





Abstract
The aim of the present study was to assess the feasibility of measuring combined arterial oxygen saturation measured by pulse oximetry (Sp,O2) and cutaneous carbon dioxide tension (Pc,CO2) to monitor ventilation and quantify change in Pc,CO2 during bronchoscopy.
Combined Sp,O2 and Pc,CO2 were measured at the ear lobe in 114 patients. In four patients, the ear-clip slipped and they were excluded. In total, 11 patients had artefacts with Sp,O2 recordings, thus, Sp,O2 was analysed in 99 patients. Spirometry data were available in 77 patients. Multivariate analysis of covariance and logistic regression were used for statistical analyses.
Mean baseline Pc,CO2 was 4.78±1.06 kPa (36±8 mmHg) and mean rise in the Pc,CO2 during bronchoscopy was 1.26±0.70 kPa (9.5±5.3 mmHg), while mean Pc,CO2 at the end of bronchoscopy was 5.85±1.19 kPa (44±9 mmHg) . Baseline Pc,CO2 and the lowest Sp,O2 were significantly associated with peak Pc,CO2 and the change in Pc,CO2 during bronchoscopy. Risk of significant hypoxaemia (Sp,O2≤90%) was lower for a higher baseline Sp,O2. Peak Pc,CO2 was directly associated with significant hypoxaemia. There was no significant association in the baseline Pc,CO2, peak Pc,CO2, baseline Sp,O2 or the lowest Sp,O2 comparing patients with and without chronic obstructive pulmonary disease.
In conclusion, it is feasible to measure combined pulse oximetry and cutaneous carbon dioxide tension effectively to monitor ventilation during flexible bronchoscopy.
Flexible bronchoscopy under local anaesthesia and sedation is widely performed to diagnose and manage a variety of lung diseases. The purpose of sedation is to facilitate examination of the tracheobronchial tree, carry out the necessary diagnostic or interventional procedures, and provide patient comfort 1–4. Oximetry measures the oxygenation of blood and can detect hypoxaemia, but it cannot detect hypercarbia and hence the adequacy of ventilation 5. When bronchoscopy is performed under conscious sedation without supplemental oxygen, oxygen desaturation will occur rapidly giving a good indication of ventilatory status. It has recently been shown that pulse oximetry is a useful tool to assess ventilatory abnormalities, but only in the absence of supplemental inspired oxygen 6. However, most centres routinely offer oxygen supplementation to patients during flexible bronchoscopy 7. Due to the S-shaped curve of the oxygen dissociation curve, in such situations the alveolar carbon dioxide tension will have to increase further before significant hypoxaemia is manifested 8. The British Thoracic Society (BTS) guidelines recommend that oxygen supplementation should be used to achieve an oxygen saturation (Sp,O2) of at least 90% to reduce the risk of significant arrhythmias during the procedure and also in the post-operative recovery period 2. Furthermore, they suggest that care should be taken to be alert to signs of respiratory failure in patients on oxygen supplementation, who may have “safe” oximetry readings, but who may be developing carbon dioxide retention 2. Therefore, a reliable substitute of carbon dioxide arterial tension (Pa,CO2) measured noninvasively is required as it might enhance patient safety during flexible bronchoscopy.
In intubated patients or patients under stable conditions without oral leakage, end-tidal carbon dioxide tension has a good correlation with Pa,CO2 9, 10. However, during endoscopy procedures under sedation, regular breathing is often disturbed by moving, coughing or changes between nose and mouth ventilation, causing leakage and artefacts or misinterpretation of the data acquired with end-tidal carbon dioxide measurements. These problems often restrict the use of side-stream capnography in clinical practice 10. Measurement of cutaneous carbon dioxide tension (Pc,CO2) with a digital sensor has recently been reported 11. The Pc,CO2values have been shown to have a good correlation with arterial blood gas measurements 12, 13. A rise in Pc,CO2measurement has been reported during medical thoracoscopy and colonoscopies 10, 13. The present authors aimed to assess the feasibility of measuring combined pulse oximetry (Sp,O2) and Pc,CO2at the ear lobe to monitor ventilation and quantify the degree of change in Pc,CO2during flexible bronchoscopy under local anaesthesia and sedation.
PATIENTS AND METHODS
Combined oximetry and Pc,CO2 were prospectively measured in 114 patients undergoing flexible bronchoscopy in an observational fashion (monitoring system from Sentec AG, Therwil, Switzerland). The combined cutaneous digital sensor was placed on the ear lobe of all patients prior to the procedure and was removed when the patient left the bronchoscopy suite.
