





Abstract
A mild-to-moderate increase in pulmonary arterial pressure is often associated with severe chronic obstructive pulmonary disease (COPD). Transforming growth factor (TGF)-β is a cytokine involved in the maintenance of integrity of vasculature. The aim of the study was to investigate whether the TGF-β pathway might be involved in the development of pulmonary hypertension associated with COPD.
Surgical specimens from 14 patients undergoing lung transplantation for very severe COPD (forced expiratory volume in one second 17±2% of the predicted value) and from seven donors were examined. The expression of TGF-β1 and TGF-β type II receptor (TGF-βRII), cell proliferation index and structural changes in pulmonary arteries were quantified immunohistochemically.
In severe COPD patients, increased expression of TGF-βRII was observed in both the tunica media and intima, which was associated with a normal proliferation index in both layers. Conversely, significant thickening of the tunica intima, which was not present in the tunica media, was observed, suggesting that mechanisms other than cell proliferation may be involved in intimal thickening.
In conclusion, in the pulmonary arteries of patients with severe chronic obstructive pulmonary disease, there is upregulation of transforming growth factor-β type II receptor expression associated with a normal proliferation index. These findings suggest the activation of an antiproliferative pathway, which might explain the relatively low degree of pulmonary hypertension observed in these subjects.
Chronic obstructive pulmonary disease (COPD) is a disorder characterised by airflow limitation that is slowly progressive and not fully reversible 1. Severe and very severe COPD are usually associated with increased pulmonary arterial pressure 2. This pulmonary hypertension secondary to COPD, albeit usually much milder than primary hypertension, is nonetheless an important risk factor for hospitalisation and shorter life expectancy 3. Pulmonary hypertension secondary to COPD may be due to hypoxic pulmonary vasoconstriction, emphysematous destruction of the capillary bed, excessive shear stress, inflammation and remodelling of pulmonary arteries acting against a background of genetic susceptibility 4, 5.
The most common morphological change in the pulmonary arteries of patients with COPD is thickening of the intimal layer. By contrast, at variance with primary hypertension, the medial layer of the arteries is normal or only mildly thickened 6. These structural changes are often associated with functional impairment of the endothelium 7 and with an inflammatory process in the adventitial layer 8, 9. The mechanisms underlying the development of these structural abnormalities in pulmonary arteries are still unknown.
The role of the transforming growth factor (TGF)-β pathway has been investigated in COPD. Increased expression of TGF-β1 in the airways of smokers with COPD compared to smokers without COPD has been reported 10–12, suggesting a role for TGF-β1 in the development of COPD. By contrast, recent studies on the genetics of COPD suggest a protective rather than a predisposing role for TGF-β1 in COPD 13–15. The TGF-β pathway has been poorly investigated in pulmonary hypertension secondary to COPD, although downregulation of the TGF-β type II receptor (TGF-βRII) has been reported in both primary and secondary pulmonary hypertension 16, 17.
TGF-β is a pleiotropic cytokine with a wide variety of effects on cell proliferation and differentiation and on inflammation. In humans, the TGF-β family includes three isoforms with great structural and functional similarities (TGF-β1, TGF-β2 and TGF-β3) 18. TGF-β regulates cellular processes by binding to three receptors known as types I, II and III. In particular, TGF-β binds either to the type III receptor (TGF-βRIII), which then presents it to the type II receptor (TGF-βRII), or directly to the TGF-βRII. Once activated, TGF-βRII recruits and activates the type I receptor (TGF-βRI). The activated TGF-βRI phosphorylates mothers against decapentaplegic homologue (Drosophila) (Smad) 2 or 3, which then binds to Smad4. The resulting Smad complex is able to translocate into the nucleus, where it interacts with various transcription factors to regulate the transcription of many genes. The final effect depends upon the specific ligand, heteromeric receptor type, downstream signals and transcriptional activation 19.
In order to investigate whether the TGF-β pathway is involved in pulmonary hypertension in COPD patients, the present study examined the expression of TGF-β1 and TGF-βRII in the pulmonary arteries of patients undergoing lung transplantation due to very severe COPD. Given the complexity of the TGF-β pathway, it was decided to examine expression of TGF-β1 and TGF-βRII as they have been already implicated in the pathogenesis of COPD or pulmonary hypertension, respectively 10–17.
METHODS
Subject characteristics
Lung specimens obtained from a group of patients undergoing lung transplantation because of very severe COPD were examined 20. A forced expiratory volume in one second (FEV1) of <25% of the predicted value without reversibility and/or an arterial carbon dioxide tension of ≥7.3 kPa (55 mmHg) (and/or pulmonary hypertension) with progressive deterioration were the main criteria for transplantation. Fourteen COPD patients (11 males and three females) in the age range 45–64 yrs (mean 55 yrs) were included.
