





Abstract
A prospective study was performed to evaluate the diagnostic accuracy of N-terminal-pro-B-type natriuretic peptide (NT-proBNP) levels, measured simultaneously in serum and pleural fluid, in identifying pleural effusions due to heart failure.
Pleural fluid and serum samples from all patients presenting for thoracentesis between April 2004 and May 2005 were simultaneously collected. The discriminative properties of NT-proBNP levels in identifying pleural effusions due to heart failure were determined by receiver operating characteristic curve analysis and compared to the diagnostic value of finding a transudate by Light's criteria.
Ninety-three patients were evaluated, 27% with cardiac effusion and 73% with exudative effusions of various cause. Levels of NT-proBNP in pleural fluid and serum correlated closely. Serum and pleural fluid NT-proBNP levels were significantly elevated in patients with cardiac effusion. With a cut-off value of 4,000 ng·L−1, NT-proBNP levels in pleural fluid and serum displayed comparably high diagnostic accuracies of 92 and 91%, respectively. All patients misclassified by Light's criteria were correctly identified by measuring NT-proBNP levels.
N-terminal-pro-B-type natriuretic peptide levels in either pleural fluid or serum showed a high diagnostic accuracy compared to traditional criteria. Thus measuring N-terminal-pro-B-type natriuretic peptide is a valuable additional diagnostic tool for the detection or exclusion of cardiac origin of pleural effusions.
The differentiation of pleural effusions resulting from heart failure from those of other causes is usually made by clinical criteria supported by the finding of a transudative effusion according to the criteria of Light 1 (table 1⇓). However, as these criteria were developed to detect exudative pleural effusions with a high sensitivity for not overlooking underlying causes such as infections and malignancies, their ability to exclude transudative effusions is lower 1, 2. Some studies have found a considerable proportion of patients with pleural effusions due to heart failure being misclassified as exudative 3, 4, especially after having received diuretic therapy 5. The finding of an exudative effusion usually requires an extensive diagnostic work-up. Thus a diagnostic dilemma in patients with exudative pleural effusions and clinical heart failure might result, leading to an unnecessary exposure to invasive and expensive diagnostic procedures. Conversely, thoracentesis itself presents considerable risk of complications and is associated with discomfort to the patient. Thus a strategy of identifying pleural effusions due to heart failure and possibly avoiding unnecessary diagnostic thoracenteses and/or further diagnostic procedures would be an attractive and potentially beneficial approach.
Light's criteria for defining transudative pleural effusions#
B-type natriuretic peptide (BNP) is a vasoactive peptide predominantly secreted by the heart. Its precursor molecule, pro-BNP, is cleaved to give the inactive N-terminal-pro-BNP (NT-proBNP) and the biologically active BNP. The synthesis of these peptides is stimulated by increased tension or stretching of the cardiac ventricle wall. NT-proBNP measured in serum is a sensitive marker of cardiac dysfunction and proven to be a useful tool in the diagnosis of acute and chronic systolic and diastolic left ventricular heart failure 6–9.
Since 2004, there has been some interest in the investigation of these peptides as markers for pleural effusions due to heart failure. To date, two studies have examined NT-proBNP 10, 11 and one BNP 12, with all uniformly suggesting a potential value of these peptides in predicting or ruling out heart failure as a cause of pleural effusions. There are, however, several limitations to these trials as they either measured the peptides only in pleural fluid 11 or plasma 12, were retrospective in design 11 or included only 28 selected patients to analyse 10.
The aim of the present study was to prospectively evaluate the diagnostic accuracy of NT-proBNP levels, measured simultaneously in serum and pleural fluid, in identifying pleural effusions due to heart failure in all patients presenting for thoracentesis at the Dept of Pulmonology of Dresden University Hospital (Dresden, Germany) between April 2004 and May 2005.
METHODS
Pleural fluid and serum samples were collected prospectively from all patients presenting at the Dept of Pulmonology of Dresden University Hospital, a tertiary care referral centre for diagnostic or therapeutic thoracentesis, between April 2004 and May 2005. In patients presenting repeatedly for thoracentesis, only the first episode was included. Pleural fluid and serum samples were obtained, preferably simultaneously, but a maximum time difference of ±8 h was accepted. Biochemical analysis, bacterial and fungal culture, acid-fast bacilli smear, PCR for Mycobacterium tuberculosis complex DNA, and cytological examinations (with flow cytometry if appropriate) were performed for all pleural fluid samples shortly after thoracentesis, whereas serum samples were sent for biochemical analysis. Measurement of NT-proBNP levels in serum and pleural effusion and all other biochemical analyses were carried out within 4 h after specimen collection.
