





Abstract
Levels of the soluble form of the triggering receptor expressed on myeloid cells (sTREM)-1 are elevated in severe sepsis. However, it is not known whether sTREM-1 measurements can distinguish milder bacterial infections from noninfectious inflammation. The present authors studied whether serum sTREM-1 levels differ in community-acquired pneumonia, exacerbations of chronic obstructive pulmonary disease (COPD), asthma and controls, and whether sTREM-1 may be used as a surrogate marker for the need for antibiotics.
Serum sTREM-1 levels in 150 patients with pneumonia, COPD and asthma exacerbations and 62 healthy controls were measured.
Serum sTREM-1 levels were significantly elevated in pneumonia (median 295.2 ng·mL-1), COPD (280.3 ng·mL-1) and asthma exacerbations (184.0 ng·mL-1) compared with controls (83.1 ng·mL-1). Levels were higher in pneumonia and Anthonisen type 1 COPD exacerbations than in type 2 and 3 COPD and asthma exacerbations. The area under the receiver operating characteristics curve for sTREM-1 as a surrogate marker for the need for antibiotics was 0.77.
Serum levels of the soluble form of the triggering receptor expressed on myeloid cells-1 were elevated predominantly in pneumonia and Anthonisen type 1 COPD exacerbations versus type 2 and 3 chronic obstructive pulmonary disease exacerbations, asthma and controls. Serum levels of the soluble form of the triggering receptor expressed on myeloid cells-1 has moderate but insufficient accuracy as a surrogate marker for the need for antibiotics in lower respiratory tract infections.
- Antibiotics
- asthma
- chronic obstructive pulmonary disease
- pneumonia
- respiratory infections
- soluble form of the triggering receptor expressed on myeloid cells-1
Community-acquired pneumonia (CAP), acute exacerbations of chronic obstructive pulmonary disease (COPD) and asthma cause substantial mortality and morbidity 1–4. While pneumonia is usually caused by bacterial infections 1, 2, COPD exacerbations may be triggered by either bacterial or viral infections 5, and bacterial infections are rare in asthma exacerbations 4. Similarly, while clinical practice guidelines recommend routine empiric antibiotics for all cases of pneumonia 1, 2, 6, antibiotics are usually only recommended in Anthonisen type 1 COPD exacerbations (presence of dyspnoea, increased sputum volume and purulence) 3, 5, 7, and not in Anthonisen type 2 and 3 COPD and asthma exacerbations 4. Serum procalcitonin measurements are more sensitive and specific for the diagnosis of sepsis than white blood cell counts and serum C-reactive protein levels 8, and may guide antibiotic therapy in lower respiratory tract infections 9–11. Nevertheless, the search for the ideal laboratory marker for nonsevere sepsis continues.
The triggering receptor expressed on myeloid cells (TREM)-1 is a member of the immunoglobulin (Ig) superfamily. Its expression is upregulated on phagocytic cells in the presence of bacteria or fungi 12, 13. Levels of TREM-1 and soluble TREM-1 (sTREM-1) are elevated in bronchoalveolar lavage fluid in pneumonia 14–16. Plasma sTREM-1 levels are also raised in critically ill patients with sepsis, especially severe sepsis and septic shock, compared with patients without infection 17–19. However, the value of plasma/serum sTREM-1 in diagnosing the presence of infection in noncritically ill patients has not been evaluated.
The current authors therefore aimed to study whether serum sTREM-1 levels differ among patients with CAP, exacerbations of COPD, asthma and controls, and if sTREM-1 may be used as a surrogate marker for the need for antibiotics.
PATIENTS AND METHODS
Study design and subjects
From December 2004 to April 2005, all 156 patients admitted to the respiratory unit at the present authors’ hospital with the diagnoses of CAP, acute exacerbation of COPD or asthma were identified early, by twice-daily ward visits by two investigators (J. Phua and T.K. Lim), and with the cooperation of attending physicians who informed the investigators of such patients upon admission. Six patients refused participation; therefore, 150 patients were prospectively enrolled within 24 h of admission after obtaining their informed consent. In total, 62 healthy blood donors to the local blood bank served as anonymous controls. The study protocol was approved by the National Healthcare Group Domain Specific Review Board (Singapore, Singapore).