The study conformed to the Declaration of Helsinki, and informed written consent was obtained from each subject undergoing transplantation. Each patient underwent a pre-operative interview, pulmonary function tests, chest radiography, ECG, echocardiography, right heart catheterisation and routine blood tests. As a control group, specimens obtained from the unused lung of seven donors whose other lung was used for transplantation (four males and three females; age range 15–60 yrs (mean 34 yrs)) were analysed. All had died of suicide or subarachnoid haemorrhage. No clinical data were available for the control group.
Lung tissue preparation
The lung tissue used for the present study included material from 14 patients undergoing lung transplantation due to very severe COPD. Cold ischaemic preservation lasted 60 and 120 min, respectively, for single and double lung transplantation. Small pieces were cut from all lobes and immediately fixed in Karnovsky’s solution for electron microscopy. The lungs were gently fixed in 10% phosphate-buffered formalin by airway perfusion and processed for sectioning (3 μm). Samples were selected from specimens that showed features of excellent tissue preservation and adequate lung inflation. In particular, large thin blocks of ∼30×25 mm were cut from the subpleural areas of the apical anterior and lingular segments of the upper lobes, as well as the apical and basal segments of the lower lobes. A more centrally placed block was taken to sample the segmented airways and blood vessels. The right lung was sampled in the same way, with the middle lobe being treated in the same way as the lingula 21. Adult control lungs obtained from unused donor lung transplantation were not treated with prostacyclin before preparation.
The local Research Ethics Committee (Padua, Italy) approved the study.
Immunohistochemistry and morphometric analysis
Randomly selected tissue blocks were taken from the subpleural parenchyma, fixed in 4% formaldehyde, embedded in paraffin wax and processed for immunohistochemical analysis of TGF-β1 and TGF-βRII. Briefly, sections underwent antigen retrieval by heating in a microwave oven on high power in 0.01 M citrate buffer (pH 6.0) for 8 min followed by incubation with a mouse monoclonal anti-TGF-β1 antibody (dilution 1:20; Genzyme Diagnostics, Cambridge, MA, USA), a polyclonal anti-TGF-βRII antibody (dilution 1:200; Biotechnology, Inc., Santa Cruz, CA, USA) and the monoclonal antibody MIB-1 (dilution 1:50; Dako, Santa Barbara, CA, USA), which recognises the Ki-67 antigen, a marker of proliferation. The TGF-β1 antibody shows high affinity for human TGFβ-1; however, it may cross-react with other members of the TGF-β family. The antibody used was raised against synthetic peptides corresponding to segments of the amino terminal ends of biologically active TGF-β1. Before incubation with primary antibody, the sections were treated with a biotin-blocking kit (Vector Laboratories, Peterborough, UK) in order to inhibit endogenous biotin. The detection system used was the Vectastain ABC kit (Vector Laboratories), with 3-amino-9-ethylcarbazole as the chromogenic substrate. Sections were counterstained with Mayer’s haematoxylin.
Morphometric measurements of pulmonary arteries were performed using a computerised image analyser (Casti Imaging SC processing; Casti Imaging, Venice Italy) as previously reported 22. Muscular pulmonary arteries (≥10) with a perimeter of <1.5 mm (corresponding to a diameter of ∼0.5 mm) and a double elastic lamina visible over at least half of the circumference were selected for each patient. In order to avoid measurements in tangentially cut vessels, muscular pulmonary arteries with a short:long diameter ratio of less than a third were excluded from the analysis. The areas occupied by the tunica intima and media were measured on sections stained with an antibody directed against smooth muscle actin (M0851; dilution 1:50; Dako, High Wycombe, UK), and revealed with horseradish peroxidase and diaminobenzidine. External and internal elastic laminae were outlined, and the areas occupied by the tunica intima and media were computed and expressed as a percentage of the area encompassed by the external elastic lamina as previously described 22.
TGF-β1- and TGF-βRII-positive cells in the tunica media of the pulmonary arteries were counted. The results were expressed as the number of positive cells per square millimetre of tissue examined. The final result (per patient) is the mean number of TGF-β1- and TGF-βRII-positive cells present in each artery of that patient. Moreover, the results were expressed as the percentage of positive arteries, defined as arteries with at least one TGF-β1- and TGF-βRII-positive cell in the tunica media divided by the total number of arteries examined. The proliferation index was calculated as the percentage of positive arteries, defined as arteries with at least one Ki-67-positive cell in the tunica media and intima divided by the total number of arteries examined.
