





Abstract
The aim of the present study was to compare the direct costs of three models for detection of latent tuberculosis infection (LTBI) in routine clinical practice in Switzerland.
Comparison of the overall costs of screening for LTBI, including medical and radiological examination, and preventive treatment associated with three screening models was carried out. Model 1 relies only on the tuberculin skin test (TST) according to the current national guidelines, model 2 relies on T-SPOT®.TB (Oxford Immunotec, Oxford, UK) only and model 3 relies on TST followed by confirmation of positive results by T-SPOT.TB. Costs were taken directly from the clinic's figures. Clinical assumptions were based on the 267 patients who were referred to the clinic over the study period.
Model 3 was found to be the most cost-effective. Using only the skin test (model 1) was the least cost-effective. If only one test for LTBI is to be used, then model 2 (using T-SPOT.TB only) is cheaper than using the TST (model 1).
Screening for latent tuberculosis infection by tuberculin skin test followed by confirmation with T-SPOT.TB is less costly than screening with tuberculin skin test alone, as it allows a reduction in the number of people who receive preventive treatment. In groups with a high proportion of negative tuberculin skin tests, screening with T-SPOT.TB test only may be the most cost-effective.
A key component of tuberculosis (TB) control is the targeted identification and treatment of people carrying a latent TB infection (LTBI), who are at elevated risk of progression to active TB disease 1. To date, the tuberculin skin test (TST) has been relied on to identify those infected who would benefit from treatment. The recent advent of a rapid technique for detecting antigen-specific T-cells direct from blood offers a new approach for detecting Mycobacterium tuberculosis infection 2, 3. The T-SPOT®.TB (Oxford Immunotec, Oxford, UK) test is the regulatory-approved version of the ex vivo enzyme-linked immunospot (ELISPOT) assay for the detection of activated T-cells specific for early secreted antigenic target (ESAT)-6 and culture filtrate protein (CFP)-10 4. These antigens are present in M. tuberculosis but absent from Bacillus Calmette–Guerin (BCG) and most environmental mycobacteria 5, 6. The test is a sensitive and specific marker of M. tuberculosis infection, gives uniformly negative results in healthy unexposed controls (irrespective of BCG vaccination status), and correlates with M. tuberculosis exposure among contacts 7–17. Given the lack of a gold standard for LTBI, these results strongly suggest that this may be a more accurate test than the TST. Other new blood tests using different methodologies based on the principle of detecting interferon-γ released in response to stimulation by ESAT-6 and CFP-10 have also been shown to be able to effectively discriminate TB infection from prior BCG vaccination 18, 19.
As a result of this clinical evidence, there have been growing calls to implement new blood tests into routine clinical practice. However, to date, there has been no published evidence on the cost implications of doing so.
The purpose of the present study is not to examine the absolute cost-effectiveness of LTBI treatment and screening programmes per se, but rather to examine the particular question of whether the new blood test for detection of LTBI (T-SPOT.TB) is cost-effective relative to existing programmes based upon the TST for screening recent contacts of infectious active TB patients. The study was designed to be based on actual clinical and cost data, and to examine the direct costs of implementation of this new blood test to the healthcare provider in terms of their overall budget for latent TB screening and treatment.
MATERIALS AND METHODS
Participants
The data for the analysis came directly from the use of the TST side-by-side with T-SPOT.TB under routine programme conditions at the University Medical Policlinic Lausanne (UMPL, Lausanne, Switzerland). The present authors have been running a study to compare the performance of the two tests in a number of population groups including recent contacts of infectious TB patients. All contacts presenting to the UMPL between January 2004 and December 2005 were included in the present study. A total of 267 participants were included in the study; 144 were Swiss-born and the majority of the foreign-born were immigrants from high incidence countries. In total, 168 had known BCG vaccination histories, with 89.9% (151/168) having received the BCG vaccine.
The TST was applied using the Mantoux method, using 2TU of RT23 PPD, according to the Swiss National Guidelines 20. Results were read at 72 h and considered positive if induration was ≥10 mm. All TSTs were placed and interpreted by experienced operators. For the T-SPOT.TB test, a 10 mL blood sample was taken and analysed in a local analytical laboratory (BBR-LTC Laboratories, Lausanne, Switzerland). The cut-off for the assay was ≥6 spots, according to the manufacturer's instructions.
