





Abstract
Chronic obstructive pulmonary disease (COPD) is associated with increased apoptosis and defective phagocytosis in the airway. As uncleared cells can undergo secondary necrosis and perpetuate inflammation, strategies to improve clearance would have therapeutic significance. There is evidence that the 15-member macrolide antibiotic azithromycin has anti-inflammatory properties. Its effects may be increased in the lung due to its ability to reach high concentrations in alveolar macrophages (AMs).
The present study investigated the effects of low-dose (500 ng·mL-1) azithromycin on the phagocytosis of apoptotic bronchial epithelial cells and neutrophils by AMs. Flow cytometry was applied to measure phagocytosis and receptors involved in AM recognition of apoptotic cells. Cytokines were investigated using cytometric bead array.
Baseline phagocytosis was reduced in COPD subjects compared with controls. Azithromycin significantly improved the phagocytosis of epithelial cells or neutrophils by AMs from COPD subjects by 68 and 38%, respectively, often up to levels comparable with controls.
The increase in phagocytosis was partially inhibited by phosphatidylserine, implicating the phosphatidylserine pathway in the pro-phagocytic effects of azithromycin. Azithromycin had no effect on other recognition molecules (granulocyte-macrophage colony-stimulating factor, CD44, CD31, CD36, CD91, αvβ3 integrin). At higher doses, azithromycin decreased levels of pro-inflammatory cytokines. Thus, low-dose azithromycin therapy could provide an adjunct therapeutic option in chronic obstructive pulmonary disease.
In the normal airway, repair of injury and resolution of inflammation are highly regulated processes. Epithelial injury exposes portions of the basement membrane. A provisional matrix, derived from plasma proteins including fibrin and fibronectin, is rapidly formed. Simultaneously, airway epithelial cells de-differentiate, proliferate and accumulate over the denuded area. Although the cellular mechanisms for removal of excess epithelial cells have not been fully elucidated, the process is likely to involve apoptosis (programmed cell death) of cells not attached to the basement membrane followed by phagocytic removal of apoptotic fragments by neighbouring alveolar macrophages (AMs). This process avoids secondary necrosis and the release of cell contents that may promote further inflammation 1, 2. In addition to their critical role in the phagocytosis of epithelial cells, AMs play an important role in the removal of exogenous particles, such as bacteria, and of excess inflammatory cells including neutrophils.
Previous studies have shown that chronic obstructive pulmonary disease (COPD) is associated with increased apoptosis of bronchial epithelial cells 3. If these cells are not efficiently cleared by adjacent AMs, an accumulation of apoptotic and necrotic material may ensue, promoting the ongoing inflammation and loss of structural integrity that is prevalent in COPD. This may result, at least partially, from an overwhelming of the clearance capacity of AMs, either by excess apoptosis, or by a functional deficiency in the AM. In this regard, the current authors have also reported defective phagocytosis of bronchial epithelial cells by AMs in COPD 4. Building on this evidence, the authors’ current research has focused on treatment strategies that aim specifically at improving macrophage function with a view to improving clearance of apoptotic material in the lung.
A number of studies have suggested that macrolide antibiotics, including azithromycin, have anti-inflammatory properties, partly due to their modulation of production of pro-inflammatory cytokines 5, 6. In addition, a few studies have reported increased macrophage phagocytic activity in the presence of these antibiotics (using neutrophils or beads as targets) 7, 8. However, the effect of macrolide antibiotics on phagocytosis of apoptotic bronchial epithelial cells by AMs, particularly with regard to COPD, has not been studied previously.
The current study investigated the effect of the 15-member macrolide antibiotic azithromycin on the phagocytic ability of AMs obtained from bronchoalveolar lavage (BAL) from human volunteers. It was hypothesised that low-dose azithromycin would improve the phagocytic function of AMs for apoptotic bronchial epithelial cells. Such an approach has the potential to complement existing therapies for COPD significantly.
MATERIALS AND METHODS
Bronchoscopy
AMs were collected from 10 healthy volunteers and nine subjects with COPD (diagnosed using the Global Initiative for Chronic Obstructive Lung Disease criteria 9 of a relevant history and post-bronchodilator forced expiratory volume in one second (FEV1) 30–80% of predicted and FEV1/forced vital capacity <70%), using BAL obtained at fibreoptic bronchoscopy, as previously described 3, 4. Volunteers were specifically recruited for the study and informed consent was obtained. Control subjects were never-smokers with the exception of one currently smoking subject who had normal lung function and no evidence of lung disease. Six COPD subjects were current smokers and three ex-smokers. There was no exacerbation of COPD for 6 weeks prior to involvement in the study. Two of the COPD subjects were receiving inhaled corticosteroids, a further two used bronchodilators as required and the remaining subjects were untreated. Lung cancer was excluded by radiological examination (at least plain postero-anterior and lateral chest radiography) and bronchoscopic examination. Demographic details of the subjects are presented in table 1⇓. Ethics approval was obtained from the Royal Adelaide Hospital (Adelaide, Australia). AMs were washed and resuspended in RPMI 1640 media (Gibco, Karlsruhe, Germany), supplemented with 10% foetal calf serum (Gibco) and 1% weight/volume penicillin/streptomycin (Gibco; hereinafter referred to as “culture medium”), at a concentration of 3×105 cells·mL-1 for investigation of phagocytosis and 3×106 cells·mL-1 for all other investigations.