In order to evaluate the intensity of staining due to expression of TGF-βRII in the tunica intima and media, a semi-quantitative score was applied (0: no staining; 1: weak staining; 2: moderate staining; and 3: strong staining).
The cases were coded and measurements made without knowledge of clinical data.
Statistical analysis
Group data are expressed as mean±sem, or as median and range when appropriate. Differences between groups were analysed using the nonparametric Mann–Whitney U-test for morphological data, and an unpaired t-test for clinical data. Correlation coefficients were calculated using Spearman’s rank method. A probability of p≤0.05 was accepted as significant.
RESULTS
Clinical findings
The clinical characteristics, lung function data and haemodynamic parameters of the patients with very severe COPD are shown in table 1⇓. Five of the 14 patients with severe COPD showed α1-antitrypsin deficiency emphysema. No significant differences in lung function and haemodynamics were observed between patients with and without α1-antitrypsin deficiency. All patients with very severe COPD were ex-smokers with a mean±sem cumulative cigarette consumption of 43±13 pack-yrs. No data were available regarding the presence of chronic bronchitis symptoms. The FEV1 was 17±2% pred, and the diffusing capacity of the lung for carbon monoxide (DL,CO) was 26±6%. The mean pulmonary arterial pressure was 26±3 mmHg, as measured by right heart catheterisation. The left ventricular ejection fraction, obtained on heart catheterisation, was 66±5%, and the right ventricular ejection fraction, obtained echocardiographically, was 50±3%.
Subject characteristics
Before lung transplantation, all COPD patients were treated with inhaled anticholinergic and/or β2-agonists and seven of them with oral steroids (4–8 mg·day-1 methylprednisolone). All patients were clinically stable without evidence of lung infection at the time of surgery.
Immunohistochemical and morphometric findings
On average, 13±2 pulmonary muscular arteries were examined per subject. The arterial perimeter was similar in patients with very severe COPD and donors (647±34 versus 701±55 μm), indicating that arteries of similar size were compared.
TGF-β1 and TGF-βRII were expressed in both the tunica intima and tunica media, with very intense staining in the intimal layer, which precluded precise quantification of the number of positive cells in this layer, where it was only possible to perform semiquantitative scoring of staining intensity.
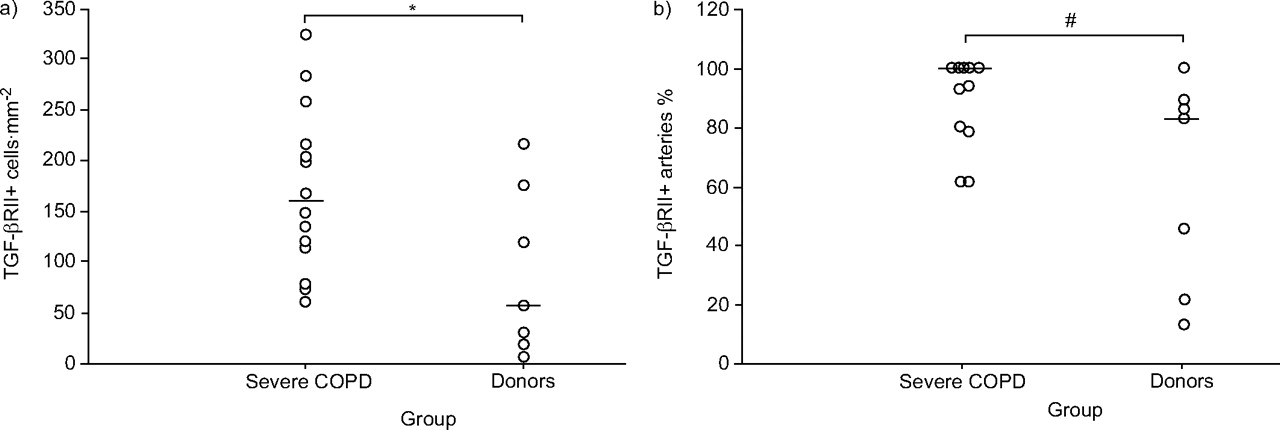
Both the number of TGF-βRII-positive cells (median (range) 158 (61–324) versus 56 (7–216) cells·mm-2; p = 0.05) and percentage of TGF-βRII-positive arteries (100 (62–100) versus 83 (13–100); p = 0.03) were increased in the tunica media of patients with severe COPD compared to donors (figs 1⇓ and 2⇓). Furthermore, there was a marked difference in median numbers of TGF-β1-positive cells between severe COPD and donors, but this difference did not reach significance (17.2 (0.6–395) versus 5 (0–87) cells·mm-2; p = ns). Finally, the percentage of TGF-β1-positive arteries was similar in severe COPD and donors (19 (7–100) versus 18 (0–58); p = ns).