According to the Swiss National Guidelines, contacts with a TST ≥10 mm are offered a preventive treatment with isoniazid for 9 months. Contacts who refuse the preventive treatment are offered a clinical follow-up for 2 yrs.
The raw data from the results of both tests, used in the subsequent cost-effectiveness analysis, are shown in table 1⇓. Of the 267 contacts, 193 (72.3%) were positive by TST. Seventy-four (27.7%) were positive by T-SPOT.TB. Only 33.7% (65 out of 193) of the TST-positive individuals were also positive by the T-SPOT.TB test. There were nine individuals who were T-SPOT.TB positive and TST negative.
Comparative results of the tuberculin skin test(TST) and T-SPOT®.TB tests in all 267 contacts using a TST cut-off of 10 mm
Models
A simple decision-tree analysis was constructed representing different possible clinical pathways for the diagnosis and subsequent treatment of LTBI (fig. 1⇓). Three scenarios were modelled as follows: model 1 captures current practice where the TST is used as the only tool to diagnose LTBI, model 2 calculates the costs of using T-SPOT.TB alone as the only tool to diagnose LTBI (i.e. a complete replacement for the TST), and model 3 calculates the costs of using the TST for the initial screening of patients, followed by a T-SPOT.TB test in all TST-positive individuals prior to treatment. The clinical and cost-effectiveness basis for model 3 has also been put forward by the UK National Institute for Clinical Excellence (NICE) in draft guidelines for the implementation of new blood tests for TB 21.
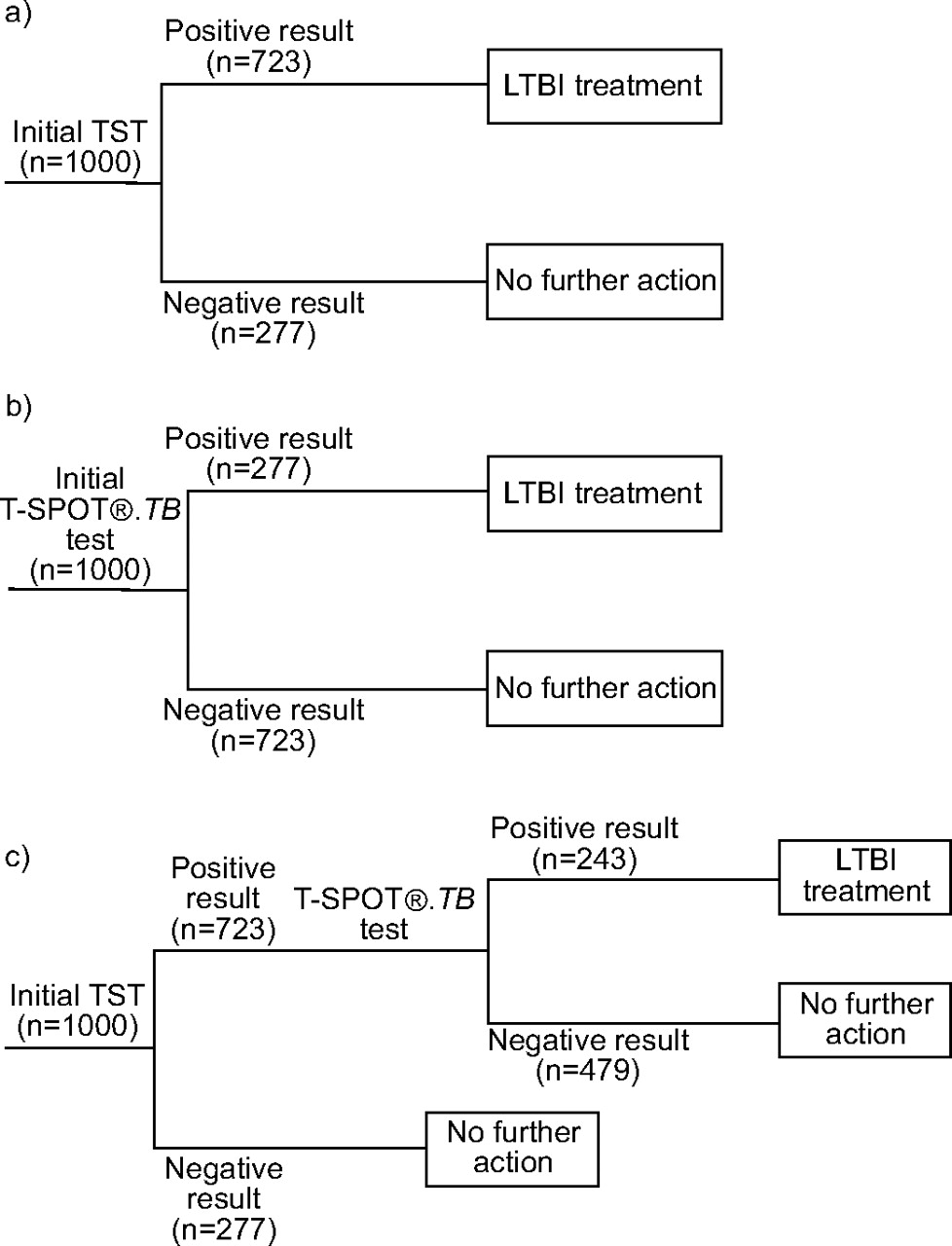
The three decision-tree clinical pathway models (models 1–3). a) Model 1: base case – costs of screening using the tuberculin skin test (TST) alone according to the Swiss guidelines 1. b) Model 2: T-SPOT®.TB screening – costs of screening if T-SPOT.TB were to replace TST entirely as the only tool for detecting latent tuberculosis infection (LTBI). c) Model 3: T-SPOT.TB as confirmatory test – costs of screening using TST as the first-line tool, followed by T-SPOT.TB in TST +ve individuals to rule out false positives. The overall cost results, with data and costs normalised to a cohort size of 1,000 subjects and using a skin test cut-off of 10 mm according to the Swiss guidelines 1 are as follows. a) Total cost of initial