Demographic characteristics of the population studied
Reagents
Azithromycin was purchased from Pfizer Inc. (New York, NY, USA) and clindamycin from Upjohn Co. (Tokyo, Japan). Ampoules for intravenous use were reconstituted with distilled water to 100 mg·mL-1 and 150 mg·mL-1, respectively, then diluted to the required concentrations with RPMI 1640. The following monoclonal antibodies (MABs) and immunological reagents were employed: CD45 (phycoerythrin (PE)-CY5), CD14 (PE-CY5), CD33 (PE-CY5), CD36 (fluorescein isothiocyanate; FITC), CD51 (FITC; Immunotech/Coulter, Marseille, France), Annexin V (FITC; BD Biosciences, San Jose, CA, USA), 7-amino-actinomycin D (7-AAD; Sigma Chemicals, Castle Hill, Australia), CaspACE FITC-VAD-FMK (Promega, Madison, WI, USA), Mitotracker green (MTG; Molecular Probes, Eugene, OR, USA), CD61 (PE) and CD44 (FITC; BD Biosciences), CD31 (platelet/endothelial cell adhesion molecule-1; PECAM) and CD91 (low-density lipoprotein receptor-related protein; Serotec, Oxford, UK). A MAB to granulocyte-macrophage colony-stimulating factor (GM-CSF) receptor, (MAB)4HI (GM-CSF-R), was provided by A. Lopez (Hanson Institute, Adelaide, Australia). A control immunoglobulin (Ig)G MAB (BD Biosciences) and PE-conjugated rat anti-mouse IgG1 (BD Biosciences) were used with (MAB)4HI. (MAB)217 (IgM kappa chain, a gift from P. Henson, University of Colorado Health Sciences Center, Denver, CO, USA) was also used to identify a surface receptor (expressed on transforming growth factor-β and β-glycan stimulated human monocyte-derived macrophages) that recognises phosphatidyl serine (PS) on apoptotic cells. A control IgM MAB and FITC-conjugated goat anti-mouse IgM (Rockland Immunochemicals, Gilbertsville, PA, USA) were used with the (MAB)217.
Stimulation of AMs
AMs were incubated with different concentrations of azithromycin or the 16-member macrolide antibiotic clindamycin, as a negative control, for 24 h at 37°C in an atmosphere of 5% CO2. GM-CSF was used as a positive control based on reports that it up-regulates phagocytosis in several other models 10, 11. After 24-h incubation, the supernatant was removed and stored at -70°C for further analysis. The pellet containing AMs was resuspended, and surface staining and investigation of apoptosis carried out immediately.
16HBE bronchial epithelial cells
Immortalised normal human bronchial epithelial (HBE) cells (cell line 16HBE) were used as phagocytic targets. The cell line was maintained and passaged as previously described 12. For use in the phagocytosis assay, the cells were induced to apoptosis using ultraviolet (UV) radiation for 20 min, then stained with MTG as previously described 12. It has previously been shown that induction of apoptosis with UV for 20 min achieved >80% apoptosis with minimal necrosis, as assessed by Annexin V/propidium iodide staining, more consistently than other methods including Fas ligation 12.
Neutrophil isolation
Neutrophils were isolated from the peripheral blood of healthy human donors by dextran sedimentation and density-gradient centrifugation. The neutrophil layer was washed in PBS and contaminating erythrocytes lysed with 0.9% buffered ammonium chloride for 5 min. Neutrophils were again washed and resuspended in culture medium at a concentration of 5×106 cells·mL-1, then incubated for 24–48 h at 37°C in 5% CO2 and assessed for apoptosis using Annexin V staining as previously described 13. The percentage of apoptotic neutrophils deemed suitable for use in the phagocytosis assay was ≥60%.