a) Number of transforming growth factor-β type II receptor (TGF-βRII)-positive cells in the tunica media of pulmonary arteries; and b) percentage of TGF-βRII-positive arteries (defined as arteries with at least one TGF-βRII-positive cell in the tunica media divided by the total number of arteries examined) in patients with severe chronic obstructive pulmonary disease (COPD) and donors. Points represent individual patients; horizontal bars represent medians. *: p = 0.05; #: p = 0.035.

Photomicrograph showing transforming growth factor-β type II receptor (TGF-βRII) expression in the tunica media of a pulmonary artery from a patient with a) severe chronic obstructive pulmonary disease and b) a donor. TGF-βRII-positive cell is shown by the arrow (stained brown).
When TGF-βRII staining intensity was evaluated, an increased intensity of staining was found in patients with severe COPD compared to donors in both the tunica intima (2 (0–3) versus 1 (0–1); p = 0.003) and tunica media (1 (0.5–3) versus 0.5 (0–1); p = 0.001).
Morphometric analysis of pulmonary arteries in patients with severe COPD showed an increased thickness of the tunica intima (20.5 (11–27) versus 11 (11–15) μm; p = 0.001), but not of the tunica media (42.5 (26–57) versus 48 (35–60) μm; p = ns) compared to donors (fig. 3⇓). The proliferation index was similar in patients with severe COPD and donors in both the tunica intima (0 (0–26) versus 0 (0–0); p = ns) and media (40 (17–80) versus 30 (0–60); p = ns).

{kind=link}
{kind=link}
{kind=link}
Thickness of tunica intima and media in pulmonary arteries from patients with severe chronic obstructive pulmonary disease (COPD) and donors. Data are expressed as the percentage of the area encompassed by the external elastic lamina. Horizontal bars represent medians. ns: nonsignificant. ***: p = 0.001.
No significant differences in morphometric measurements or expression of either TGF-β1 or TGF-βRII were observed between patients with or without α1-antitrypsin deficiency.
The mean intra-observer coefficient of variation for TGF-βRII-positive cells was 0.12, whereas that for TGF-β1-positive cells was 0.08.
Correlations
A significant correlation was found between TGF-βRII expression in the tunica media and the severity of airflow limitation (p<0.05; r = 0.59). No other correlation was found between TGF-βRII expression and any vascular remodelling parameter. Similarly, no correlation was found between vascular remodelling parameters and disease severity or smoking history.
DISCUSSION
The present study shows that, in the pulmonary arteries of patients with very severe COPD undergoing lung transplantation, there is increased expression of TGF-βRII in both the tunica media and tunica intima, which was associated with a normal proliferation index in both layers. Conversely, significant thickening was observed only in the tunica intima, and not in the tunica media, suggesting that mechanisms other than cell proliferation may be involved in intimal thickening.
Since TGF-β1 has been implicated in the pathogenesis of COPD and TGF-βRII in that of pulmonary hypertension 10–17, the focus of the present study was on examining the expression of these two molecules in pulmonary arteries from patients with very severe COPD.
Previous studies have shown an increased number of inflammatory cells 8, 9 in pulmonary arteries from patients with COPD. Inflammatory cells are a source of cytokines and growth factors that may contribute to the development of structural and functional abnormalities of the vessel wall 23. Among different cellular pathways, TGF-β1 is a pleiotropic cytokine that, by binding to its receptors, might be involved in orchestrating both inflammatory and remodelling processes observed in the pulmonary arteries of patients with COPD 24. Although TGF-β1 is often regarded as a purely profibrotic factor 10, considerable evidence indicates that this molecule can exert diverse and potentially protective effects within the vascular wall as it is able to inhibit the proliferation of vascular cells 25. Recent studies in patients with idiopathic pulmonary hypertension have shown defects in growth-suppressive genes, including TGF-βRII and the B-cell-leukaemia/lymphoma-2-gene-product-associated X protein apoptosis-related genes, in plexiform lesions 16. In 90% of plexiform lesions, TGF-βRII is not expressed (in contrast to the abundant expression in the endothelial cells outside the lesions), whereas only 8% of arteries do not express TGF-βRII in secondary pulmonary hypertension. Thus, it has been proposed that somatic mutations in growth regulatory genes allow clonal expansion of endothelial cells, which contribute to the formation of plexiform lesions and vascular obliteration. It is interesting to note that decreased expression of type II receptors with the acquisition of a proliferative phenotype has been described in vascular cells within atheromas 26, 27, and that the loss TGF-βRII has been associated with progression from adenoma to carcinoma 28 and with tumour progression towards metastasis in lung adenocarcinoma 29. Taken together, these studies impute the role of an important growth inhibitor to the TGF-β signalling system, which, if impaired, leads to cells proliferation in cancer and vascular diseases 30. Indeed, loss of TGF-β signalling has recently been described in plexiform lesions of patients with idiopathic pulmonary hypertension 17. The increased expression of the receptor associated with a normal thickness of the tunica media and cell proliferation observed in the present study further suggests an antiproliferative profile for this cytokine, supporting its potential protective role in limiting the vessel wall disease observed in COPD. This might explain the mild pulmonary hypertension in the extremely severe COPD patients examined in the present study. Indeed, the mean pulmonary arterial pressure in the present population was 26 mmHg, which is consistent with that observed by other authors in patients with COPD, in whom it rarely exceeds 35 mmHg 31.
