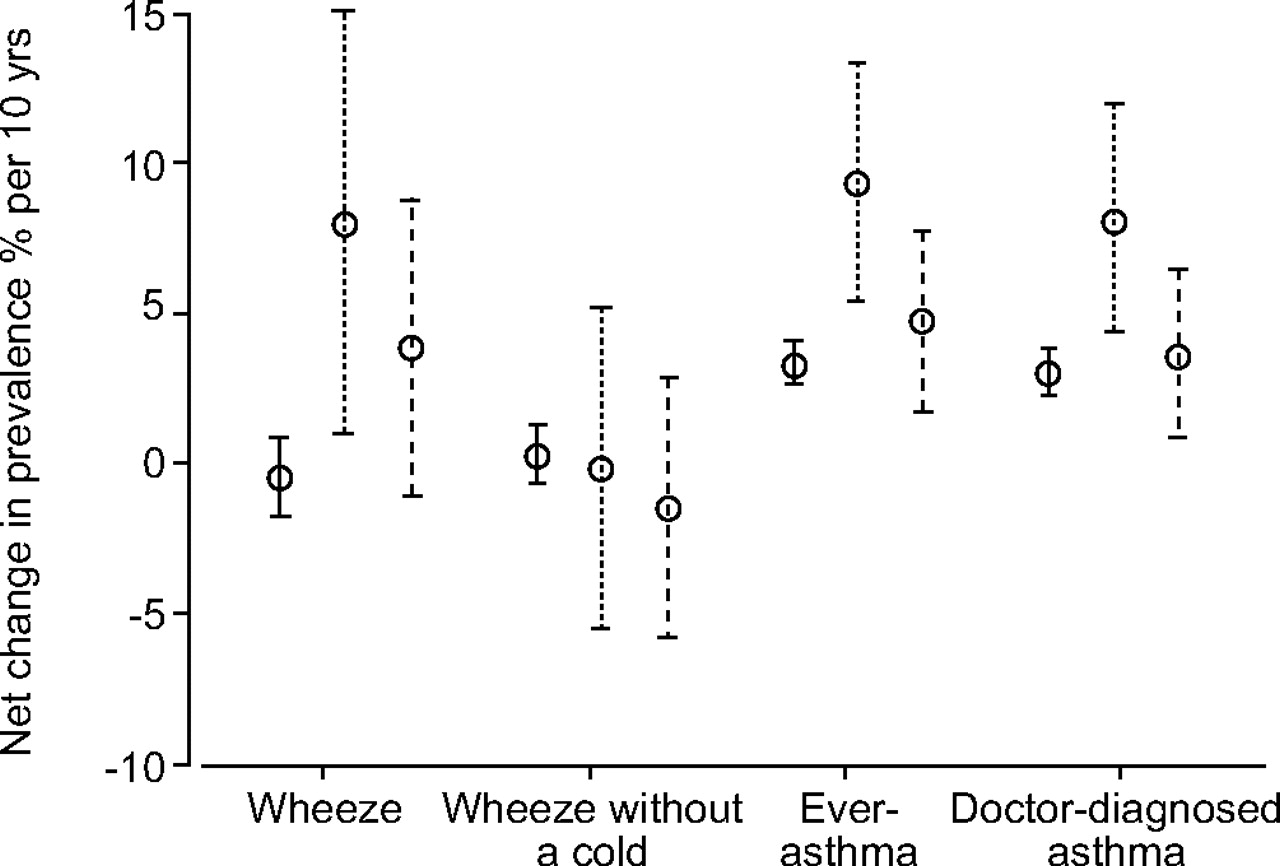
Adjustment for smoking and sex, and for age group and centre or country when also possible, had little effect on differences in net change between obesity groups (table 6⇓). Only overall differences in nonspecific wheeze were statistically significant, including outcomes not shown. The greatest increase in wheeze was in those obese at each survey compared with those not obese at either survey (adjusted difference 7.6% per 10 yrs, 95% CI 2.8–12.4). Figures 1⇓ and 2⇓ display unadjusted net changes for males and females, showing the net increase in wheeze in males and females who were obese at each survey, or who became obese (sex–obesity group interaction p = 0.591). There was a different pattern of asthma in males and females; males showed a small net increase with little difference between the obesity groups, while females showed a larger increase, with the greatest net change in those obese at each survey (sex–obesity group interaction p = 0.050). The pattern for doctor-diagnosed asthma was similar to that for ever-asthma, although the sex–obesity group interaction was not statistically significant (p = 0.153). The net increase in wheeze without a cold was less in females than in males. It was weakly related to obesity in males (p = 0.073), but not in females (p = 0.699); the sex–obesity group interaction was not statistically significant (p = 0.187).