Phagocytosis of apoptotic airway epithelial cells and neutrophils by AMs
A flow-cytometric assay to measure phagocytosis was applied, as previously reported 13, with minor modifications. Briefly, BAL aliquots (1 mL) were added to 10-mL polypropylene tubes (Johns Professional Products, Sydney, Australia), on a 45° slope, and incubated for 2 h at 37°C/5% CO2. The fluid was removed and the adherent AMs were reincubated for 24 h in 1 mL of culture medium containing azithromycin, clindamycin or GM-CSF (a control with medium alone was included). All treatments and controls were performed in triplicate. The fluid was gently removed from the adherent AM monolayer. MTG-stained apoptotic bronchial epithelial cells or neutrophils were washed and then repelleted in 1 mL of culture medium containing the required concentrations of azithromycin or other treatment. These were added to the AMs at a ratio of 10:1. After 1.5-h incubation, the fluid was gently removed, the cells exposed to ice-cold 0.5 mM EDTA, then pelleted by centrifugation without further washing. AMs were then stained with CD33 (PE-Cy5) MAB and washed. Unfixed cells were analysed immediately using a FACS Calibur flow cytometer (BD Biosciences). Crystal violet (0.8 mg·mL-1) was added to quench autofluorescence of AMs and adherent but not phagocytosed epithelial cells. The current authors have previously shown that these assay conditions are optimal for detection of phagocytosis, with an intra-assay coefficient of variation of 10.6%.
Effect of azithromycin on viability of AMs and bronchial epithelial cells
Annexin V staining
Staining with Annexin V was performed for bronchial epithelial cells as previously described 13. Annexin staining could not be used for the investigation of AM apoptosis owing to the known expression of PS from ingested apoptotic cells on the AM cell membrane.
7-AAD staining
Staining with 7-AAD was used to quantify apoptosis as previously described 13.
Staining of apoptotic cells for active caspases
CaspACE FITC-VAD-FMK, an FITC-conjugate of the cell-permeable caspase inhibitor valine-alanine-aspartic acid-fluoromethyl ketone, allows delivery of the inhibitor into the cell where it binds to caspase, serving as a marker for apoptosis. Cells were stained with 100 μl of 10-μM CaspACE, followed by staining with CD14 to identify the macrophage population as previously described 14.
Effect of azithromycin on pro-inflammatory cytokine production by AMs
Interleukin (IL)-12, tumour necrosis factor (TNF)-α, IL-10, IL-6, IL-1β and IL-8 were quantified using an Inflammatory Cytometric Bead Array kit and software (BD Biosciences) as previously reported 15.
Effect of azithromycin on receptors responsible for the phagocytosis of apoptotic bronchial epithelial cells by AMs
The effects of azithromycin on receptors important in the recognition of apoptotic cells by AM were investigated. These included the thrombospondin receptor (TSP-R, CD36), the αvβ3 integrin (CD51/CD61), CD31, CD91 and (MAB)217-reactive PS receptor. A control IgM MAB (100 μg·mL-1) was used as the control for (MAB)217. In concert with the analysis of phagocytic function, expression of these receptors on AMs in the presence of azithromycin was quantified using flow-cytometric methods as previously reported 4. In view of the current authors’ findings and reports by others 16 of the enhancement of phagocytic function by engagement of the CD44 receptor on AMs, the effects of azithromycin on AM expression of CD44 were also investigated.
Effect of azithromycin on GM-CSF receptor expression and GM-CSF production by AMs
In view of the current authors’ findings of increased phagocytosis in the presence of GM-CSF, the effects of azithromycin on GM-CSF levels and GM-CSF receptor expression by AMs were investigated. GM-CSF receptor levels were determined using a MAB to GM-CSF receptor ((MAB)4HI) and flow-cytometric methods as described previously. A control IgG MAB (Dako, Glostrup, Denmark) was included with each analysis. MABS were used at a final concentration of 1 μg·mL-1.
GM-CSF concentrations were measured by specific ELISA (Quantikine; R&D Systems, Minneapolis, MN, USA), using 24-h supernatant from AMs cultured in the presence/absence of 500 ng·mL-1 azithromycin (this concentration was based on the lowest concentration of azithromycin that significantly increased the phagocytic ability of AMs). Triplicate samples from nine individual donors were stored at -70°C and tested on the same day.
Inhibition of phagocytosis by PS liposomes and CD44
AMs (3×106 cells·mL-1 in a total volume of 100 μL) were pre-incubated with each inhibitor at 37oC for 30 min, followed by washing and assay of phagocytosis as described previously. The inhibitors were MABs to CD44 (Serotec) used at a concentration of 10 μg·mL-1, and liposomes prepared by sonication of pure phosphotidylcholine (Avanti Polar Lipids, Pelhan, AL, USA) and PS (Avanti Polar Lipids) in PBS at a molar ratio of 70:30, used at a concentration of 0.1 mM total lipid 17.
Statistical analysis
The nonparametric Mann–Whitney U-test was used to analyse data. A p-value of <0.05 was considered significant.