Any further diagnostic work-up was left to the discretion of the attending physicians, but echocardiography was performed in all patients with suspected pleural effusion due to heart failure.
The study protocol was approved by the ethics committee of the medical faculty of Dresden University of Technology (Dresden, Germany), and informed consent was obtained from the participants.
Serum and pleural fluid total protein, lactate dehydrogenase (LDH) and cholesterol levels were measured using test kits from Roche Diagnostics (Mannheim, Germany) and a Hitachi 917 analyser (Roche Diagnostics). The upper normal limit for serum LDH with the test kit used is 213 U·L−1 in females and 225 U·L−1 in males. NT-proBNP was measured by electrochemiluminescence immunoassay using the Elecsys 2010 (Roche Diagnostics) according to the manufacturer's protocol. According to the manufacturer, this test has an intra-assay coefficient of variation of 0.8–3% and a detection range of 5–35,000 ng·L−1. Higher values were obtained by diluting samples 1:10 or 1:100.
After the termination of the study, when the last included patient had been discharged from hospital, clinical diagnosis was established independently from the biochemical data by reviewing the hospital records of all patients.
The diagnosis of heart failure was based on findings of the typical clinical picture of decompensated heart failure, including history, physical examination, chest radiography and response to diuretic therapy, and confirmed by echocardiographical evidence of left ventricular systolic dysfunction (left ventricular ejection fraction of ≤40%), severe valvular disease (grade II or III) or severe left ventricular diastolic dysfunction; all patients with pleural effusions due to heart failure had New York Heart Association Functional Class III or IV symptoms.
Malignant effusions were diagnosed when malignant cells were detected on cytological examination of pleural fluid or in lung biopsy specimens in the absence of other causes of pleural effusion.
Parapneumonic effusions or pleural empyemas were associated with the clinical and radiological diagnosis of acute pneumonia or the detection of pus or a positive bacterial culture in pleural fluid.
Other, rare, causes of exudative pleural effusions were defined by clear clinical pictures or established diagnostic criteria (post-cardiac injury syndrome, acute pleuritis, post-operative effusion, collagen disease, pleural tuberculosis, chylothorax).
Data from the biochemical analyses, including NT-proBNP levels, are presented as median (interquartile range). Medians were compared using the nonparametric Mann–Whitney U-test, and qualitative variables were compared using Fisher's exact test. The correlation between pleural fluid and serum NT-proBNP concentration was tested using Spearman's coefficient of rank correlation. Sensitivity, specificity, positive predictive value, negative predictive value and accuracy were calculated according to standard formulae. Exact binomial 95% confidence intervals (CI) were calculated for all operational characteristics. Receiver operating characteristic (ROC) curve analysis was used to determine the discriminative properties of various cut-off levels of NT-proBNP. A p-value of <0.05 (two-sided) was considered significant. The regression equation was calculated as described previously according to the Passing and Bablok 13 method.
RESULTS
Pleural fluid and serum samples were collected from 101 consecutive patients presenting for thoracentesis at the Dept of Pulmonology between April 2004 and May 2005. Eight (8%) patients, for whom a definite diagnosis could not be established from the hospital records, were excluded from the analysis. The remaining 93 patients were divided as follows, according to the aforementioned criteria, amongst the following diagnoses: 25 (27%) with effusions due to heart failure, 40 (43%) with malignant effusions, 15 (16%) with parapneumonic effusions or pleural empyema, and 13 (14%) with exudative pleural effusions due to other causes (four acute pleuritis, three post-cardiac injury syndrome, three after local surgery, one collagen disease, one pleural tuberculosis and one chylothorax).
Of the patients diagnosed with pleural effusion due to heart failure, 18 (72%) suffered from systolic heart failure with a median (interquartile range) left ventricular ejection fraction of 30% (25–40%), four (16%) patients had acute decompensated left ventricular valvular defects of grade II and III and three (12%) patients presented with lung congestion due to severe left ventricular diastolic dysfunction associated with pulmonary venous hypertension, established by heart catheter examination.