Mean change and 95% confidence interval in net change in prevalence (%) per 10 yrs for selected outcomes in males by obesity group. ____: not obese at either survey; · · · ·: obese at each survey; -------: changed from not obese to obese.
{kind=link}
{kind=link}
Mean change and 95% confidence interval in net change in prevalence (%) per 10 yrs for selected outcomes in females by obesity group. ____: not obese at either survey; · · · ·: obese at each survey; -------: changed from not obese to obese.
Difference in net change in prevalence per 10 yrs of follow-up, unadjusted and adjusted for smoking group and sex
Assessment of heterogeneity
There was a suggestion of a greater net change in ever had asthma in obese females than in males, compared with those not obese, which was largely reflected in doctor-diagnosed asthma. Hence, heterogeneity between countries in net change in obese females was investigated 23. No estimate could be obtained for Estonia (one centre in Tartu) or Belgium (two centres in Antwerp). There was no suggestion of heterogeneity in net change in asthma in obese females between the remaining 11 countries (p = 0.628).
Net changes in relation to smoking groups
There were large differences in net change in wheeze by smoking group (p<0.0001, unadjusted or adjusted), with a decrease in quitters (-10.9% per 10 yrs, 95% CI -14.3– -7.5%) and a large increase in re-starters (8.3% per 10 yrs, 95% CI 3.1–13.6%). The interaction with sex was not significant (p = 0.133). Wheeze without a cold showed a similar pattern of differences, with a decrease in quitters (-5.9% per 10 yrs, 95% CI -8.6– -3.2%), but the biggest increase in continuing smokers (3.4% per 10 yrs, 95% CI 1.6–5.3%). No asthma outcome showed an overall difference between smoking groups; however, for doctor-diagnosed asthma, there was a borderline significant interaction between sex and smoking group (p = 0.060). There was some evidence for differences in doctor-diagnosed asthma between smoking groups in males (p = 0.031), with the greatest net increase in ex-smokers.
DISCUSSION
Neither the analyses of incidence or net change showed an increase in asthma in participants who became obese, but overall incidence and net change were higher in participants who were obese at each survey, compared with those who were never obese. Results for males and females separately suggest that changes in diagnosed asthma do not parallel those in symptoms, and may help to explain the stronger relation of asthma to obesity found in females in some studies.
Overall, 7.9% of participants became obese and 5.2% remained obese. Had the current authors found no difference in either group compared with those who were never obese this might of been attributed to lack of power, but a difference in the smaller of the two groups was detected.
Previous studies that have analysed incidence in relation to weight gain have not distinguished between increases at different points on the weight scale 9–14. This approach could mask a relationship between incidence and the development of obesity, due to the much stronger relation of incidence to obesity than to overweight 5, 6, and the possibly J-shaped relation between incidence and BMI 10. Only two previous studies have found a significant relationship between incidence and weight gain. Height and weight in the Nurses Health Study were self-reported, and weight gain was calculated from that recalled at 18 yrs of age 9. The largest increases in weight were seen in females already obese at age 18 yrs, thus, the relationship may reflect an association with extreme obesity rather than weight gain per se. Beckett et al. 10 reported a relationship of incidence to high BMI and to change in BMI, statistically significant in only females, but with no interaction term reported. The current results do not conflict with the literature, but help to clarify the nature of the relationship of incidence to the development of obesity.
Net change in ever-asthma was greater in those who were obese at both surveys compared with the never-obese group, but only in females. Net change in doctor-diagnosed asthma followed the same pattern. However, net change in wheeze was greater in those who became obese, as well as in those who remained obese, rather than in the never-obese group, in both males and females. There was weak evidence for a relationship of wheeze without a cold to the obesity group but only in males. There were also some differences between symptoms and asthma outcomes in their relationships to smoking groups. Incidence was greater in ex-smokers than in never-smokers, and possibly lower in current smokers. Net change analysis did not support this, suggesting a relationship of change in diagnosed asthma to smoking status in males only.