RESULTS
BAL return
There was significantly reduced BAL return in asymptomatic smokers and COPD subjects (table 1⇑). However, adequate AM numbers to perform the investigations described were obtained from both groups. It should be noted that not all investigations were performed on all subjects.
Effect of macrolide antibiotics on phagocytosis of apoptotic bronchial epithelial cells and neutrophils by AMs
Treatment with 500 ng·mL-1 of azithromycin significantly increased the percentage of AMs that had phagocytosed apoptotic bronchial epithelial cells, compared with untreated AMs (figs 1⇓ and 2⇓). For control subjects, treatment of AMs with 500 ng·mL-1 azithromycin resulted in a mean 55% increase. Similarly, for COPD subjects, there was a mean 67% increase in phagocytosis compared with no-agents-added control. These results were noted for both current and ex-smoker COPD subjects, and for the two COPD subjects who were treated with inhaled corticosteroids.

Representative histograms showing the effects of azithromycin on the phagocytosis of apoptotic bronchial epithelial cells and neutrophils by alveolar macrophages (AM; derived from normal volunteers). AMs were incubated with 500 ng·mL-1 azithromycin for 24 h prior to phagocytosis assay. The percentage of AMs that had ingested fluorescein isothiocyanate-stained apoptotic cells after 90 min co-incubation was assessed by flow cytometry. Histograms show relative fluorescence intensities of Mitotracker green staining of a) AM plus ingested apoptotic bronchial epithelial cells, and b) AM plus ingested apoptotic neutrophils. There is relatively lower phagocytosis of apoptotic neutrophils compared with apoptotic epithelial cells. The peaks to the left represent AMs that have not ingested cells; the peaks to the right represent AMs that have ingested cells. ░: untreated cells; –––: azithromycin-treated cells.

Effect of azithromycin (500 ng·mL-1) on the phagocytosis of apoptotic a) bronchial epithelial cells, and b) neutrophils by alveolar macrophages (AMs). AMs from normal volunteers or subjects with chronic obstructive pulmonary disease (COPD) were incubated with (Az+)/without (Az-) 500 ng·mL-1 azithromycin for 24 h prior to phagocytosis assay. Each value represents the mean of triplicate determinations. *: p<0.05 versus control with no azithromycin added.
Consistent with the results obtained using apoptotic airway epithelial cells, there was a significant increase (mean increase 38 and 70% in control and COPD groups, respectively) in phagocytosis of apoptotic neutrophils in the presence of 500 ng·mL-1 azithromycin (figs 1⇑ and 2⇑).
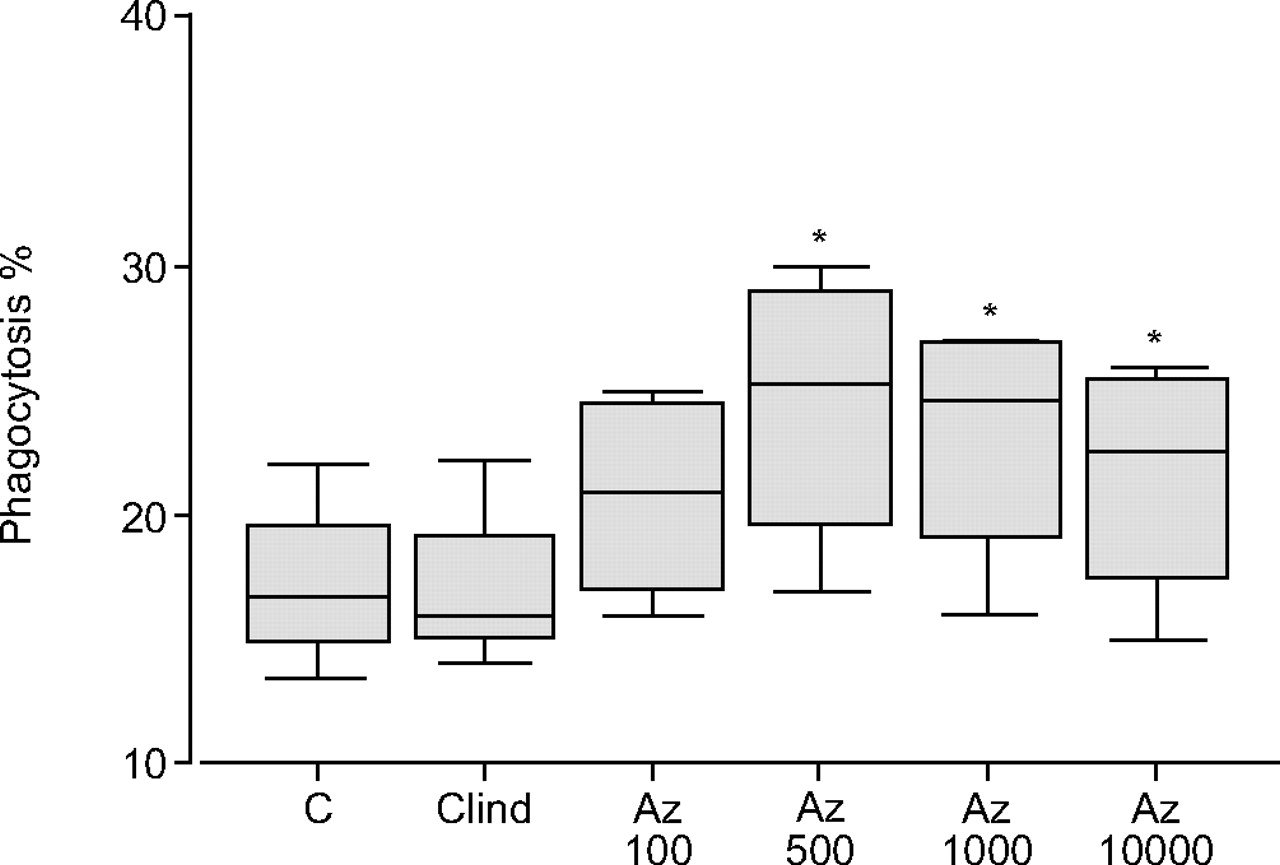
There was no significant increase in phagocytosis with increasing doses of azithromycin beyond 500 ng·mL-1 (fig. 3⇓). Similar enhancing effects were noted in the presence of 500 IU·mL-1 GM-CSF, a positive control (for control subjects, treatment of AMs with GM-CSF resulted in a 65% increase in phagocytosis of bronchial epithelial cells compared with no-agents-added control). In contrast, a 16-member macrolide, clindamycin, failed to improve the phagocytic ability of AMs significantly and was thereafter used as a negative control (fig. 3⇓).