As expected, patients with cardiac transudates were of greater age, more often had a history of chronic heart failure, myocardial infarction, renal failure or diabetes mellitus, more often presented with bilateral effusions and had significantly lower pleural fluid levels and pleural fluid to serum ratios of protein, LDH and cholesterol (table 2⇓). However, patients with exudative effusions frequently suffered from comorbid illnesses, with 27 (40%) of them having a history of chronic, nondecompensated heart failure.
Characteristics of study participants
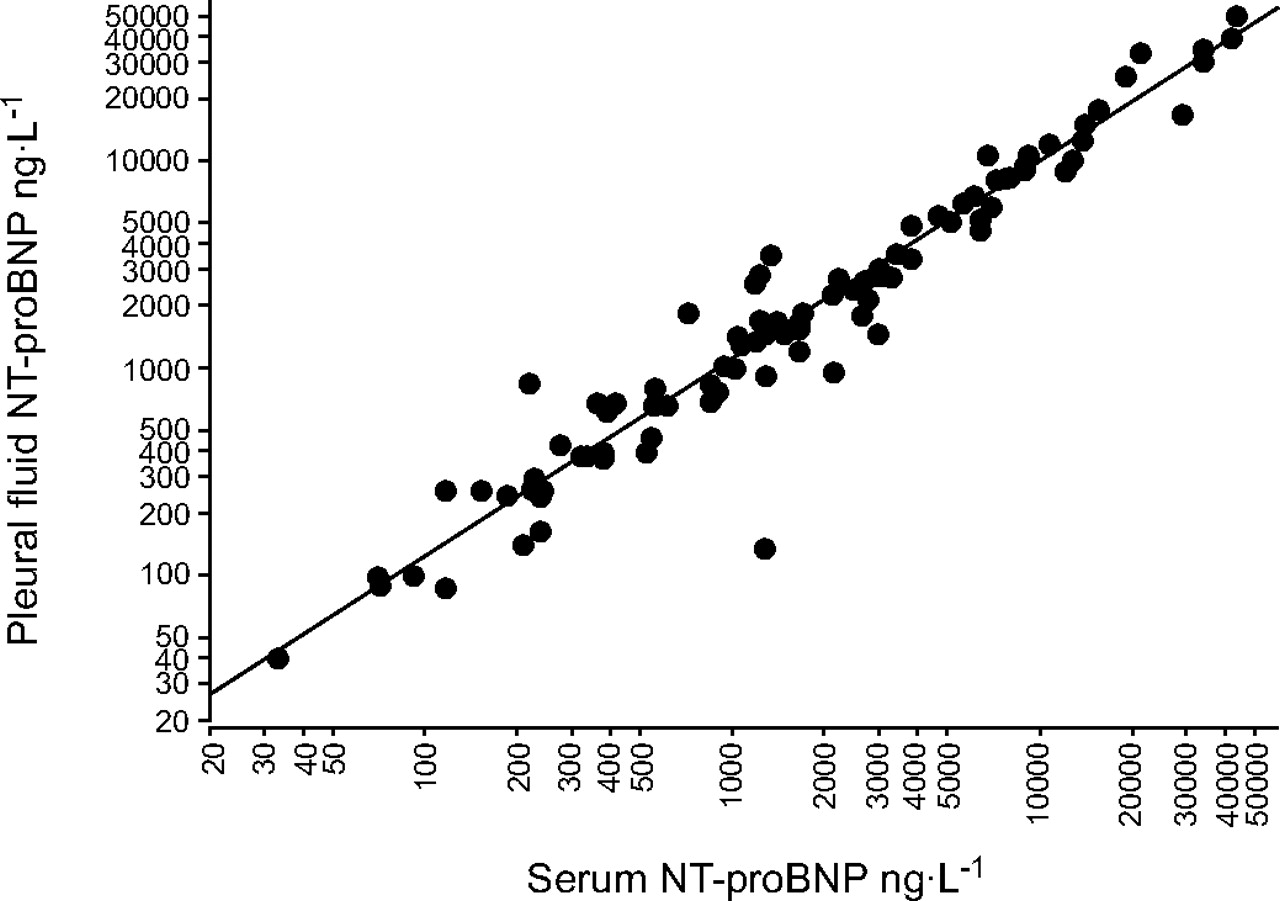
Levels of NT-proBNP measured in pleural fluid and in serum correlated closely (Spearman's coefficient of rank correlation 0.96; p<0.001; fig. 1⇓).