Thus there is evidence, although weak, for sex modification on the effect of the obesity group on wheeze without a cold and doctor-diagnosed asthma, and of the smoking group on doctor-diagnosed asthma. This evidence suggests that there may be some differential diagnosis linked to the absence of smoking in males and to the presence of obesity in females. If this is the case, the latter appears to be a general finding and not confined to a few countries, as there was no evidence for heterogeneity between countries in the net change in ever-asthma in obese females. In ECRHS I, evidence for a sex difference in the cross-sectional associations of symptoms and asthma with BMI was weak 24. A similar analysis to that presented in the current study, in a population showing a stronger sex difference, would provide valuable information on the possibility of differential diagnostic labelling.
The present authors found that incidence and net change in ever-asthma were both greater in females than in males, while there were some differences in the results by the two methods of analysis in relation to the obesity groups. Incidence of asthma was related to the obesity group overall. It was greater in those who remained obese compared with those not obese at either survey, with no suggestion of a difference between males and females. A greater incidence of asthma in adult females than males has been reported previously by a number of studies 7, 10, 12, 15, 25–27. Two of these studies shared some participants with the current study 15, 28 but from a small number of centres, and the studies were conducted using a postal questionnaire rather than an interview-administered questionnaire. Not all studies have found a statistically significant difference in incidence in young adult males and females 5, 13, 28, 29. Differences in the definition of asthma and in the exclusion criterion for cases at baseline will affect absolute estimates of incidence, making comparisons between studies difficult. It is known that insensitive exclusion criteria may bias relative risk 16, and hence also HRs, so that these too may not be comparable.
A date of onset was only available for analysis of incidence for ever-asthma. Other outcomes were analysed using net change. Doctor-diagnosed asthma showed a greater net increase in females than in males. Overall, net change in wheeze without a cold was significantly greater in males than in females, which was not explained by differences in smoking. There was no significant difference in net change between males and females in the other outcomes.
There are several reasons why incidence and net change analysis may give different results. Net change is comprised of incidence and remission, a factor associated with each in consistent directions has a large effect on net change, while a factor associated either positively or negatively with both incidence and remission may show no relationship with net change. Net change analysis avoids the need to choose a criterion to omit participants with asthma at baseline, and to use a date of onset, and is applicable to all outcomes. As was shown by the high proportion of incident cases of asthma who reported age of onset before the first survey, there is poor recall of this. The 95% limits of agreement for recall of age of first attack of asthma were wide, ranging -11.4–11.6 yrs for those with onset before survey I.
The current study provides no evidence for increased asthma in those who became obese. Net change in asthma was raised in those who were obese at each survey compared with those who were not obese, but only in females. The net increase in ever-asthma and doctor-diagnosed asthma was greater in females than in males, but the net change in wheeze without a cold was greater in males. The present results are consistent with wheeze increasing in individuals who become obese, but of asthma being more frequently diagnosed in females, especially obese females. These findings may help to explain the stronger association between asthma and obesity in females than in males which was found in some studies.
Acknowledgments
ECRHS Co-ordinating Centre: P. Burney (Project Leader); S. Chinn (Statistician); D. Jarvis (Principal Investigator); J. Knox (Project Coordinator); C. Luczynska† (Principal Investigator); J. Potts (Assistant Statistician); S. Arinze (Data Manager).
ECRHS Steering Committee: J.M. Antó and J. Sunyer (Institut Municipal d'Investigació Mèdica (IMIM-IMAS), Universitat Pompeu Fabra (UPF), Barcelona, Spain); P. Burney, S. Chinn, D. Jarvis, J. Knox and C. Luczynska (King's College London, London, UK); I. Cerveri (University of Pavia, Pavia, Italy); R. de Marco (University of Verona, Verona, Italy); T. Gislason (Iceland University Hospital, Reykjavik, Iceland); J. Heinrich and M. Wjst (GSF – Institute of Epidemiology, Neuherberg, Germany); C. Janson (Uppsala University, Uppsala, Sweden); N. Künzli (University of Basel, Basel, Switzerland and University of Southern California, Los Angeles, CA, USA); B. Leynaert and F. Neukirch (Institut National de la Santé et de la Recherche Médicale (INSERM), Paris, France); J. Schouten (University of Groningen, Gronigen, the Netherlands); C. Svanes (University of Bergen, Bergen, Norway); P. Vermeire (University of Antwerp, Antwerp, Belgium).