Effects of clindamycin (Clind) and varying concentrations of azithromycin (Az; 0–10,000 ng·mL-1) on the phagocytosis of apoptotic bronchial epithelial cells by alveolar macrophages (AMs). AMs from normal volunteers were incubated with azithromycin for 24 h prior to phagocytosis assay. Box plots show mean±sd and data range of three separate experiments. *: p<0.05 versus control (C) with no antibiotic added.
The effects of azithromycin were dependent on the length of time the AMs were pre-incubated with the antibiotic (fig. 4⇓). Pre-incubation of airway epithelial cells or neutrophils with azithromycin did not improve their phagocytosis by AMs (data not shown).

Time-dependent effects of pre-incubation of alveolar macrophages (AMs) with 500 ng·mL-1 azithromycin on the phagocytosis of apoptotic bronchial epithelial cells by AMs. AMs from normal volunteers were incubated with azithromycin for 0–36 h prior to phagocytosis assay. Box plots show mean±sd and data range of three separate experiments. *: p<0.05 versus control (C) with no azithromycin added.
Baseline phagocytic ability of macrophages from COPD subjects versus controls
The phagocytic capacity of the macrophages from COPD subjects was lower than that seen with the normal controls (p = 0.005), providing confirmation of previous results 13, on this occasion in a cohort of subjects in whom malignancy had been excluded (fig. 2⇑).
Effect of azithromycin on viability of AMs and bronchial epithelial cells
7-AAD staining and measurement of caspase activation revealed no significant effects on AM viability of 500 ng·mL-1 azithromycin for up to 48 h, compared with control treatment (data not shown). Similarly, treatment with azithromycin for up to 48 h did not adversely effect the viability of 16HBE bronchial epithelial cells compared with control treatment where no azithromycin was added (e.g. 500 ng·mL-1 azithromycin for 24 h. Annexin: control 21.5±5.7% versus azithromycin 25.8±9.1%; 7-AAD: control 24.5±5.7% versus azithromycin 24.6±7.9%; Caspase: control 25.3±4.5% versus azithromycin 23.4±5.1%).
Effect of azithromycin on AM phenotype and receptors responsible for the phagocytosis of apoptotic bronchial epithelial cells by AMs
There was no change in CD14 staining on AMs in the presence of azithromycin (data not shown). The αvβ3 integrin/TSP-R/TSP system is one pathway by which AMs recognise apoptotic cells 18. Levels of these receptors on AMs were measured to investigate their involvement in the effects of azithromycin on phagocytosis. No significant differences in expression of TSP-R (CD36) or αvβ3 integrin were noted in the presence of 500 ng·mL-1 azithromycin (fig. 5⇓). The expression of CD51 and CD61 was low on AMs and not increased in the presence of azithromycin. Similarly, there was no change in the expression of (MAB)217-reactive receptor, which recognises PS on apoptotic cells, after treatment of AM with azithromycin (fig. 5⇓). CD31 and CD91, two further receptors on AMs that are involved in the recognition of apoptotic cells, were also investigated. No significant differences in the expression of CD31 or CD91 were noted in the presence of 500 ng·mL-1 azithromycin (fig. 5⇓).