Correlation of serum and pleural effusion levels of N-terminal-pro-B-type natriuretic peptide (NT-proBNP). Spearman's coefficient of rank correlation is 0.963 (95% confidence interval (CI) 0.944–0.975; p<0.001). Regression equation according to Passing and Bablok 13 method: serum NT-proBNP = −12.967+0.959×pleural fluid NT-proBNP; intercept A = −12.967 (95% CI −59.000–12.414); slope B = 0.959 (95% CI 0.908–1.000). The scale is a logarithmic scale.
Median (interquartile range) levels of NT-proBNP in pleural fluid or serum among patients with pleural effusion due to heart failure were significantly higher (10,427 (7,366–21,844) ng·L−1 in pleural fluid; 10,791 (6,588–20,263) ng·L−1 in serum) than in patients with noncardiac causes (947 (372–1,937) ng·L−1 in pleural fluid; 989 (296–1,691) ng·L−1 in serum; all p<0.0001; fig. 2⇓, table 2⇑).
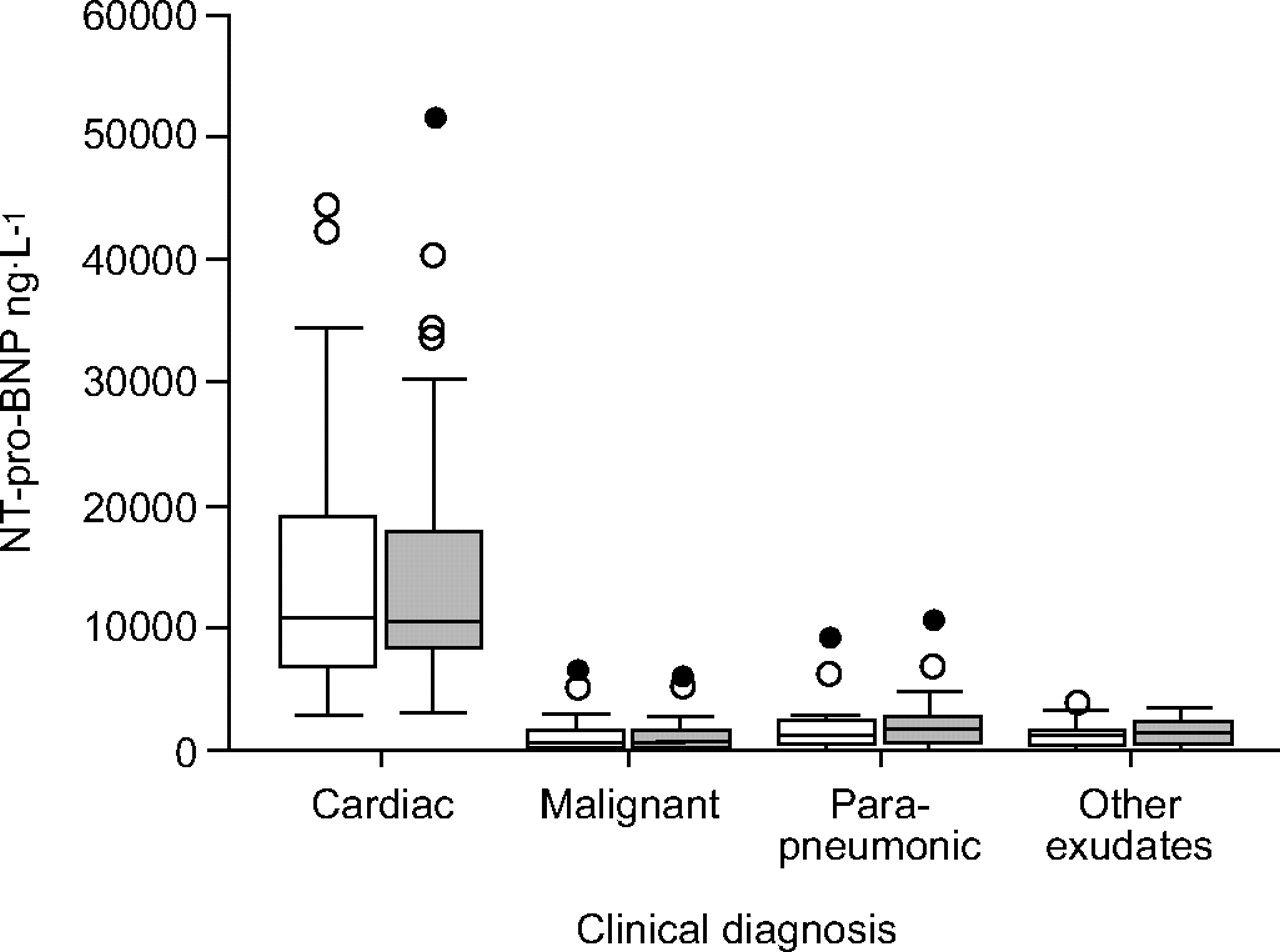
Box-plots showing N-terminal-pro-B-type natriuretic peptide (NT-proBNP) levels in serum (□) and pleural effusion (▒) by clinical diagnosis. Boxes represent median and interquartile range (○: outliers; •: extremes).
