





Abstract
The present study investigated the association between reported parental smoking and exhaled nitric oxide fraction (FeNO) in young children.
In total, 78 children (24 females, mean age 51.3 weeks) were recruited. Fourteen lived with one smoking parent and eight with two smoking parents. FeNO was measured using the modified single-breath technique.
Mean±sd FeNO levels were 33.0±18.9, 38.3±15.0 and 48.3±14.7 ppb for children with no, one and two smoking parents, respectively. There was a significant linear trend across the groups and, after controlling for other relevant factors, a significant difference between the groups.
In the present study, exposure to environmental tobacco smoke was associated with increased exhaled nitric oxide fraction in young children. Furthermore, there was evidence of a dose–response relationship between childhood exhaled nitric oxide fraction and the number of smoking parents.
Exhaled nitric oxide (exhaled nitric oxide fraction; FeNO) appears to reflect allergic airway inflammation 1. It may also be a biomarker for the acute respiratory effects of exposure to airway irritants 2 and is raised as a result of exposure to a range of ambient, domestic and occupational pollutants 3–5. Environmental tobacco smoke (ETS) is an important airway irritant; however, the effect of ETS on FeNO in children is unclear.
Active smoking is associated with reduced FeNO 6. Controlled exposure to ETS can also decrease levels 7, 8; however, in most epidemiological studies, no effect of passive smoke exposure on FeNO has been observed 9–11. The situation is less clear in infants where parental smoking may either decrease 12, 13 or increase 13 tidal FeNO, with the relationship being dependent on maternal atopy. As part of a study of lung function and airway inflammation in young children, the current authors investigated the relationship between reported parental smoking and FeNO in this age group.
METHODS
Subjects and protocol
The results from 78 children (24 females, mean age 51.3 weeks (range 13–106 weeks)), who had FeNO data and had been well for at least 2 weeks before testing, were included in the present study. Thirty-six children had a history of wheeze. All children underwent pulmonary function testing that included measures of lung volumes (forced expiratory volume in 0.5 seconds (FEV0.5)) and FeNO. Children were studied in the supine position, asleep following an oral dose of chloral hydrate (60–100 mg·kg-1). FeNO was measured using the single-breath technique, as described previously 14. The expiratory flow was 11 mL·s-1. FEV0.5 was measured using the raised-volume, rapid thoraco-abdominal compression technique 15. FeNO was always measured first. The study was approved by the Medical Ethics Committee of the Princess Margaret Hospital for Children and written informed consent was obtained from the parents.
Statistical analyses
FeNO was normally distributed. FEV0.5 values were converted to a z-score (FEVz), using data collected previously 16, and were also normally distributed. Parental smoking was categorised both as a binomial variable (yes/no) and by the number of smokers (none/one/both). The effect of parental smoking on both FeNO and FEVz was analysed using unpaired t-tests and ANOVA. A dose–response relationship between the number of smoking parents (0, 1 or 2) and FeNO was determined using the Chi-squared test for linear trend. Multiple linear regression was used to examine the association between paternal smoking and FeNO adjusted for the child's age, sex, health status (history of wheeze versus no history of wheeze), doctor-diagnosed eczema and FEVz, as well as maternal atopy. Maternal atopy was defined as at least one positive reaction to a skin prick test. Finally, given previous findings in infants 13, a multiple linear regression model was constructed to assess whether maternal atopy modified the relationship between parental smoking and FeNO. This model included the two main effects (parental smoking and maternal atopy) and an interaction term (maternal atopy × parental smoking). Data are expressed as mean±sd.
RESULTS
Twenty-two children lived with at least one smoker. Of these, 14 lived with one smoking parent and eight with two smoking parents. Fathers (13 out of 14) were the main smokers in one-parent-smoking households. There were no differences in age, height, weight, FEVz, proportion of wheezers, doctor-diagnosed eczema and maternal atopy between children from smoking and nonsmoking households (table 1⇓).