Pneumonia was diagnosed in the presence of a new chest radiograph infiltrate with at least one of the following: cough; sputum; dyspnoea; fever >38.0°C; abnormal breath sounds; leukocytosis >10,000 cells·mm-3; and leukopenia <4,000 cells·mm-3 1, 2. The Global Initiative for Chronic Obstructive Lung Disease guidelines were used to define COPD 3. A COPD exacerbation was diagnosed when dyspnoea, sputum production or purulence increased 7, without radiological consolidation. Asthma was defined according to the Global Initiative for Asthma guidelines 4. An asthmatic exacerbation was diagnosed when dyspnoea, cough, wheezing or chest tightness increased without radiological consolidation. The diagnoses were independently verified by the two investigators upon enrolment, and reviewed again upon discharge or death. Patients with suspected pulmonary tuberculosis and bronchiectasis were excluded.
The patients were followed prospectively until discharge or death. Variables recorded included: patient demographics; symptoms and signs; prior antibiotics; routine blood tests; microbiological cultures; chest radiograph findings; pulmonary function tests (for COPD patients); outcomes (length of stay and mortality); and complications (intensive care unit admission and mechanical ventilation). In the respiratory unit, sputum and blood cultures were performed on admission, before antibiotics, according to the discretion of the managing physicians, usually only on patients with severe pneumonia, and not routinely on patients with COPD and asthma exacerbations, as per clinical practice guidelines 3, 4, 6. Serum procalcitonin and C-reactive protein (CRP) levels were recorded if ordered by the managing physicians. Patients with pneumonia were stratified according to severity (sepsis or severe sepsis including septic shock) 20 and the Pneumonia Severity Index (PSI) score and class were calculated 21. Patients with COPD were stratified according to the Winnipeg criteria 7. Antibiotics were prescribed by attending physicians without interference by the investigators. However, for the purpose of the study, in accordance with practice guidelines 1–7, all patients who were given the diagnoses of pneumonia and Anthonisen type 1 COPD exacerbation upon discharge or death by the investigators, were labelled by the investigators as requiring antibiotics, and all other patients (Anthonisen type 2 and 3 COPD exacerbations, asthma and controls) as not requiring antibiotics.
Methods
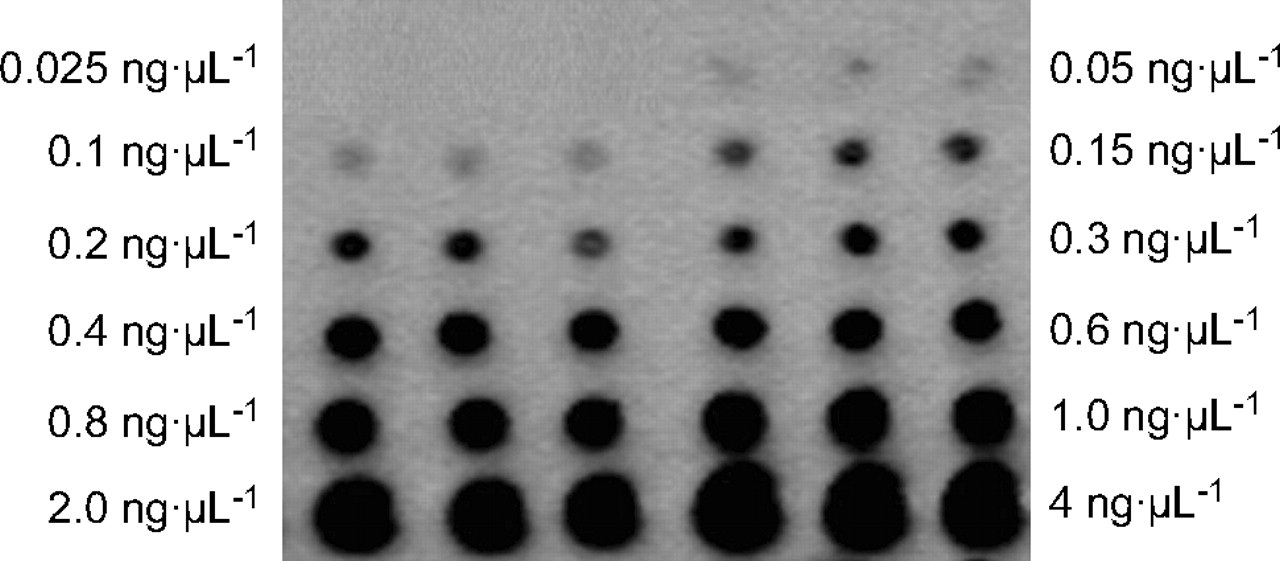