Measurement of NT-proBNP levels in pleural fluid and serum displayed high diagnostic accuracy, as shown by ROC curve analysis (area under the curve 0.98 for both; fig. 3⇓). Linear discriminant analysis after logarithmic transformation of NT-proBNP levels revealed nearly identical cross-validated discriminative properties for measurement in pleural fluid and serum. As determined by ROC curve analysis, an NT-proBNP cut-off value of 4,000 ng·L−1 in pleural fluid and serum had a sensitivity of 92% (95% CI 74–99%) and 88% (95% CI 69–97%) and a specificity of 93% (95% CI 84–98%; both the same), each with an overall diagnostic accuracy of 92% (95% CI 85–97%) and 91% (95% CI 84–96%), respectively (table 3⇓).

{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve of N-terminal-pro-B-type natriuretic peptide (NT-proBNP) levels (1: 3,000 ng·L−1; 2: 4,000 ng·L−1; 3: 7,000 ng·L−1) in serum (––––) and pleural effusion (-----) for differentiating between cardiac and noncardiac pleural effusions (area under the curve 0.98 for both serum and pleural effusion (95% confidence interval 0.96–1.00)).
Predictive potential of>4,000 ng·L−1 N-terminal-pro-B-type natriuretic peptide (NT-proBNP) in the classification of transudative cardiac pleural effusions
In the present patient group, where transudative effusions were caused by heart failure alone, it was possible to calculate the comparative diagnostic properties of Light's criteria in detecting cardiac effusions in a post-hoc analysis: the finding of a transudate was associated with a low sensitivity of 64% (95% CI 43–82%). As expected, their specificity in the exclusion of exudative effusions was high at 93% (95% CI 84–98%), leading to an overall diagnostic accuracy of 85% (95% CI 76–92%). Nine of the 25 (36%) patients with pleural effusion due to heart failure were falsely classified as exudative by Light's criteria. All of them exhibited NT-proBNP levels of >4,000 ng·L−1. The characteristics of these nine patients are shown in table 4⇓; all except one received diuretic therapy. Conversely, all five patients with exudates falsely labelled as transudates by Light's criteria showed NT-proBNP levels of <4000 ng·L−1, three of them having confirmed malignant effusions.
Characteristics of patients with pleural effusion due to heart failure misclassified as exudative by Light's criteria
DISCUSSION
The serum NT-proBNP level is an established marker for the assessment of cardiac function, and has successfully been used as a tool for the diagnosis and management of acute and chronic heart failure, including systolic and diastolic left ventricular dysfunction and valvular disease 6–9, 14. Especially in the emergency care setting, NT-proBNP levels are a valuable addition to clinical judgement for the identification or exclusion of acute heart failure as a cause of dyspnoea 6. Measurement of BNP and NT-proBNP in serum were shown to perform equally well in predicting acute heart failure 15.
In patients presenting with pleural effusion, the current findings demonstrate that levels of NT-proBNP in serum and pleural fluid are significantly elevated, ∼10-fold, in patients in whom acute decompensated left heart failure could be identified as the cause of the effusion compared to patients with noncardiac effusions. Moreover, elevated NT-proBNP levels displayed a high sensitivity and specificity in detecting cardiac transudates in this patient group over a relatively large range of cut-off values (fig. 3⇑).