Anthropometric, lung function and exhaled nitric oxide fraction(FeNO) data for children grouped according to the number of smoking parents
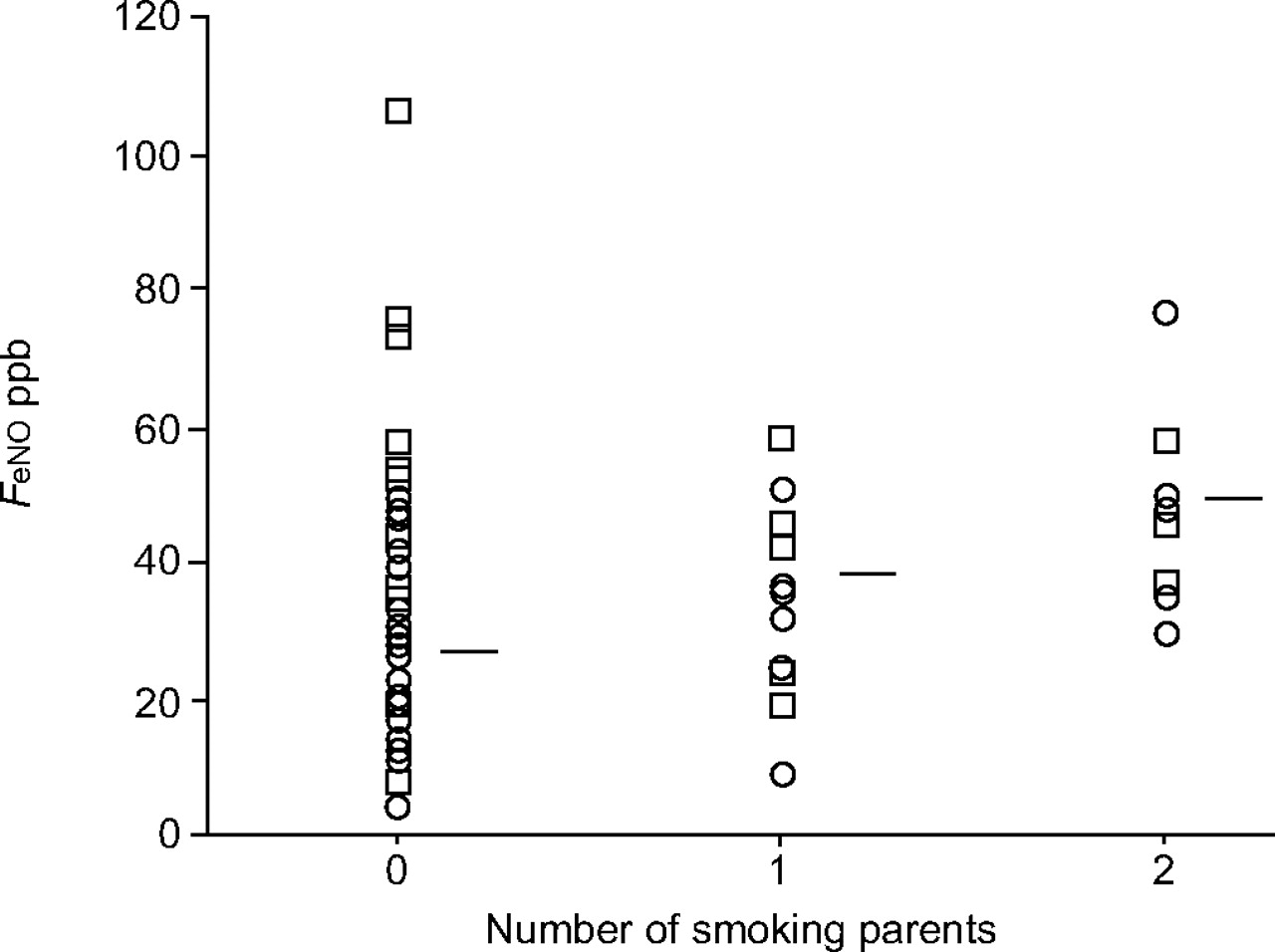
Children who had at least one smoking parent had higher FeNO than children in nonsmoking homes (p = 0.052). Mean±sd FeNO values for the two groups were 41.9±15.3 and 33.0±18.9 ppb, respectively. Within the smoking group, FeNO was 38.3±15.0 and 48.3±14.7 ppb for those with one and two smoking parents, respectively (fig. 1⇓; table 1⇑). The difference between the three groups was not significant (p = 0.07), but there was a significant dose–response relationship across the three groups (p = 0.023). In the linear regression model, parental smoking significantly increased FeNO after controlling for other factors in both the two- (9.4 ppb; 95% confidence interval (CI) 0.4–17.7 ppb in smoking group, p = 0.041) and three-group analyses (table 1⇑). In the three-group analysis, children with two smoking parents had significantly greater FeNO than children in nonsmoking homes (+16.6 ppb; 95% CI 2.9–30.4, p = 0.019). Age, sex, maternal atopy, doctor-diagnosed eczema and FEVz were not associated with FeNO. FEVz was also not associated with parental smoking. Finally, there was no significant interaction between maternal atopy and parental smoking on FeNO (p = 0.19).