ECHRS List of Principal Investigators and Senior Scientific Team: P. Vermeire, J. Weyler, M. Van Sprundel and V. Nelen (South Antwerp and Antwerp City, Belgium); R. Jogi and A. Soon (Tartu, Estonia); F. Neukirch, B. Leynaert, R. Liard and M. Zureik (Paris, France), I. Pin and J. Ferran-Quentin (Gronoble, France); J. Heinrich, M. Wjst, C. Frye and I. Meyer (Erfurt, Germany); T. Gislason, E. Bjornsson, D. Gislason, T. Blondal and K.B. Jorundsdottir (Reykjavik, Iceland); M. Bugiani, P. Piccioni, E. Caria, A. Carosso, E. Migliore and G. Castiglioni (Turin, Italy), R. de Marco, G. Verlato, E. Zanolin, S. Accordini, A. Poli, V. Lo Cascio and M Ferrari (Verona, Italy), A. Marinoni, S. Villani, M. Ponzio, F. Frigerio, M. Comelli, M. Grassi, I. Cerveri and A. Corsico (Pavia, Italy); J. Schouten (Gronnigen, the Netherlands), M. Kerkhof (Geleen, the Netherlands); A. Gulsvik, E. Omenaas, C. Svanes and B. Laerum (Bergen, Norway); J.M. Antó, J. Sunyer, M. Kogevinas, J.P. Zock, X. Basagana, A. Jaen and F. Burgos (Barcelona, Spain), J. Maldonado, A. Pereira and J.L. Sanchez (Huelva, Spain), J. Martinez-Moratalla Rovira and E. Almar (Albacete, Spain), N. Muniozguren and I. Urritia (Galdakao, Spain), F. Payo (Oviedo, Spain); C. Janson, G. Boman, D. Norback and M. Gunnbjornsdottir (Uppsala, Sweden), K. Toren, L. Lillienberg, A.C. Olin, B. Balder, A. Pfeifer-Nilsson and R. Sundberg (Gothenburg, Sweden), E. Norrman, M. Soderberg, K. Franklin, B. Lundback, B. Forsberg and L. Nystrom (Umea, Sweden); D. Jarvis and B. Harrison (Norwich, UK), D. Jarvis, R. Hall and D. Seaton (Ipswich, UK).
Centres taking part at their own expense: A. Taytard and C. Raherison (Bordeaux, France), J. Bousquet and P. Demoly (Montpellier, France); K. Richter (Hamburg, Germany); M. Osborne, S. Buist, W. Vollmer and L. Johnson (Portland, OR, USA).
SAPALDIA Senior Scientific Team: Ph. Leuenberger (Co-director), R. Bettschart, G. Bolognini, O. Brändli, M. Brutsche, L. Burdet, M. Frey, M.W. Gerbase, W. Karrer, R. Keller, B. Knöpfli, L. Nicod, A.P. Perruchoud, M. Pons, Th. Rochat, E. Russi, F. Schwarz, J.M. Tschopp, and J.P. Zellweger (all pneumology); U. Ackermann-Liebrich (Co-director), A. Morabia, J. Schwartz, E. Zemp Stutz (all epidemiology); J.C. Barthélémy and J.M. Gaspoz (both cardiology); W. Berger (genetic and molecular biology); A. Bircher and K. Blaser (both allergology); S.H. Downs (epidemiology and statistics); D. Gold (epidemiology, cardiology and pneumology); N. Künzli (epidemiology and expoure); U. Neu and P. Straehl (both exposure); N.M. Probst Hensch (epidemiology and genetic and molecular biology), C. Schindler (statistics); P. Schmid-Grendelmeyer (allergology); A. von Eckardstein (clinical chemistry).
SAPALDIA Scientific Team at Coordinating Centre: L. Bayer-Oglesby (exposure), S.H. Downs (epidemiology and statistics), D. Felber Dietrich (cardiology), M. Imboden (genetic and molecular biology), D. Keidel (statistics), P. Städele-Kessler (statistics), and M.W. Gerbase (pneumology).
SAPALDIA scientific team at local study sites: C. Burrus, D. Felber Dietrich, U. Egermann, M.W. Gerbase, R. Gimmi, A. Kick, N. Lutz, and R. Keller.
The coordination of ECRHS II was supported by the European Commission, as part of their Quality of Life programme.