screening = CHF35,000 (\#8364;22,575); total cost of treatment = CHF1,043,790 (\#8364;673,245); overall total cost = CHF1,078,790 (\#8364;695,820). b) Total cost of initial screening = CHF200,000 (\#8364;129,575); total cost of treatment = CHF400,210 (\#8364;258,135); overall total cost = CHF600,790 (\#8364;387,135). c) Total cost of initial screening = CHF35,000 (\#8364;22,575); total cost of confirmatory test CHF144,569 (\#8364;93,247); total cost of treatment = CHF351,536 (\#8364;226,740); overall total cost = CHF531,105 (\#8364;342,563). CHF: Swiss Francs.
Each model was run for a hypothetical cohort of 1,000 patients, with the model inputs for the test results directly extrapolated from the actual results shown in table 1⇑.
The models represent a direct-cost analysis from the point of view of the healthcare provider. No consideration was given to costs and quality-of-life losses on the part of the patient; in addition, no consideration was given to wider transmission of TB in the community. No time discounting was necessary, as all the costs in each clinical pathway were assumed to be incurred during a 1-yr period. The present authors also did not account for the costs of repeated TSTs, which are in practice often administered in dubious or potentially boosted cases.
Costs were taken directly from the published dispensary costs at the UMPL as shown in table 2⇓, and expressed in both Swiss Francs (CHF) and Euros (at a rate of CHF1 = \#8364;0.645). The cost of LTBI treatment includes an initial chest radiograph to rule out active TB prior to treatment, the cost of 9 months of isoniazid and the cost of clinician visits and liver function tests during the treatment period. Costs associated with bacteriological examination of sputum, if indicated, and side-effects from isoniazid treatment were ignored. All patients in whom preventative therapy was indicated were assumed to complete the full course of therapy. As no reimbursement amount has yet been established in Switzerland for the T-SPOT.TB test, a figure of CHF200 (\#8364;129) was taken as an initial sum taken to estimate the costs of the test, associated consumables and labour required to perform the test both in the laboratory and the physician's office. The costs of the T-SPOT.TB test were subsequently explored in a sensitivity analysis.