Blood levels of sTREM-1 were measured using an immunoblot technique 14, with in-house modifications. Peripheral venous blood (5–7 mL) was sent immediately in a plain tube to the laboratory. The clotted blood was centrifuged at 800×g for 10 min to harvest the serum. Absolute (100%) ethanol was added to the serum, kept in an icebath for 30 min, and recentrifuged at 16.1×g for 20 min. The supernatant was removed and SDS-PAGE buffer was added to re-dissolve the precipitate. One microlitre (μL) of each of the pre-treated samples and the serially diluted (0.05, 0.1, 0.15, 0.2, 0.3, 0.4, 0.6, 0.8 and 1.0 ng·mL-1) sTREM-1 standards (human Trem-1/Fc Chimera protein 1278-TR; R&D Systems, Minneapolis, MN, USA) were spotted onto the same nitrocellulose membrane, in triplicate (fig. 1⇓). The membrane was incubated for 1 h (to prevent nonspecific binding) with 5% bovine serum albumin in Tris base-buffered saline-0.1% Tween 20 (TBS-T), pH 7.6, followed by three washes with TBS-T buffer. The membrane was first incubated for at least 2 h with anti-sTREM-1 monoclonal antibody (dilution 1:500, IBQ02; R&D Systems), followed by thorough rinsing with TBS-T buffer, and then with the secondary antibody, horse-radish peroxidase-conjugated goat anti-mouse IgG (dilution 1:5000; Molecular Probes Inc., Eugene, OR, USA) for 1 h at room temperature. All traces of excess unbound antibody were removed by more washing with TBS-T buffer before the chemiluminescent signals were developed using the SuperSignal® West Pico Chemiluminescent Substrate (Pierce, Rockford, IL, USA). The signals were detected by the MULTI GENIUS Bio Imaging System (Syngene, Frederick, MD, USA) and the spot intensities (volumes) were determined using the GeneTools software (Syngene). The serum sTREM-1 levels in the patient samples were extrapolated from the calibration curve generated from the sTREM-1 standards run in triplicates on the same membrane (0.05–1.0 ng per μL or per application). The sensitivity, reproducibility (both intrabatch and interbatch) and linearity of the assay were assessed.

Representative chemiluminescent signals obtained from the protein dot blot array for generation of the calibration curve. Known concentrations (0.025–4.0 ng·μL-1) of recombinant soluble form of the triggering receptor expressed on myeloid cells-1 were dotted onto the PVDF membrane in triplicate, and the average for each concentration was used for construction of the calibration curve. At the 0.025 ng·μL-1 concentration, the signals were too faint to show up consistently; at 0.05 ng·μL-1, all triplicates were detectable in numerous repeat runs, thus verifying the sensitivity of the assay as 0.05 ng·μL-1.
The sensitivity of the dot-blot array assay for sTREM-1 was 0.05 ng·μL-1, defined as the lowest consistently detectable concentration in all 10 replicates. Defining this as the limit of the analytical sensitivity, absolute sTREM-1 levels could be assigned to most study subjects, including 49 controls; the remaining 13 had sTREM-1 levels <0.05 ng·μL-1. To include them in the statistical analysis, the current authors arbitrarily assigned them as having sTREM-1 values of 0.05 ng·μL-1.