{kind=link}
Exhaled nitric oxide fraction (FeNO) for children grouped by the number of smoking parents. ——: mean (unadjusted); □: children with a history of wheeze; ○: nonwheezers.
DISCUSSION
In the present study, parental smoking was associated with an increase in FeNO in young children. Furthermore, there was evidence of a dose–response relationship between FeNO and the number of smoking parents. Increased FeNO has previously been reported in infants of smoking atopic mothers 13, whereas it is low in healthy newborns of smoking nonatopic mothers 12, 13. This suggests that the presence of maternal atopy modifies the relationship between maternal smoking and FeNO in young children. In the present study, there was no significant interaction between maternal atopy and parental smoking on FeNO; however, there was insufficient power to adequately investigate such an interaction.
Raised FeNO observed in the present study, as well as in infants of smoking atopic mothers reported elsewhere 13, is interesting as cigarette smoke has mostly been associated with lower FeNO. FeNO is decreased in smokers 6 and can also be reduced immediately after smoking a cigarette 6, 7, although Chambers et al. 17 reported a short-term increase in FeNO directly after smoking a cigarette. Cigarette smoke has been shown to decrease inducible nitric oxide synthase (iNOS) in vitro 18.
The effect of ETS on FeNO is less clear. In controlled exposure studies, passive smoking can cause an acute decrease in FeNO in nonsmoking healthy subjects 7, 8. Most epidemiological studies have not found an effect of parental smoking on FeNO in children 9–11, although Warke et al. 19 reported lower FeNO in exposed compared with unexposed asthmatic children. Most of these studies have used reported parental smoking as the exposure variable. This may not always be a good indicator of exposure for older children 20. However, reported smoking may be a good marker of exposure for young children as they are generally unable to remove themselves from the source. Indeed, Le Seouf et al. 21 found a strong relationship between reported parental smoking and urinary cotinine levels in infants, but only a weak relationship, which decreased with age, in children >2 yrs of age.
The mechanism for increased FeNO in very young children exposed to ETS is not known. It is possible that it may be an early marker of allergic sensitisation. FeNO is strongly associated with atopy in children, even in the absence of disease 9, and there is evidence that pre-natal and early life exposure to ETS increases the risk of allergic sensitisation in young children 22, 23, although the data are not consistent 24. Another explanation is that FeNO reflects the acute irritant effects of exposure to ETS in this age group 13.
There was evidence of a dose–response relationship between the number of smoking parents and FeNO in children. This has not been reported previously; however, as numbers of children with two smoking parents in the present study are small (n = 8), this finding should be treated cautiously. It was not possible to determine whether this was due to increased exposure from having two smoking parents or from maternal smoking alone, as all but one of the one-smoking-parent smokers were fathers. Future studies should include an objective marker of ETS exposure, such as urinary cotinine, to better determine exposure levels. Interestingly, urinary cotinine levels are reported to be highest in infants living with two smoking parents, although levels are still significantly higher in infants with smoking mothers only compared with those with smoking fathers only 25.
Frey et al. 13 found that both pre- and post-natal smoking were, separately, associated with increased FeNO. In the present study, it was not possible to differentiate between the effects of pre- and post-natal ETS exposure, as only one of the smoking mothers did not smoke during pregnancy.
In the present study, FeNO was measured using a single-breath technique 14. Frey et al. 13 measured infant FeNO during tidal breathing and also found an association with parental smoking. There is no standard method for collecting FeNO in very young children, although some measure of flow needs to be considered 13, 26. The consistency of the results, despite different collection methods, suggests that these may not be just chance findings.
In an earlier paper on FeNO in the same cohort, the present authors reported that levels were significantly higher in females than males. After a small increase in subject numbers, this association was not evident in the current analyses. In a Swiss study 13, infant males had higher FeNO than females, but only in the offspring of mothers with atopic disease. Maternal atopy had no influence on sex differences in FeNO in the present study (data not shown).
In the present study, parental smoking was associated with increased exhaled nitric oxide fraction in children with evidence of a dose–response relationship. The mechanisms for this are unknown. Potential mechanisms and issues, such as the separate effects of pre- and post-natal environmental tobacco smoke exposure and the influence of maternal atopy on the association between parental smoking and exhaled nitric oxide fraction, should be explored further.
Acknowledgments
The authors would like to thank all children and their parents for participating in the study, and E. Pascoe for statistical advice.
- Received January 17, 2006.
- Accepted June 9, 2006.
- © ERS Journals Ltd
References