The following bodies funded the local studies in ECRHS II included in this paper: FWO (Fund for Scientific Research)-Flanders Belgium (grant code: G.0402.00), University of Antwerp, Flemish Health Ministry (Belgium); Estonian Science Foundation (Estonia); Institut Pneumologique d'Aquitaine, Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, Ministere de l'Emploi et de la Solidarite, Direction Generale de la Sante, CHU de Grenoble, Comite des Maladies Respiratoires de l'Isere, Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, CHU de Grenoble, Ministere de l'Emploi et de la Solidarite, Direction Generale de la Sante, Aventis (France), Direction Régionale des Affaires Sanitaires et Sociales Languedoc-Roussillon, Ministere de l'Emploi et de la Solidarite, Direction Generale de la Sante, UCB-Pharma (France), Aventis (France), Glaxo France, Programme Hospitalier de Recherche Clinique-DRC de Grenoble 2000 no. 2610, Ministry of Health, Direction de la Recherche Clinique, CHU de Grenoble (France); GSF-National Reasearch Centre for Environment & Health, Deutsche Forschungsgemeinschaft (DFG; grant code MA 711/4-1GSF-National Research Centre for Environment & Health, DFG (grant code FR 1526/1-1; Germany); Icelandic Research Council, Icelandic University Hospital Fund (Iceland); University of Verona; Italian Ministry of University and Scientific and Technological Research (MURST); Glaxo-SmithKline Italy, Italian Ministry of University and Scientific and Technological Research (MURST), Local University Funding for research 1998 & 1999 (Pavia), ASL 4 Regione Piemonte, AO CTO/ICORMA Regione Piemonte, Ministero dell'Università e della Ricerca Scientifica, Glaxo Wellcome spa (Verona; Italy); Norwegian Research Council, Norwegian Asthma & Allergy Association (NAAF), Glaxo Wellcome AS, Norway Research Fund (Norway); Fondo de Investigaciones Santarias (FIS; grant code: 97/0035-01, 99/0034-01 and 99/0034-02), Hospital Universitario de Albacete, Consejeria de Sanidad, Public Health Service (grant code: R01 HL62633-01), CIRIT (grant code: 1999SGR 00241)), Basque Health Dept (Spain); Swedish Heart Lung Foundation, Swedish Foundation for Health Care Sciences & Allergy Research, Swedish Asthma & Allergy Foundation, Swedish Cancer & Allergy Foundation (Sweden); National Asthma Campaign (UK); American Lung Association of Oregon, Northwest Health Foundation, Collins Foundation, Merck Pharmaceutical (USA).
Financial support for ECRHS I for centres in ECRHS II was provided by the following Institutes: Belgian Science Policy Office, National Fund for Scientific Research; Ministère de la Santé, Glaxo France, Insitut Pneumologique d'Aquitaine, Contrat de Plan Etat-Région Languedoc-Rousillon, CNMATS, CNMRT (90MR/10, 91AF/6), Ministre delegué de la santé, RNSP, France; GSF, and the Bundesminister für Forschung und Technologie, Bonn, Germany; Ministero dell'Università e della Ricerca Scientifica e Tecnologica, CNR, Regione Veneto grant RSF n. 381/05.93, Italy; Norwegian Research Council project no. 101422/310; Dutch Ministry of Wellbeing, Public Health and Culture, the Netherlands; Ministero Sanidad y Consumo FIS (grants No. 91/0016060/00E-05E and No. 93/0393), and grants from Hospital General de Albacete, Hospital General Juan Ramón Jiménenz, Consejeria de Sanidad Principado de Asturias, Spain; The Swedish Medical Research Council, the Swedish Heart Lung Foundation, the Swedish Association against Asthma and Allergy; National Asthma Campaign, British Lung Foundation, Department of Health, South Thames Regional Health Authority, UK; United States Department of Health, Education and Welfare Public Health Service (grant No. 2 S07 RR05521-28), USA.
Research support for SAPALDIA was provided by the National Science Foundation of Switzerland (grant no.32 65896.01, NF 32 59302.99, NF 32 47BO 104283, NF3247BO 104288, NF 3233-048922.96 (N. Künzli), and NF 32-32450.92 (E. Zemp)), the Federal Office for Forest, Environment and Landscape, the Federal Office of Public Health, the Federal Office of Roads and Transport, the Cantons Basel-Stadt, Basel-Land, Geneva, Zurich, Ticino, Aargau, Luzern, the Swiss Lung League and the Lung League of Geneva, Ticino, Zurich and Basel Stadt/Basel Landschaft.
- Received December 21, 2005.
- Accepted July 13, 2006.
- © ERS Journals Ltd
References