Flexible bronchoscopy was performed under local anaesthesia and sedation. Combined sedation was achieved with intermittent boluses of intravenous midazolam and 5 mg of hydrocodone 1. All patients received supplemental nasal oxygen at 2–4 L·min-1. Significant hypoxaemia (Sp,O2≤90%) during flexible bronchoscopy was successfully treated with jaw support or nasopharyngeal tube insertion 7. The duration of bronchoscopy was calculated from the administration of sedation until the flexible bronchoscope was removed from the tracheobronchial tree. Bronchoalveolar lavage (BAL) was performed in 57 patients, endobronchial biopsy in 32, bronchial washings in 19, transbronchial needle aspiration in 18, transbronchial biopsy in 15 patients and bronchial brushings in 11 patients. Spirometry data prior to bronchoscopy was available in 77 patients. Patients with chronic obstructive pulmonary disease (COPD) were defined using the American Thoracic Society/European Respiratory Society guidelines 14.
Statistical analysis
Data are presented as mean±sd. Multivariate analysis was performed using analysis of covariance to examine peak Pc,CO2, change in Pc,CO2 from baseline, and change in Pc,CO2 adjusted for baseline Pc,CO2 during bronchoscopy as dependent factors versus patient age, dose of midazolam (mg·kg-1), baseline Pc,CO2 and lowest Sp,O2as independent factors. Scatterplots are provided for the association of peak Pc,CO2 and change in Pc,CO2 with duration of procedure. ANOVA was used to examine the association between the type of sampling procedure during bronchoscopy with the change in Pc,CO2. Logistic regression was used to examine independent factors associated with significant hypoxaemia (Sp,O2≤90%) and COPD. The t-test was used to compare significance between the baseline and peak Pc,CO2 during bronchoscopy and Pc,CO2 at lowest Sp,O2 and the peak Pc,CO2 during bronchoscopy.
RESULTS
The mean duration of the procedure was 19±10 min. In four patients, the ear-clip slipped off the ear lobe due to patient movement. These patients were not included in the analysis as the equilibration had to be achieved again and there was loss of data recording points. Therefore data analysis was performed in 110 patients (70 males and 40 females, mean age 61±15 yrs). In 11 patients, the Sp,O2 was not included in the analysis due to artefacts produced by coughing or a low signal whilst recording. Therefore, Pc,CO2 measurements, for the purposes of data analysis, were available in 110 patients and both oximetry and Pc,CO2 measurements were available in 99 patients. Therefore, for multivariate analysis only data from patients with both oximetry and Pc,CO2 were used. Hypoxaemia during the procedure was successfully treated with jaw support or nasopharyngeal tube insertion in all patients. None of the patients developed severe respiratory depression resulting in administration of sedation reversal medication or in abandoning the procedure without completion. The indications for bronchoscopy were: 1) suspected lung malignancy, 42 (38%) patients; 2) radiological infiltrates, 31 (28%) patients; 3) haemoptysis, nine (8%) patients; 4) suspected interstitial lung disease, nine (8%) patients; 5) suspected sarcoidosis, five (5%) patients; 6) post-airway stent inspection, four (4%) patients; 7) cough, three (3%) patients; 8) post-lung surgery, two (2%) patients; and 9) evaluation of post-tracheostomy tracheal stenosis, larngeal papilloma and mucociliary dyskinesis (all n = 1).
The mean dose of midazolam administered was 0.06±0.03 mg·kg-1. The mean baseline Pc,CO2 was 4.78±1.06 kPa (36±8 mmHg) and the mean peak Pc,CO2 was 6.11±1.19 kPa (46±9 mmHg; p<0.0001). The peak Pc,CO2 during the procedure was recorded at a mean duration of 13±7 min. The mean rise in the Pc,CO2 during the procedure was 1.26±0.70 kPa (9.5±5.3 mmHg). The mean Pc,CO2 at the end of the procedure was 5.85±1.19 kPa (44±9 mmHg) and at the time of removal of the sensor was 5.85±1.19 kPa (44±9 mmHg). A rise in Pc,CO2 was observed in all patients except one. The baseline Sp,O2 was 97±2%. The lowest mean Sp,O2 was 93±4%. The lowest Sp,O2 in patients who desaturated from their baseline Sp,O2 measurement was recorded at a mean duration of 9±6 min. The mean Pc,CO2 measured at lowest Sp,O2 was 5.85±1.86 kPa (44±14 mmHg) and the mean peak Pc,CO2 recorded subsequently was 6.78±1.72 kPa (51±13 mmHg; p<0.0001).