Compared with the finding of a transudate using the established Light's criteria in the present patient group, in whom transudative pleural effusions were only attributed to heart failure, it was found that NT-proBNP levels in serum and pleural fluid discriminate more accurately between cardiac versus noncardiac effusions. In accordance with the literature, Light's criteria exhibited high ability in the exclusion of exudates, but the finding of a transudate showed a low sensitivity of 64% in the identification of cardiac effusions. In patients misclassified by Light's criteria in either way, NT-proBNP levels were always able to correctly detect or exclude a cardiac origin of the effusion. Thus Light's criteria remain the diagnostic standard for the exclusion of exudative effusions, but measurement of NT-proBNP levels proved to be a valuable supplementary diagnostic tool, which, according to the present data, strongly suggests a cardiac origin of the effusion at levels >4,000 ng·L−1, and, conversely, makes cardiac effusions very unlikely at levels of <4,000 ng·L−1 (fig. 3⇑). These data are in general agreement with the other studies examining this issue.
One recently published study by Gegenhuber et al. 12 examined plasma levels of BNP in 64 prospectively enrolled consecutive patients, 31 with pleural effusions due to heart failure, two with transudative effusions of different origin and 24 with exudative effusions. They reported a diagnostic accuracy for plasma BNP levels of 93% in the identification of cardiac effusions, comparable to the data found in the present study with NT-proBNP.
Tomcsanyi et al. 10 prospectively compared NT-proBNP levels in pleural fluid and serum in 14 patients with pleural effusion due to congestive heart failure and 14 patients with pleural exudates of various cause. In this small study, the authors found significantly higher levels of NT-proBNP in either serum or pleural fluid from patients with cardiac effusions (median 6,295 versus 277 ng·L−1 in pleural fluid; 5,713 versus 236 ng·L−1 in serum) and suggested a diagnostic cut-off point for detecting cardiac transudates of 599–1,457 ng·L−1. However, patients with exudative effusions and coexisting chronic heart failure were excluded from their analysis.
Porcel et al. 11 retrospectively examined NT-proBNP levels in the pleural fluid of a cohort of 117 patients after thoracentesis, randomly selected from a larger database, of whom 44 (38%) were diagnosed as having pleural effusion due to acute heart failure. Consistent with the present data, the authors detected significantly higher median levels of NT-proBNP in cardiac effusions (6,931 ng·L−1) compared to exudative effusions (292 ng·L−1). From their data, they calculated a diagnostic cut-off point of 1,500 ng·L−1 for detecting cardiac transudates with a sensitivity of 91% and a specificity of 93%. NT-proBNP levels in serum were not measured in their study.
As in the present study, both authors measured NT-proBNP levels using a commercial electrochemiluminescence immunoassay and an Elecsys 2010 analyser (Roche Diagnostics).
Although the NT-proBNP levels of the present patients with pleural effusions due to heart failure are comparable to those determined by the former two groups, approximately three-fold higher median NT-proBNP levels were detected in the present patients with exudative effusions (table 2⇑), resulting in a suggested cut-off value that is approximately three-fold higher. Unlike the other two studies, the present prospective data present the results from nonselected consecutive patients with pleural effusion. This led to the inclusion of a considerable proportion (40%) of patients with noncardiac exudative effusions suffering from coexisting mild-to-moderate chronic but not decompensated heart failure, including chronic right and/or left ventricular dysfunction, chronic cardiac valve disease and/or chronic atrial fibrillation (table 2⇑), conditions known to be associated with elevated NT-proBNP levels. Moreover, of the present patients with exudative effusions, 19% had a history of diabetes mellitus and 16% of impaired renal function, diseases that can also cause elevated NT-proBNP-levels 16. The discrepancy in NT-proBNP levels might be explained by the high frequency of these comorbid conditions in the present nonselected patient group, frequently suffering from thoracic malignancies and pleural empyema, which mainly occur in elderly patients with multiple comorbid conditions. Thus they possibly represent a more realistic group of control subjects. This suggestion is supported by the finding of a study evaluating NT-proBNP concentrations in serum as a diagnostic tool for the detection of reduced left ventricular systolic function in a cohort of 2,193 consecutive hospital in-patients 17. The authors divided the patients into three groups and found median NT-proBNP levels of 7,273 ng·L−1, 2,368 ng·L−1 and 685 ng·L−1 in patients with an LVEF of ≤40%, >40% and >50%, respectively. Based on this data from consecutive hospitalised patients, the median serum NT-proBNP level of 989 ng·L−1 seen in the present patient group with noncardiac pleural effusions and a high frequency of comorbid conditions, including nondecompensated chronic heart failure, lies well within the expected range. Thus, the present authors' suggested a higher cut-off value of 4,000 ng·L−1 might be more appropriate in accurately predicting a cardiac origin of pleural effusions while minimising of the risk of overlooking additional underlying diseases. Conversely, the possibility that the present results and the corresponding cut-off values have also been biased due to the limitations of the study, discussed below, cannot be excluded. Thus further prospective trials on large nonselected patient groups are needed in order to confirm these issues.