Detection of phagocytic recognition molecules on alveolar macrophages (AMs). AMs were incubated for 24 h in the presence (▓)/absence (▒) of 500 ng·mL-1 azithromycin, and flow cytometry was used to measure surface staining. AMs were gated as CD33 (PE-Cy5) bright. Histograms show relative fluorescence intensities of surface staining for a) CD44, b) CD91, c) monoclonal antibody 217-reactive phosphatidylserine receptor, d) CD36, and e) CD31. There were no significant changes in the presence of 500ng·mL-1 azithromycin. ░: isotype control.
Effect of azithromycin on GM-CSF receptor expression and GM-CSF production by AMs
The expression of GM-CSF receptor on AMs was low (<10% of cells) and not significantly increased in the presence of 500 ng·mL-1 azithromycin for 24 h.
There was no significant increase in GM-CSF production by AMs after 24 h in the presence of 500 ng·mL-1 azithromycin (no azithromycin 6.8±9.2 pg·mL-1 versus 500 ng·mL-1 azithromycin 7.0±10.8pg·mL-1). For all receptors, similar results were observed in the presence of 1,000 or 5,000 ng·mL-1 azithromycin (data not shown).
Inhibition of phagocytosis by PS liposomes and CD44
Azithromycin and CD44 ligation had similar phagocytosis-enhancing effects (fig. 6⇓). There was no additional increase in phagocytosis when the two were combined.

Effect of inhibitors on the phagocytosis of apoptotic bronchial epithelial cells by alveolar macrophages (AMs). AMs from normal volunteers were incubated with each inhibitor for 30 min, washed then exposed to apoptotic bronchial epithelial cells for 90 min. a) phosphatidylserine (PS) liposomes; b) CD44 (10 μg·mL-1). C: media only; Az: azithromycin 500 ng·mL-1; PS block: 0.1 mM PS liposomes. Box plots show mean±sd and data range of three separate experiments. *: p<0.05 versus control with no inhibitor or Az added. There is an increase in the phagocytic ability of AMs with CD44 ligation or Az but no additive effect with both mediators. There is a decrease in the pro-phagocytic effect of azithromycin after treatment with PS liposomes.
PS liposomes suppressed azithromycin-enhanced phagocytosis (fig. 6⇑), indicating that the PS pathway may be at least partially involved in the azithromycin-mediated phagocytosis of apoptotic bronchial epithelial cells by AMs.
Effect of azithromycin on pro-inflammatory cytokine production by AMs
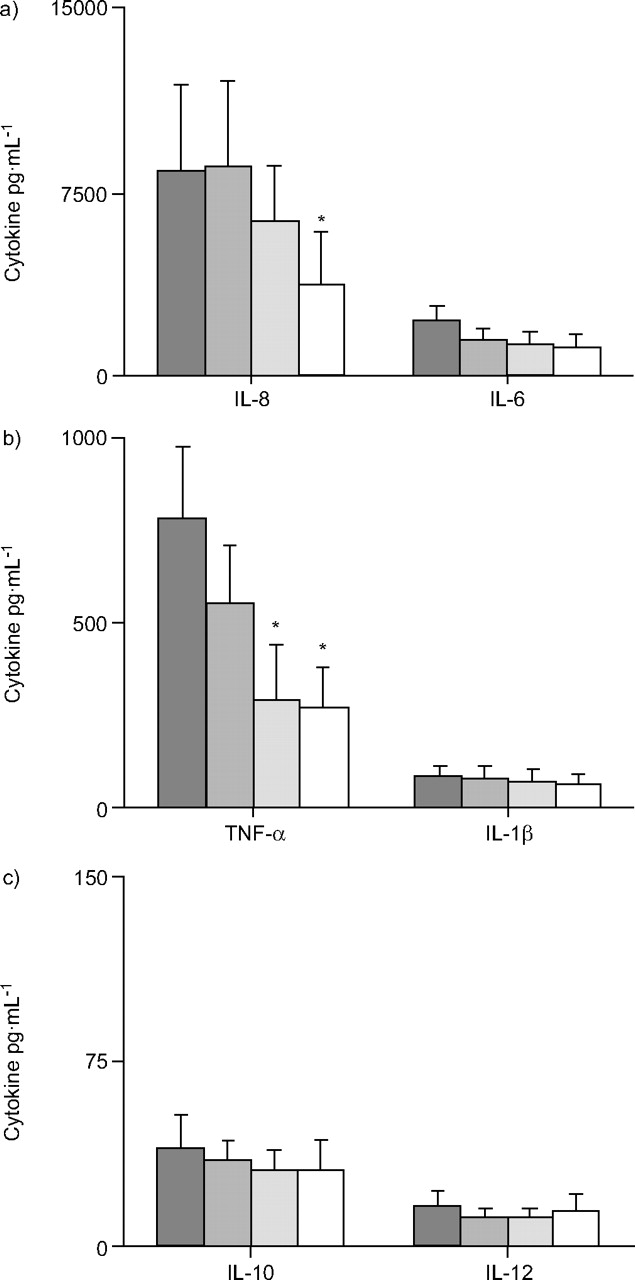
Cytokine levels were measured by cytometric bead array after 24-h incubation of AMs in the presence of azithromycin. With 500 ng·mL-1 azithromycin, there was a trend for decreased expression of IL-6 and significantly reduced expression of TNF-α and IL-8 (fig. 7⇓). However, the decrease reached statistical significance only when concentrations of azithromycin were increased to 1,000 ng·mL-1 for TNF-α and 10,000 ng·mL-1 for IL-8 (fig. 7⇓).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effect of azithromycin on pro-inflammatory cytokine production by alveolar macrophages (AMs). Azithromycin (500–10,000 ng·mL-1) was added to AMs for 24 h. Cytokine levels in culture supernatant were measured by cytometric bead array. There is a significant decrease in tumour necrosis factor (TNF)-α in the presence of 1,000 and 10,000 ng·mL-1 azithromycin and interleukin (IL)-8 in the presence of 10,000 ng·mL-1 azithromycin. Data are presented as mean±sem of five separate experiments, in triplicate. ▒: control (no azithromycin); ▓: 500 ng·mL-1 azithromycin; ░: 1,000 ng·mL-1 azithromycin; □: 10,000 ng·mL-1 azithromycin. *: p≤0.05 versus control.