Costs of latent tuberculosis infection(LTBI) tests and treatment used as inputs for cost-effectiveness models
RESULTS
Figure 1⇑ shows how the costs, combined with the actual clinical data, allow the full costs of each clinical pathway to be calculated. The total cost of the TST only pathway (model 1) is CHF1,078,790 (\#8364;695,820), the initial cost of screening 1,000 contacts with the TST is CHF35,000 (\#8364;22,575) and the costs of subsequently treating the 723 TST-positive individuals for LTBI is CHF1,043,790 (\#8364;673,245). The overall cost of using T-SPOT.TB only (model 2) is lower at CHF600,210 (\#8364;387,135) because, although the initial costs of screening are higher, fewer people receive treatment. As treatment costs are substantially higher than the costs of screening by either test, this results in an overall cost saving. Model 3 is marginally cheaper than model 2, costing CHF531,105 (\#8364;342,563) for 1,000 patients.
These results show that the costs of an LTBI screening and treatment programme targeted solely at high-risk groups currently costs CHF1,079 (\#8364;696) per patient (table 3⇓). Switching solely to the T-SPOT.TB test in place of the TST would reduce costs by 44% and using both tests together according to the clinical pathway in model 3 would reduce costs by 49%.
Overall costs of a latent tuberculosis infection screening and treatment programme#
A sensitivity analysis of the cost of the T-SPOT.TB test was also performed (table 4⇓); this calculated the overall cost of the T-SPOT.TB test at which models 2 and 3, respectively, would become cost neutral to the current testing paradigm (model 1). The results show that if T-SPOT.TB was used as a direct replacement for the TST it would be cost neutral at an overall cost of CHF679 (\#8364;438). If T-SPOT.TB was used as a subsequent test after an initial TST, this strategy would be cost neutral at an overall cost for T-SPOT.TB of CHF958 (\#8364;618). The cost of T-SPOT.TB at which using it alone would be the cheapest strategy was calculated; model 2 would become dominant if the price of T.SPOT.TB was ≤CHF131 (\#8364;84).
A simple sensitivity analysis of the cost of performing the T-SPOT®.TB test, reporting the overall costs of the T-SPOT.TB test at which models 2 and 3 would be cost neutral compared with the current latent tuberculosis infection (LTBI) screening guidelines using only the tuberculin skin test (TST)#