The intrabatch coefficient of variation (CV%), calculated from five replicates of each of three sTREM-1 concentrations (1.0, 2.0 and 3.5 ng·μL-1) within the same batch run was 7.7, 7.0 and 4.0%, respectively. The interbatch CV%, calculated from five replicates of these sTREM-1 concentrations (1.0, 2.0 and 3.5 ng·μL-1) obtained from six separate runs was 4.0, 6.3 and 7.29%, respectively. When the calibration curve was plotted for sTREM-1 concentrations from 0.05–4.0 ng·μL-1, data points could not be fitted into a single linear regression line. The linear regression, y = 3839.5x, only applied to values between 0.05 and 0.8 ng·μL-1 (fig. 2⇓). Beyond 0.8 ng·μL-1, the linear relationship between the intensity of the signal generated and the analyte concentration was no longer valid due to a saturation effect, i.e. a limitation exists in the dynamic range of sTREM-1 levels extrapolated from the calibration curve. Most of the present study samples gave signals that could be extrapolated, with values between 0.05 and 0.8 ng·μL-1. For those few samples with signals >0.8 ng·μL-1, one could either report these as >0.8 ng·μL-1 or calculate the sTREM-1 levels after diluting and re-running the sample. To avoid use of decimals, serum sTREM-1 values were reported as ng·mL-1.

A representative calibration curve of the soluble form of the triggering receptor expressed on myeloid cells (sTREM)-1. The linear relationship between the signal intensities and the serum sTREM-1 concentrations was valid within a dynamic range of sTREM-1 concentrations between 0.05 ng·μL-1 and 0.8 ng·μL-1. The regression equation was y = 3839.5x and the correlation coefficient was 0.9627. This calibration curve was useful for extrapolating the unknown sTREM-1 levels for most (>90%) of the study subjects directly or after dilution of the samples with values >0.8 ng·μL-1.
During clinical validation of the above protein dot-blot array method, parallel Western blots with the anti-sTREM-1 monoclonal antibody were performed to characterise the products measured in the patient samples. A single band was consistently found in the Western blots, demonstrating that the protein measured by the dot-blot array assay was sTREM-1. As Western blotting is time consuming and expensive, the current authors opted to use only the protein dot-blot arrays thereafter to measure serum sTREM1 levels.
All laboratory analyses were carried out with the laboratory staff having no prior knowledge of the patients' diagnoses and other clinical details. Similarly, attending physicians and investigators were blinded to the sTREM-1 values throughout the study. The sTREM-1 values were only released to the investigators at the end of the study, once the clinical diagnoses had been made.
Statistics
Values were expressed as mean±sd for parametric data and median (range) for nonparametric data. Group differences were compared for parametric data by ANOVA. To compare nonparametric data (including sTREM-1 levels) between groups, the Kruskal–Wallis test was first performed for overall differences, followed by the Mann–Whitney U-test to compare specific groups. A receiver operating characteristics (ROC) curve was constructed to determine various cut-off values of sTREM-1, with respect to the need for antibiotics. The accuracy of chosen threshold sTREM-1 values was defined as the sum of concordant cells divided by the sum of all cells in the two-by-two table. Statistical significance was set at an α-value of 0.05. All p-values were two-sided.
RESULTS
Of the 150 enrolled patients, the investigators revised the attending physicians' diagnoses in four patients from COPD to asthma. There was no further revision of the diagnoses between enrolment and discharge or death. In total, 72 patients had pneumonia, 43 had COPD, and 35 had asthma. As mentioned previously, 62 healthy blood donors served as controls.
The patients' baseline characteristics are shown in table 1⇓. Patients with pneumonia had higher temperatures than patients with COPD or asthma (p<0.001). Patients with pneumonia had higher leukocyte counts than patients with COPD (p = 0.019). Of those with pneumonia, 46 had unilobar consolidation, while 26 had multilobar consolidation. Of those with COPD, the latest mean post-bronchodilator forced expiratory volume in one second (FEV1) was 44±15% of predicted, forced vital capacity (FVC) was 62±17% pred, and FEV1/FVC was 50±11%. Microbiological data are shown in table 2⇓.
Patients' characteristics
Microbiological data
Median sTREM-1 levels varied significantly among the various groups (p<0.001), with the highest levels in patients with pneumonia, followed by COPD, asthma and controls (table 1⇑ and fig. 3⇓). Serum sTREM-1 levels were significantly higher in pneumonia (p<0.001), COPD (p<0.001) and asthma (p<0.001) than controls, and significantly higher in pneumonia than asthma (p = 0.027).