Factors associated with peak Pc,CO2and change in Pc,CO2during the study
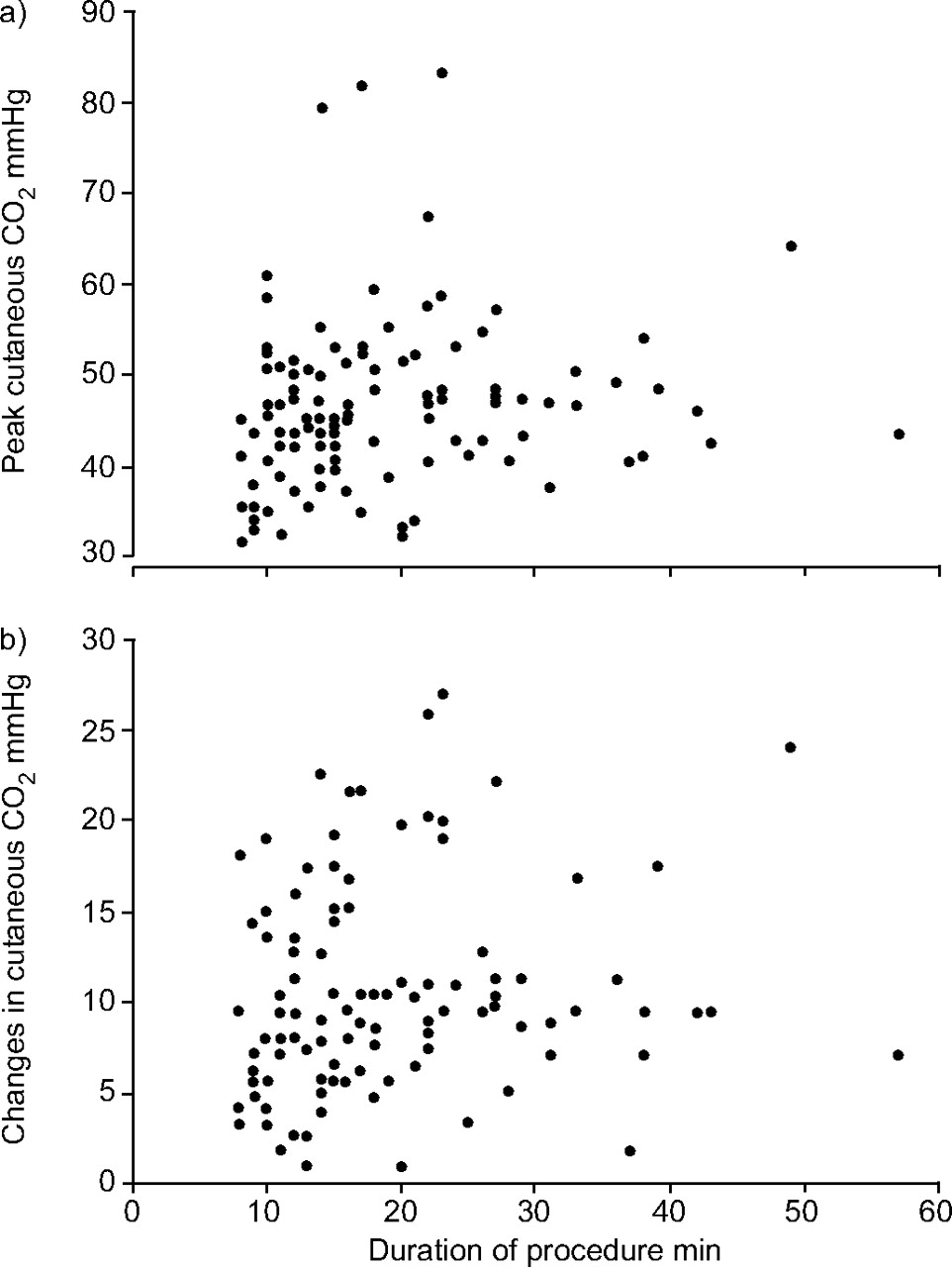
The peak Pc,CO2 during the study was significantly associated with the baseline Pc,CO2 (p<0.0001) and lowest Sp,O2 (p = 0.016). A higher baseline Pc,CO2 was associated with the peak Pc,CO2 (β = 0.8). However, there was an inverse relationship of the lowest Sp,O2 with the peak Pc,CO2, thus, the manifestation of a lower Sp,O2 was associated with the peak Pc,CO2 (β = -0.4). Change in Pc,CO2 (difference in baseline and peak Pc,CO2) was also significantly associated with baseline Pc,CO2 (p = 0.024) and lowest Sp,O2 (p = 0.016). Both of these factors had an inverse relationship with the change in Pc,CO2, thus, patients manifesting a lower Sp,O2 (β = -0.4) and a lower baseline Pc,CO2 (β = -0.2) would have a higher change in Pc,CO2. Similarly, the change in Pc,CO2 divided by the baseline Pc,CO2 (adjusting the change in Pc,CO2 for baseline) was also significantly associated with baseline Pc,CO2 (p<0.0001) and lowest SO2 (p = 0.016). This analysis highlights that baseline Pc,CO2 and the lowest Sp,O2 are linked to the peak Pc,CO2 as well as the rise in Pc,CO2 during bronchoscopy. There was no significant relationship of age and midazolam dosage with the peak Pc,CO2, change in Pc,CO2 and the change in Pc,CO2/baseline Pc,CO2. There was also no association of peak Pc,CO2 and change in Pc,CO2 with the procedure duration (fig. 1⇓). This factor was not included in the multivariate analysis as there appear to be two groups of patients; one group with higher peak Pc,CO2 and change in Pc,CO2 with a short duration of procedure and the other group of patients who have a higher peak and change in Pc,CO2 with a longer duration of procedure. To assess the influence of procedure on change in Pc,CO2 and change in Pc,CO2/baseline Pc,CO2, these were categorised as follows: 1) transbronchial biopsy only and transbronchial needle aspiration only (n = 10); 2) BAL only (n = 42); 3) transbronchial biopsy, transbronchial needle aspiration, and BAL in a combination of two or more (n = 16); and 4) bronchial washings and/or endobronchial biopsy (n = 42). There was no significant association between the procedures performed and change in Pc,CO2 (p = 0.3) and change in Pc,CO2/baseline Pc,CO2 (p = 0.2) during bronchoscopy.
{kind=link}
Scatter plot of duration of procedure in a) peak cutaneous carbon dioxide and b) change in cutaneous carbon dioxide.
Factors associated with significant hypoxaemia and COPD