DISCUSSION
The current authors report that the macrolide antibiotic azithromycin at low doses significantly improved the phagocytosis of apoptotic bronchial epithelial cells by BAL-derived AMs from normal and COPD subjects, without having pro-apoptotic effects on either AMs or epithelial cells. No changes were noted in the presence of a 16-member macrolide, clindamycin. In agreement with other studies 7, 8, similar effects were also noted for clearance of apoptotic neutrophils. These results were noted for both current and ex-smoker COPD subjects, and for the two COPD subjects who were treated with inhaled corticosteroids, suggesting that the pro-phagocytic effects of azithromycin are not adversely influenced by smoking per se, or by drug effects. Whether the effects of azithromycin are reduced in patients with advancing age remains to be determined. The present study investigated subjects with mean ages of 53 and 60 yrs for controls and COPD groups, respectively. Although the effects of ageing upon human AMs have not been determined, a study of rodent macrophages reported age-related changes in macrophage function 19.
Improving the phagocytic ability of AMs for bronchial epithelial cells may have clinical significance with regard to new or adjunct treatments for COPD where there is inflammation associated with ineffective repair of the injured epithelium and loss of structural integrity. This inflammatory condition is associated with increased apoptosis of bronchial and alveolar epithelial cells 3. In addition to an absolute increase in pro-apoptotic mechanisms, the current authors have previously shown that impaired capacity for phagocytic clearance of apoptotic bronchial epithelial cells is likely to be important in COPD 12. There is already compelling experimental evidence that macrophages play a key role in the resolution of inflammatory responses. For instance, the causative link between macrophage dysfunction and consequent accumulation of secondary necrotic material was demonstrated in a study by Knapp et al. 2, in which mice selectively depleted of AMs showed impaired resolution of inflammation and increased mortality, directly related to increased accumulation of apoptotic material and secondary necrosis.
The current findings of improved AM phagocytic ability for apoptotic bronchial epithelial cells in the presence of azithromycin may thus provide a novel approach to supplement existing therapies in COPD. To date, pharmacological therapies for COPD have focused on smooth-muscle function (bronchodilators) and efforts to dampen inflammatory responses (corticosteroids). Refinements in these approaches have yielded some therapeutic gains but, in many patients, responses are still often unsatisfactory. It has also become clear that many of the cellular abnormalities in COPD, including excess epithelial apoptosis, persist despite smoking cessation 3. Thus, novel approaches to treatment are critical if management of this disease is to improve. Therapies that improve clearance of accumulated apoptotic material may reduce the risk of secondary necrosis and release of toxic cell contents that perpetuate inflammation.