At variance with TGF-βRII expression, expression of TGF-β1 was not significantly different between the two groups of subjects, even if median TGF-β1 expression was higher in severe COPD patients, showing a parallel trend in the expression of the ligand and its type II receptor. This observation, together with the finding of a normal thickness of the tunica media, further supports the antiproliferative role of the TGF-β pathway in COPD. This lack of medial thickening in pulmonary arteries from patients with severe COPD is not completely unexpected, since a similar finding was reported by Santos et al. 6 in patients undergoing lung volume reduction surgery for severe emphysema.
In contrast with the medial layer, increased thickness of the tunica intima was found in patients with severe COPD compared to donors. However, when cell proliferation in the tunica intima was analysed, it was found that it was similar in the two groups of subjects. Based on these findings, it could be hypothesised that different mechanisms, besides cell proliferation, may be involved in intimal thickening, such as extracellular matrix deposition and smooth muscle cell migration. In particular, a latent form of TGF-β, latent TGF-β-binding protein 1, could play a role in intimal remodelling, favouring smooth cell migration, as recently described 32, 33. Furthermore, cytokines other than TGF-β might be involved in the development of intimal remodelling.
Since the TGF-β pathway seems to be involved in the development of not only pulmonary hypertension but also COPD itself, it is intriguing to note that genetic studies point toward a protective role of TGF-β1 in preventing the development of this disease. Indeed, it has recently been reported that the high-producer TGF-β1 genotype may protect against the development of COPD 14, 15, even if the mechanisms through which this molecule acts remain to be elucidated.
In the present study, the structural changes, as well as the expression of TGF-β1 and TGF-βRII, in pulmonary arteries were similar in patients with and without α1-antitrypsin deficiency, indicating that the extent of remodelling of pulmonary arteries is similar in the two types of emphysema. However, it is also possible that the sample size was too small (particularly in the group of patients with α1-antitrypsin deficiency) to detect a significant difference. Furthermore, the fact that all of the patients with α1-antitrypsin deficiency were heavy smokers should be highlighted, and it is possible that smoking itself influenced the results.
Although the poor clinical characterisation of the donors in the present study was clearly apparent, it is possible to be confident that these subjects were free from any kind of major lung diseases, as the lungs were carefully checked by the pathologist for transplantation. Indeed, lung specimens from donors gives the unique opportunity to analyse a large amount of lung tissue in relatively healthy individuals; nonetheless, there are still potential biases. In particular, since smoking history is not an exclusion criterion for selection of lung donors 34, it is possible that some of the donors were smokers. Moreover, some of them would have been ventilated before lung transplantation. Since it is known that smoking and ventilation may induce structural changes in pulmonary arteries, this may have influenced the results 9, 35, 36.
In conclusion, in pulmonary arteries from patients with very severe chronic obstructive pulmonary disease, there is upregulation of transforming growth factor-β family signalling associated with a normal thickness of the tunica media and normal cell proliferation. This may suggest an antiproliferative, and thus protective, role of this cytokine in the development of the pulmonary hypertension observed in end-stage chronic obstructive pulmonary disease. Further studies are required to explore the complexity of the transforming growth factor-β pathway and its involvement in this heterogeneous disease.
Acknowledgments
The authors thank C. Regorda and M.E. Zanin for their help in the collection and analysis of clinical data, and C. Drace Valentini for assistance in editing the manuscript.
- Received July 1, 2005.
- Accepted May 4, 2006.
- © ERS Journals Ltd
References