Boxplots of serum levels of the soluble form of the triggering receptor expressed on myeloid cells (sTREM)-1 in patients with pneumonia (n = 72), chronic obstructive pulmonary disease (COPD; n = 43), asthma (n = 35) and controls (n = 62). Boxplots represent the 25th and 75th percentiles, with the internal horizontal lines showing the median and T bars the 10th and 90th percentiles. ○: outliers. The p-values refer to comparisons between groups using the Mann–Whitney U-test. #: p = 0.027; ***: p<0.001.
Among patients with pneumonia, those without severe sepsis had median (range) sTREM-1 levels of 303.3 (38.9–824) ng·mL-1, those with severe sepsis had median levels of 403.2 (28.4–929.1) ng·mL-1, while those with septic shock had median levels of 262.5 (44.7–721.4) ng·mL-1 (p = 0.27). Eight patients were assigned to PSI risk class I, 11 to class II, 15 to class III, 20 to class IV and 17 to class V. There was no relationship between sTREM-1 levels and PSI class. In addition, 20 of the 72 patients with pneumonia received antibiotics for the current illness prior to hospital admission. There was no significant difference in sTREM-1 levels between those who took prior antibiotics and those who did not. There was also no relationship between sTREM-1 levels and microbiological results (including the presence or absence of bacteraemia).
Within the COPD group, the 16 patients with Anthonisen type 1 exacerbations had higher sTREM-1 levels (median (range) 445.2 (79.7–925.2) ng·mL-1) than the 27 patients with Anthonisen type 2 (10 patients) and 3 (17 patients) exacerbations (median (range) 207.0 (57.3–979.4) ng·mL-1, p = 0.031; fig. 4⇓). The COPD patients with type 1 exacerbations had similar sTREM-1 levels to those with pneumonia (p = 0.18) but higher sTREM-1 levels than the asthmatics (p = 0.010). The COPD patients with type 2 and 3 exacerbations showed a trend towards lower sTREM-1 levels than the patients with pneumonia (p = 0.084) but had similar sTREM-1 levels to the asthmatics (p = 0.78).

Boxplots of serum levels of the soluble form of the triggering receptor expressed on myeloid cells (sTREM)-1 in patients with Anthonisen type 1 exacerbations of chronic obstructive pulmonary disease (n = 16) versus those with type 2 and 3 exacerbations (n = 27). Boxplots represent the 25th and 75th percentiles, with the internal horizontal lines showing the median and T bars the 10th and 90th percentiles. ○: outliers. #: p = 0.031.
Of the patients with pneumonia and Anthonisen type 1 COPD exacerbations, 88 were deemed to require antibiotics by the investigators, while 124 patients with Anthonisen type 2 and 3 COPD exacerbations, asthma and controls were deemed not to require antibiotics. Those labelled as requiring antibiotics had significantly higher median (range) sTREM-1 levels (310.52 (8.4–929.1) ng·mL-1) than those labelled as not requiring antibiotics (113.4 (30.0–979.4) ng·mL-1; p<0.001; fig. 5⇓).

Boxplots of serum serum levels of the soluble form of the triggering receptor expressed on myeloid cells (sTREM)-1 in patients with pneumonia and Anthonisen type 1 chronic obstructive pulmonary disease (COPD) exacerbations deemed to require antibiotics by the investigators (n = 88) versus those with Anthonisen type 2 and 3 COPD exacerbations, asthma and controls who were deemed not to require antibiotics (n = 124). Boxplots represent the 25th and 75th percentiles, with the internal horizontal lines showing the median and T bars the 10th and 90th percentiles. ○: outliers. ***: p<0.001.