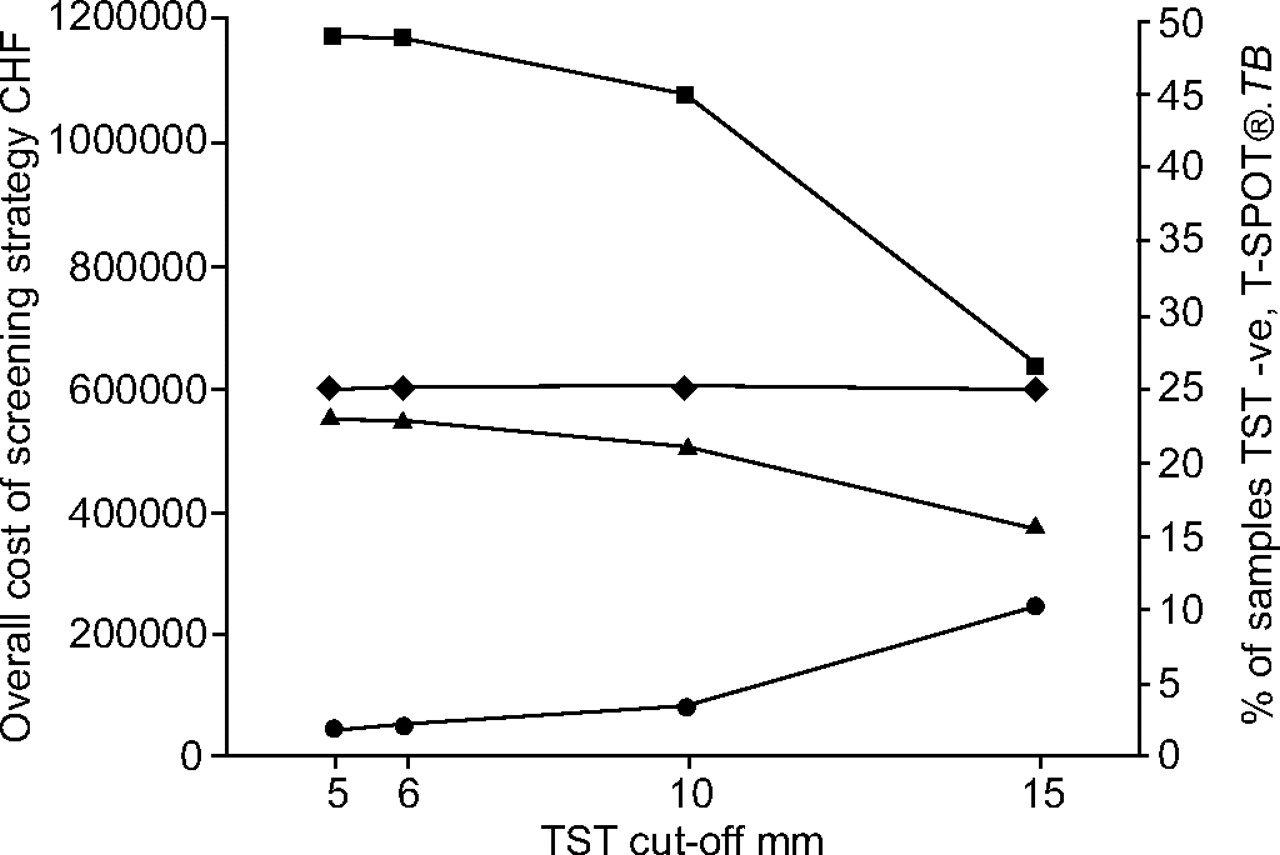
As the induration size for the TSTs was recorded, modelling of the effect of applying different TST cut-offs on the resulting cost of the three screening strategies was also possible. The results are shown in figure 2⇓. Results with TST cut-off values of 5, 6 and 15 mm were calculated from the clinical data, as these cut-offs correspond to those used in other European countries. The costs of model 2 (T-SPOT.TB only) clearly do not change with TST cut-off, as this screening strategy does not involve the TST. However, as increasing TST cut-off decreases the number of people deemed to be infected, the costs of both models 1 and 3 decrease with increase in the cut-off size from 10 to 15 mm (to 59 and 70% over the 10-mm totals, respectively). Decreasing the TST cut-off value from 10 to 5 mm increases the costs of models 1 and 3, although this effect is relatively small (10 and 7% increase, respectively). Nonetheless, at all TST cut-off values modelled, the relative costs of each screening strategy were consistent; with model 3 being the cheapest, followed by model 2 and, lastly, model 1. As higher TST cut-offs increase the specificity of the TST at the cost of sensitivity, the current authors also calculated the proportion of the cohort who were T-SPOT.TB positive but TST negative, as a surrogate for the risk of TST false-negatives. The risk of TST false-negatives increased from 1.9 to 10.1% as the TST cut-off increased from 5 to 15 mm (fig. 2⇓).

{kind=link}
{kind=link}
The variation of the overall costs of the three screening strategies, and the risk of false-negative tuberculin skin test (TST) results (approximated as those samples that were TST -ve but T-SPOT®.TB +ve) with TST cut-off. ▪: Model 1 (TST only); ♦: model 2 (T-SPOT®.TB only); ▴: model 3 (TST followed by T-SPOT®.TB); •: risk of false-negative TSTS. CHF: Swiss Francs.
DISCUSSION
Previous cost-effectiveness methodologies for LTBI screening and treatment have used iterative Markov processes to examine the overall costs to the healthcare system over periods of 15–20 yrs 22–28, and have included the costs of TB reactivation and drug side-effects, with or without including the costs of loss of quality-of-life and the costs of wider TB transmission. The present authors chose instead to focus only on direct costs over a much shorter time period, for a number of reasons.