The pharmokinetics of azithromycin are characterised by rapid uptake by AMs with high, sustained levels in tissues 20, 21. The effects of azithromycin may be even more marked in COPD subjects who continue to smoke as smokers have increased intrapulmonary uptake of antibiotics that are highly concentrated in AMs 22, 23. Importantly, there have been many reports of the anti-inflammatory properties of azithromycin 24, 25. As a result, low-dose azithromycin has already been used for clinical trials in various disease states, including cystic fibrosis 26, panbronchiolitis 27 and bronchiolitis obliterans 22. In addition, an in vivo study of human volunteers treated with 500 mg·day-1 azithromycin for 3 days demonstrated an increase in neutrophil apoptosis up to 28 days after the last azithromycin dose, and a continuous fall in chemokine and IL-6 concentrations in serum 28. This finding has particular relevance to COPD where prolonged neutrophil survival has been linked to the pathogenesis of the disease 29.
The current findings suggest that the effects of azithromycin may be mediated by improved phagocytic ability of AMs for apoptotic bronchial epithelial cells, in addition to other anti-inflammatory properties of the antibiotic. The findings are consistent with those of Yamaryo et al. 7, who reported that azithromycin promoted the phagocytosis of apoptotic neutrophils by AMs. The mechanisms leading to the improvement of AM phagocytosis in the presence of low-dose azithromycin are unclear. Consistent with other studies 30, the current authors noted a significant decrease in TNF-α and IL-8 in the presence of azithromycin. However, these effects required higher concentrations of azithromycin (>1,000 ng·mL-1) than the maximum effect on phagocytosis (500 ng·mL-1), suggesting that the pro-phagocytic effects of low-dose azithromycin may involve pathways other than those related to the inflammatory cytokine/chemokine network.
Ligation of CD44 receptors was shown to increase the phagocytic ability of AMs by a similar magnitude to azithromycin. However, the effects of azithromycin and CD44 ligation on phagocytosis were not additive. While the latter finding may implicate the CD44 pathway in the pro-phagocytic effects of azithromycin, it is also possible that the maximum phagocytic capacity of the AMs had been reached, masking the additive effect that would have been noted if azithromycin was working via a separate pathway to CD44. Additionally, no change in AM surface expression of CD44 in response to azithromycin was found.
Several receptors important for the recognition and removal of apoptotic cells by AMs were studied. These include the vitronectin receptor (αvβ3 integrin), TSP-R (CD36), CD31 (PECAM), CD91 and a (MAB)217-reactive PS receptor 31, 32. In the present study, however, no changes were noted in any of these receptors in the presence of azithromycin. Yamaryo et al. 7 similarly found that blocking AMs with (MAB)217 did not alter the levels of phagocytosis of apoptotic neutrophils by AMs. The present study found, however, that PS liposomes inhibited the azithromycin-enhanced phagocytosis of apoptotic bronchial epithelial cells by AMs, indicating that the pro-phagocytic ability of azithromycin is at least partially PS dependent. These findings are also consistent with a report of PS receptor-dependent up-regulated phagocytosis of apoptotic neutrophils in the presence of erythromycin and clarythromycin 7.
Yamasawa et al. 33 recently investigated the effects of azithromycin on TNF-α-stimulated A549 airway epithelial cells and reported that the mechanism of action of azithromycin may, at least partially, relate to the modulation of GM-CSF release. However, the increase in GM-CSF only occurred in the presence of azithromycin at concentrations >10,000 ng·mL-1. The current authors used azithromycin at concentrations that are clinically achievable with low-dose treatment regimes 34 and found no significant changes in GM-CSF release or expression of GM-CSF receptor after treatment of AMs with azithromycin, suggesting that the GM-CSF pathway may not be involved in the effects of low-dose azithromycin on AM function.
Although commonly used for treatment of acute exacerbations, there are little data on the use of low-dose long-term azithromycin therapy for COPD, although another macrolide antibiotic, clarithromycin (at 500 mg·day-1 for 3 months), has been applied for the treatment of patients with moderate-to-severe COPD 35, causing a small reduction in the neutrophil differential and neutrophil chemotaxis. Whether low-dose long-term azithromycin treatment will result in a significant improvement in COPD requires further study. Interestingly, the present study showed that the phagocytosis-promoting effects of azithromycin reached their maximum at the low dose of 500 ng·mL-1, suggesting that the low doses used in cystic fibrosis trials would be appropriate for improving the phagocytic ability of AMs in COPD.
The current authors have thus established the efficacy of azithromycin for improving macrophage function in normal and chronic obstructive pulmonary disease subjects. This work indicates a rationale for further clinical studies of azithromycin in chronic obstructive pulmonary disease.
Acknowledgments
The authors acknowledge the invaluable contribution of the Bronchoscopy Unit and the nursing staff at the Chest Clinic of the Thoracic Medicine Dept, Royal Adelaide Hospital, Adelaide, Australia.
- Received January 4, 2006.
- Accepted May 15, 2006.
- © ERS Journals Ltd
References