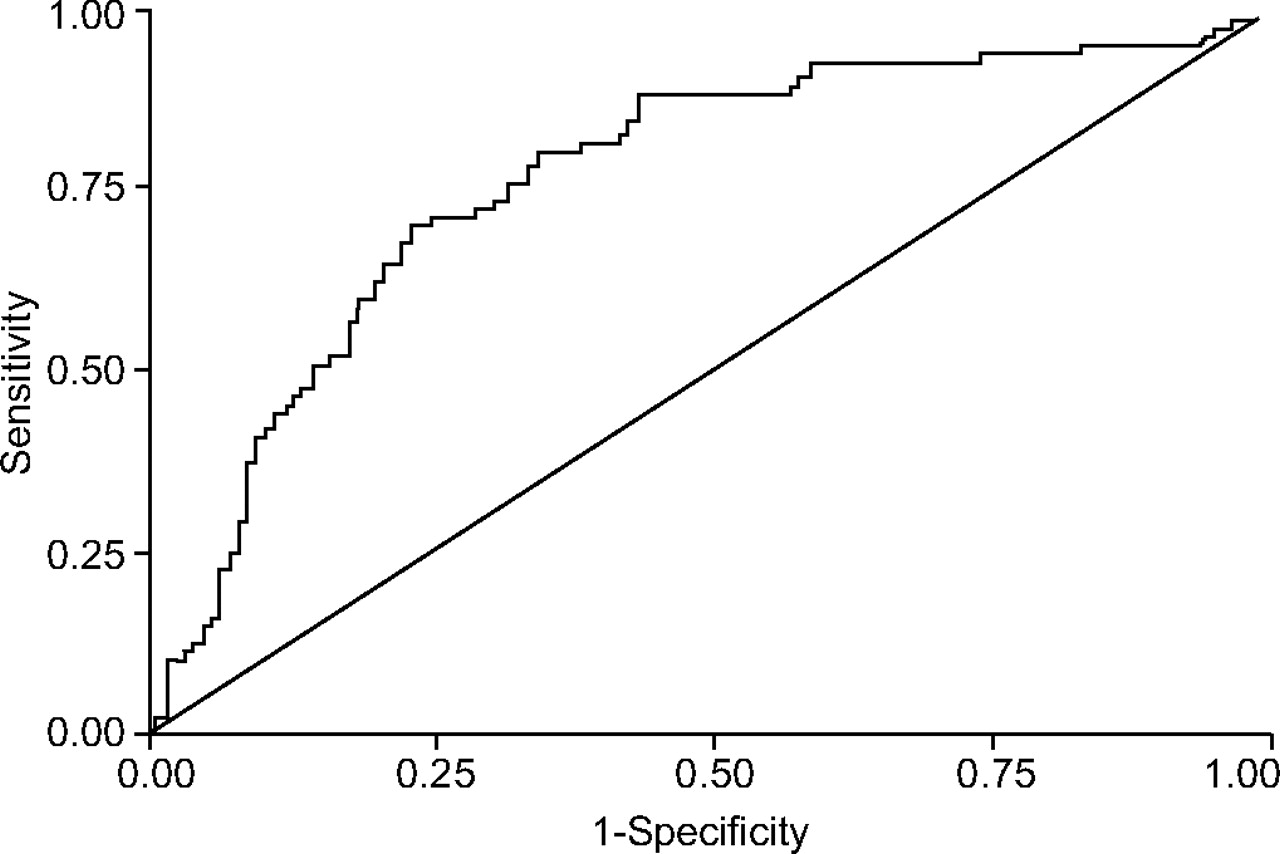
The area under the ROC curve when sTREM-1 levels were used to predict the need for antibiotics was 0.77 (95% confidence interval 0.70–0.84; p<0.001; fig. 6⇓). At a cut-off of 163.4 ng·mL-1, sTREM-1 yielded a sensitivity of 81%, a specificity of 65%, a positive predictive value of 62%, a negative predictive value of 83%, and an accuracy of 72% for differentiating patients labelled as requiring antibiotics from those labelled as not requiring antibiotics. An alternate sTREM-1 cut-off value of 218.8 ng·mL-1 gave a sensitivity of 70%, a specificity of 77%, a positive predictive value of 68%, a negative predictive value of 79% and an accuracy of 74%.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristics (ROC) curve of serum levels of the soluble form of the triggering receptor expressed on myeloid cells-1 to predict the need for antibiotics. The area under the ROC curve was 0.77 (95% confidence interval 0.70–0.84, p<0.001).