First, the present authors wanted the model to use only actual clinical data, rather than epidemiological assumptions derived from the literature that may or may not accurately reflect the local situation 29. By taking this approach, it was possible to use the clinical results of the present authors' 2-yr long comparison of both tests side-by-side. The results therefore reflect the reality of the TB screening and treatment programme in a low-incidence region, such as Lausanne, Switzerland.
Secondly, many individual hospitals and public health services, when faced with increasing pressure on healthcare costs and a fixed annual budget to provide TB control, will quite legitimately be examining how the introduction of new technology will impact their annual budget, rather than the overall costs of TB to wider society over a 20-yr timeframe. The restriction of the present model to a simple clinical pathway enables healthcare payers to quickly calculate the actual direct costs of implementing the T-SPOT.TB test and how it will affect their yearly budgets for TB control.
Lastly, the simplicity of the model construction allows the model to be quickly and easily applied to different geographical locations and screening situations, based on actual clinical data that can be easily obtained from pilot studies.
The results of the present study demonstrate that the cheapest clinical pathway in all situations modelled was model 3; using an initial TST followed by T-SPOT.TB only in TST-positive individuals. This finding is consistent with the findings and recommendations presented in the UK NICE Guidelines 21. It is interesting that this overall conclusion is not affected by the TST cut-off used; and makes the findings from this study potentially applicable to different countries where different TST cut-off values are used. Clearly the potential difficulty of implementing model 3 into clinical practice is that it does not take into account people who may be TST negative, but T-SPOT.TB positive. These people may be at risk of TB reactivation, but would not receive treatment. In the cohort examined in Lausanne, this was not a significant factor as there were only nine such individuals in the 267 contacts, representing 3.3% of all results.
However, if populations are considered where the TST suffers from considerable anergy (for example, young children, and HIV and other immunosuppressed patients), where it is likely that T-SPOT.TB will identify truly infected patients missed by the TST 17, 30–32, then model 3 may no longer be appropriate. Clearly, this argument would also apply to other populations where there is a hidden risk of immunosuppression, such as immigrants with a high probability of undeclared HIV infection. In addition, the present study's results show that in situations where higher TST cut-offs are used, the risk of false-negative TST results can be significant; 10.1% of the present study cohort would have been considered infected by T-SPOT.TB but not by the TST, if a cut-off value of 15 mm had been used. To truly understand the cost saving that would result from using T-SPOT.TB in these populations, either on its own (model 2) or according to another clinical algorithm, would require a Markov-type analysis that could compute the cost-savings from the cases of TB averted by early identification and treatment of people at high risk of reactivation. This was outside the scope of the present study, but this is clearly an important area for future research.
Notwithstanding this future analysis, as the difference in cost was relatively small (11.5%) between models 2 and 3, the clarity of a simplified testing algorithm, the convenience of fewer return visits and the clinical benefit of fewer potential false-negative results afforded by using only T-SPOT.TB may nonetheless make model 2 the preferred strategy over time. Similarly, if the cost of the test could be reduced to <CHF131, then model 2 also becomes the cheapest option, in addition to these other benefits.
To the best of the present authors' knowledge, this is the first analysis of the costs of using a new blood test for tuberculosis infection. Although the detailed costs may change, the present authors believe that the overall results are likely to be applicable to any developed world setting where there is a high proportion of positive tuberculin skin test results, many of whom are due to prior Bacillus Calmette–Guerin vaccination in adults 33 and children 34, and where the main cost of the tuberculosis control programme is thus due to preventive treatment of individuals identified to be infected by the tuberculin skin test. The present results show that using T-SPOT®.TB is likely to bring about substantial direct cost savings in tuberculosis control programmes.
Acknowledgments
The authors would like to thank the Laboratoire BBR Lausanne (director A. Zellweger) and the local staff for running the T-SPOT®.TB tests.
- Received January 15, 2006.
- Accepted March 29, 2006.
- © ERS Journals Ltd
References