In total, 15 patients had significant hypoxaemia during bronchoscopy. A lower baseline Sp,O2 (p = 0.003; odds ratio (OR) 0.6) and the peak Pc,CO2 (p = 0.041; OR 1.1) were significantly associated with significant hypoxaemia. Therefore, with a higher baseline Sp,O2 the risk of significant hypoxaemia is lower and the peak Pc,CO2 is directly associated with significant hypoxaemia. Patient age, duration of procedure, midazolam dose and baseline Pc,CO2 were not associated with significant hypoxaemia. In total there were 25 patients with COPD. The mean forced expiratory volume in one second in patients with mild, moderate, severe and very severe COPD was 90±10% (n = 4), 64±8% (n = 13), 39±5% (n = 6) and 25±3% (n = 2), respectively. There was no significant association in the baseline Pc,CO2, peak Pc,CO2, baseline Sp,O2, or the lowest Sp,O2 comparing patients with and without COPD.
DISCUSSION
Recently, Pc,CO2 measurements obtained using the device used in this study have been shown to have a good correlation with arterial carbon dioxide values when >100 samples were compared (R = 0.95) 13. The findings of the present study show that ventilation can be effectively monitored during flexible bronchoscopy using combined oximetry and Pc,CO2measurement. In a study of 22 patients, an increase in Pc,CO2 has been shown to occur during flexible bronchoscopy 5. However, Evans et al. 5 concluded that the technology they used for Pc,CO2 monitoring was complex. Measurement of Pc,CO2 in the current study was simple and did not lead to a delay in the start of the procedure or any complications related to the equipment. The potential complication when using this device is burning of the skin as the sensor is heated to a temperature of 42°C. The recommended maximum duration for which a sensor can be placed cutaneously at 42°C is 8 h 15. None of the patients in the present study had an apparent burn on the skin. The BTS guidelines caution physicians to monitor signs of respiratory failure in patients undergoing flexible bronchoscopy on oxygen supplementation that may have safe oximetry readings, but may be developing carbon dioxide retention. Patients with a higher baseline Pc,CO2 are at a greater risk of developing a higher peak Pc,CO2. Furthermore, the peak Pc,CO2 was significantly associated with the lowest Sp,O2 during bronchoscopy. The results of the current study show that it is feasible to measure continuous Pc,CO2during bronchoscopy, which has been shown to be a good surrogate of Pa,CO2 2, 12, 13. Based on the findings of the present study, no specific trend was observed in the association between peak Pc,CO2 and change in Pc,CO2 with procedure duration, both a short and a longer procedure duration were associated with the peak Pc,CO2 and change in Pc,CO2. The ability to effectively measure Pc,CO2 is an important step in patient monitoring as diagnostic bronchoscopies are performed using routine sedation and also drugs, such as propofol, which are considered as general anaesthetics are being increasingly used also in the absence of a trained anaesthetist 16–19.