Among the patients with pneumonia, COPD and asthma, there was no relationship between sTREM-1 levels and intensive care unit admission, need for invasive ventilation and length of hospital stay (p>0.05). However, there was a trend towards higher sTREM-1 levels for those who died in hospital (median (range) 302.5 (44.7–929.1) ng·mL-1 versus those who survived (median (range) 255.4 (28.4–979.4) ng·mL-1, p = 0.059).
Serum procalcitonin levels were measured in 29 patients (18 with pneumonia, eight with COPD and three with asthma). Levels were higher in pneumonia (median (range) 1.52 (0–261.90) ng·mL-1) than in COPD (median (range) 0.25 (0–0.78) ng·mL-1, p = 0.037) and asthma (median (range) 0 (0–0.09) ng·mL-1, p = 0.012). Serum CRP levels were measured in 40 patients (29 with pneumonia, nine with COPD and two with asthma). Levels were higher in pneumonia (median (range) 12.0 (2.2–33.0) mg·L-1) than in COPD (median (range) 1.9 (0–12.9) mg·L-1, p<0.001) and asthma (median (range) 1.5 (0–2.9) mg·L-1, p = 0.030). There was no significant correlation between sTREM-1 levels and procalcitonin or CRP levels (p>0.05).
DISCUSSION
The current authors found that serum sTREM-1 levels of patients with pneumonia, COPD and asthma exacerbations were elevated compared with controls. The most significant increase was seen in patients with pneumonia and Anthonisen type 1 COPD exacerbations, rather than Anthonisen type 2 and 3 COPD and asthma exacerbations. Serum sTREM-1 was moderately accurate as a surrogate marker for the need for antibiotics in lower respiratory tract infections.
TREM-1 is activated in the presence of toll-like receptors, and its expression is increased in fluids and tissues infected by bacteria and fungi 13, 22, resulting in increased sTREM-1 levels in blood 16, 19, 23. TREM-1 amplifies the inflammatory response by triggering the production of cytokines in sepsis 12, 24, whereas sTREM-1 may act as a negative feedback regulator of the inflammatory response 25. Previous clinical studies have shown that sTREM-1 levels could differentiate critically ill patients with severe sepsis from those without 17, 19. However, it is not known if sTREM-1 levels are increased in relatively mild infection.
This is the first study to show that serum sTREM-1 levels are indeed elevated in both nonsevere and severe CAP. Patients with pneumonia had the highest sTREM-1 levels, significantly higher than those in asthma and controls.
The sTREM-1 levels in the current study differed from those of previous clinical studies 17–19 due to differing study populations and analytical techniques. Several factors contribute to sTREM-1 assay variability in the literature, including, as with any Western blot or immunoblot systems, the substrate used in the final end-point reaction, the antigen (standard) used as calibrator, and the nature and avidity of the primary antibody.
The appropriate substrate choice depends on the enzyme label (horseradish peroxidase versus alkaline phosphatase), desired sensitivity (ng, pg or fg detection limits) and form of signal (light/chemiluminescence emission versus chromogen formation) or method detection (chemiluminescence versus colorimetry measurements). Various substrates were tried in order to optimise this step and SuperSignal® West Pico (Pierce) was chosen. This constituted a major modification from the published method of Gibot and co-workers 14, 17, 18, which used the enzyme substrate chromogen Opti-4CN (Bio-Rad). The chemiluminescent signal generated by SuperSignal® West Pico (Pierce) greatly enhances assay sensitivity compared to the use of chromogenic substrates 26. In addition, reaction performance can be affected by the concentration and purity of the substrate and by other additives and buffer components. Thus, use of the same source and product are essential to enable reproducibility of results.
The type and source of the antigen standards and the primary anti-sTREM-1 antibody used have not been standardised and this can further contribute to discrepancies in reported sTREM-1 levels. Human TREM-1/Fc Chimera protein 1278-TR was used as calibrator and IBQ02 as primary antibody in the assay. In one of the earliest clinical reports on sTREM-1, Gibot et al. 14, used 21C7, a monoclonal murine IgG1 directed against human TREM-1. The current authors manually applied 1 μL of a more concentrated sample to the cellulose membrane; Gibot and co-workers 14, 17 applied 100 μL of their pre-treated, purified sample with the aid of a vacuum created by the Bio-Dot microfiltration apparatus from Bio-Rad Laboratories Inc. (Catalogue No. 170-6545; personal communication with S. Gibot, Service de Reanimation Medicale Hopital Central, Nancy Cedex, France).