The other interesting finding of the present study is the close correlation between NT-proBNP levels in pleural fluid and serum, leading to equal diagnostic efficacy in the identification of cardiac effusions. This confirms the data of Tomcsanyi et al. 10, who found a comparably high correlation. To date, the origin of NT-proBNP in pleural fluid is unclear, although it has been suggested that it derives from serum NT-proBNP, and might diffuse easily into the pleural space due to its small molecular size 18. Thus there seems to be no additional value in measuring NT-proBNP in pleural fluid.
There are several limitations to the present study. First, the examination of a relatively small prospective group of 93 consecutive patients means that the present results need to be confirmed in larger studies.
Secondly, since the study was designed as a pilot study to prospectively examine the diagnostic discriminative properties of NT-proBNP levels between cardiac and noncardiac pleural effusions and to suggest cut-off values for further studies, the small subset of eight patients in whom a definite diagnosis could not be established from the hospital records had to be excluded from the analysis, although this might be a subgroup of potential interest in studying the predictive properties of NT-proBNP level.
Thirdly, it was not possible to include any transudative pleural effusions of noncardiac origin, such as effusions associated with hepatic or renal disease. Examining the diagnostic utility of NT-proBNP level in this patient group would be of particular interest, since Light's criteria are not able to discriminate between them. Moreover, the preliminary data from Porcel et al. 11 suggest a potential value of NT-proBNP level for this indication.
Fourthly, as the diagnosis of pleural effusion due to heart failure is usually based on clinical criteria supported by the finding of a transudate, it cannot be concluded, from the present data, whether or not NT-proBNP measurement would be of any additional diagnostic value compared to the clinical impression of the treating physician; this issue remains subject to further studies 18.
Fifthly, there were several factors related to the study design potentially biasing the present results. Echocardiography was performed in all patients with suspected pleural effusion due to heart failure; in all other patients this was left to the discretion of the attending physician. Thus, in a minority of 25 of the 68 patients diagnosed as having noncardiac effusions, who were all without any clinical signs suggestive of heart failure, echocardiography was not performed and underlying heart disease, although less probable, cannot be entirely excluded. As a small proportion of patients with pleural effusion due to heart failure or malignancy referred for therapeutic rather than diagnostic thoracentesis were included, this might have biased the disease prevalence of heart failure in the present patient group and thus the diagnostic properties calculated for NT-proBNP level. Finally, although the study-relevant diagnosis was established independently from the biochemical data, the attending physicians treating the patients were not blinded to the NT-proBNP results. The possibility cannot be excluded that this diagnostic information might have influenced further diagnostic approaches and thus, again, potentially biased the study results.
In conclusion, NT-proBNP levels in either pleural fluid or serum showed high diagnostic accuracy in identifying cardiac transudates. Thus they might be valuable additional diagnostic tools for the detection or exclusion of a cardiac origin of pleural effusions. From the present data, it can be suggested that cut-off levels in nonselected patient groups might be higher than those previously reported 10, 11 to avoid overlooking underlying causes other than heart failure in the often multimorbid patients presenting with pleural effusions. However, larger prospective studies are needed to confirm the cut-off points in nonselected patient groups and to examine the discriminatory properties of NT-proBNP level in differentiating transudates of noncardiac origin. It would also be interesting to compare the diagnostic properties of NT-proBNP level with the clinical suspicion of the treating physician in addition to the finding of Light's criteria in the identification of cardiac effusions.
As N-terminal-pro-B-type natriuretic peptide levels in serum and pleural fluid correlate closely, and measurement of N-terminal-pro-B-type natriuretic peptide in serum showed equally good diagnostic properties, examination in serum alone might be a promising diagnostic tool for the suggestion of pleural effusion due to heart failure with an acceptable positive predictive value, leading to the possibility of potentially postponing diagnostic thoracentesis in this situation until a trial of diuretic therapy has been performed. However, this strategy should be addressed in further prospective trials.
- Received September 28, 2005.
- Accepted January 31, 2006.
- © ERS Journals Ltd
References