The mean duration to the manifestation of lowest Sp,O2 was earlier than the mean duration to the peak Pc,CO2. Therefore, it seems impossible to predict the occurrence of lowest Sp,O2 based on rising Pc,CO2 values. The lowest Sp,O2 manifested was significantly associated with peak Pc,CO2. The hypothesis for this observation is that hypoventilation during flexible bronchoscopy performed under sedation with oxygen supplementation is multifactorial, and not only due to central respiratory depression, in which case a rise in Pc,CO2 would precede significant hypoxaemia due to the nature of the oxygen dissociation curve. Hypoventilation during flexible bronchoscopy is therefore due to a combination of upper airway obstruction, alveolar hypoventilation caused by sedative medication and the procedure itself 7. The effective treatment of hypoxaemia with jaw support or nasopharyngeal tube insertion supports the role of upper airway obstruction leading to acute hypoxaemia during flexible bronchoscopy 7. The rise in Pc,CO2 manifested thereafter reflects alveolar hypoventilation, which is likely to be due to the combined effect of sedatives (central respiratory depression), as well as the procedure itself potentially leading to ventilation perfusion mismatch. The findings of the current study show that after effective treatment of upper airway obstruction, there continues to be a rise in Pc,CO2 reflecting hypoventilation. Therefore, Sp,O2 alone is not sufficient to monitor the complete ventilation status of the patient during bronchoscopy, thus highlighting the value of combined oximetry and cutaneous capnography during bronchoscopy.
The permissible level of Pc,CO2 rise during bronchoscopy is not known. The BTS guidelines state that the use of sedation in patients with severe COPD has increased risks relating to potential carbon dioxide retention 2. The findings of the present study show that patients with COPD who are not in hypercapnic respiratory failure are at an equal risk of hypercapnia as well as hypoxaemia compared with patients without COPD. Based on the findings of the current study (mean rise in Pc,CO2 of 1.33±0.66 kPa), the present authors speculate that a rise of 2.0 kPa in Pc,CO2 from baseline may be an indication to limit further administration of sedatives and needs to be confirmed in future studies.
In conclusion, the current study demonstrates the feasibility of measuring combined oximetry and cutaneous capnography effectively to monitor ventilation during flexible bronchoscopy. Patients with COPD who are not in hypercapnic respiratory failure have a similar risk of hypoxaemia and hypercapnia compared with those without COPD during bronchoscopy. The peak Pc,CO2 is higher in patients with a higher baseline Pc,CO2 and is associated with lowest Sp,O2 during bronchoscopy. Significant hypoxaemia is associated with the peak Pc,CO2 and baseline Sp,O2. With the current study results, it is not possible to predict and accurately select a group of patients who should undergo capnography during bronchoscopy. Patients with elevated baseline Pa,CO2 or a low baseline Sp,O2 will have the benefit of better monitoring of ventilation using such a device. Specifically, patients with a longer duration of procedure did not show a different rise in Pc,CO2 compared with the others. Furthermore, the current authors expected an association of the sedative dose with rise in cutaneous carbon dioxide tension, but that was also not the case. Therefore, future studies need to analyse the different patient groups with regards to the baseline cutaneous carbon dioxide tension to potentially limit the application of cutaneous capnography to only a specific group of patients.
Acknowledgments
The authors would like to thank F. Baty and A. Schötzau for their assistance with performing the statistical analysis. The authors would also like to thank Sentec AG (Therwil, Switzerland) for providing the combined cutaneous carbon dioxide and oximetry monitoring system.
- Received July 28, 2005.
- Accepted April 10, 2006.
- © ERS Journals Ltd
References