In the present study, patients with septic shock appeared to have lower sTREM-1 levels than those without, although this was not statistically significant; these findings are similar to previous data 17. Given that sTREM-1 acts as an anti-inflammatory mediator, these findings may be due to patients with more severe sepsis having a weaker counter inflammatory response 25.
Interestingly, although serum sTREM-1 levels were highest in patients with pneumonia, levels were also elevated in patients with acute exacerbations of COPD and asthma when compared with healthy controls. For COPD, the increase in sTREM-1 levels was mainly due to patients with Anthonisen type 1 exacerbations. While the role of bacteria in COPD exacerbations remains debatable 5, it is possible that the current patients with type 1 exacerbations had higher airway bacterial loads, which triggered systemic inflammation 7, 27, 28 and increased sTREM-1 levels. As for asthma exacerbations, systemic inflammation also occurs 29, and may, therefore, lead to increased serum sTREM-1 levels. Although the expression of TREM-1 is predominantly upregulated by infection rather than noninfectious inflammation 13, this is not exclusive. It has been demonstrated that TREM-1 expression is upregulated during the inflammatory response to noninfected surgery 30.
In this study, it was determined that only patients with pneumonia and Anthonisen type 1 exacerbations required antibiotics 1–7. The area under the ROC curve for sTREM-1 levels with respect to this need for antibiotics was 0.77, which implied moderate accuracy. In a previous study by Gibot et al. 17, the area under the ROC curve to diagnose infection in critically ill patients was higher at 0.97. It is likely that a larger difference in sTREM-1 levels existed in these patients because those with severe sepsis had much more systemic inflammation. Despite the moderate degree of accuracy, it is evident that at this stage, sTREM-1 measurements are not sufficiently useful to guide antibiotic therapy for lower respiratory tract infections without severe sepsis, given the overlap in levels among controls and patients with pneumonia. Besides, the present study's limited data on procalcitonin and CRP showed that these tests may be as discriminative, if not more, than sTREM-1 in this respect. Nevertheless, the current authors emphasise that the present study assessed the use of sTREM-1 as a surrogate marker for the need for antibiotics. Future studies should then assess the outcomes of treatment of lower respiratory tract infections with antibiotics versus placebo based on sTREM-1 levels.
There are several limitations to this study. Cultures were not routinely performed for all patients. While viral aetiologies in the pneumonia group cannot be ruled out, most cases of pneumonia are bacterial in origin 1, 2. Among patients with pneumonia, it was unsurprising that five had Pseudomonas aeruginosa in their sputum, as three of them were diabetic and one had lymphoma 1, 6. Nevertheless, it cannot be concluded with certainty whether the organisms cultured were pathogenic or colonisers, especially as there was no mandate for sputum collection prior to antibiotics. The same applies to COPD and asthma exacerbations. It is difficult to distinguish positive cultures due to true recent infections from colonisers without prior long-term follow-up and molecular typing of bacteria strains. This notwithstanding, the prevalence of positive sputum cultures in the current authors’ COPD patients is consistent with that reported in previous literature 5. Furthermore, although the controls were relatively young, to the current authors’ knowledge, there is no evidence that age affects sTREM-1 levels.
In conclusion, serum levels of the soluble form of the triggering receptor expressed on myeloid cells-1 are elevated predominantly in community-acquired pneumonia and Anthonisen type 1 chronic obstructive pulmonary disease exacerbations, as compared with type 2 and 3 chronic obstructive pulmonary disease exacerbations, asthma and controls. The serum soluble form of the triggering receptor expressed on myeloid cells-1 has a moderate but insufficient degree of accuracy as a surrogate marker for the need for antibiotics in lower respiratory tract infections.
Acknowledgments
The authors would like to thank all the nurses of the respiratory wards and E-Ling Toh of the Clinical Trials Unit of the National University Hospital, Singapore, for the assistance rendered throughout the study.
- Received January 14, 2006.
- Accepted June 23, 2006.
- © ERS Journals Ltd
References










