





Abstract
The aim of this study was to investigate the association between clinical variables and all-cause and respiratory mortality in patients with chronic obstructive pulmonary disease (COPD) undergoing long-term oxygen therapy (LTOT).
The authors retrospectively studied a historic cohort of 128 patients with COPD (126 males, mean age±sd 68.9±9.7 yrs, body mass index (BMI) 25.1±4.5 kg·m−2, and forced expiratory volume in one second 25.4±8.8% predicted), who were being treated with long-term oxygen therapy in a tertiary teaching hospital between 1992 and 1999. Comorbidity, assessed with the Charlson Index, was present in 38% of the patients. Vital status and cause of death were assessed through the population death registry.
A total of 78 patients (61%) had died by the end of follow-up. Three-year survival was 55%. Death was due to respiratory causes in 77% of cases. On Cox analysis, BMI <25 kg·m−2, comorbid conditions, age ≥70 yrs and cor pulmonale were associated with all-cause mortality. The BMI and comorbidity were the only significant predictive factors when the analysis was restricted to respiratory mortality.
In conclusion, body mass index <25 kg·m−2 and comorbidity were predictors of all-cause and respiratory mortality in a cohort of chronic obstructive pulmonary disease patients treated with long-term oxygen therapy. These factors should be taken into account when considering the management and prognosis of these patients.
Chronic obstructive pulmonary disease (COPD) is a common condition affecting 4–9% of the adult population 1, 2. In contrast to other diseases, COPD-related mortality has continued to increase in the general population 3.
COPD is a progressive disease that often leads to respiratory failure and death 2. Long-term oxygen therapy (LTOT) is the single treatment that has proven to be effective in increasing survival in COPD patients with chronic respiratory failure 4, 5. Nevertheless, the life expectancy in COPD patients receiving LTOT is poor, with a 5-yr survival rate of ∼40% 5, 6. Although it has been the subject of several studies, there is still some controversy regarding the risk factors associated with death in these patients. Respiratory function parameters (e.g. forced expiratory volume in one second (FEV1)), arterial blood gases (e.g. arterial oxygen tension (Pa,O2) and carbon dioxide arterial tension (Pa,CO2)), pulmonary hypertension, sex, age and body mass index (BMI), among others, are reported factors associated with mortality in these patients 6–13. However, none of these variables have achieved a clear predictive value in all of the studies in which they were examined. This discrepancy may be partly related to the heterogeneity of the methods used. In some studies, the inclusion criteria are not clearly stated; hence, other factors, such as the presence of associated lung diseases, may have influenced mortality 9. Moreover, variables such as comorbidity, which has been associated with mortality in patients with COPD 14–16, may not have been assessed in the subgroup with LTOT. Another aspect that may contribute to this discrepancy is the way in which the information on mortality was obtained. In some studies, no data are available regarding this point, and in others, the information source is the population death registry. In addition, most studies only consider overall mortality; respiratory mortality is included as an outcome measure in only one study 6.
The aim of the present study was to retrospectively analyse the variables associated with mortality in a historic cohort of COPD patients undergoing LTOT. The study design included careful selection of the patients in order to exclude those with associated pulmonary disease, and a comorbidity evaluation using a validated method 17. All-cause mortality and respiratory mortality were both considered primary outcome variables.
PATIENTS AND METHODS
Patients
All patients with COPD initiating LTOT >15 h·day−1 during 1992–1999 in the Oxygen Therapy Control Unit of a tertiary teaching hospital (Vall d'Hebron Hospital, Barcelona, Spain) with an urban catchment population of 450,000 inhabitants were considered for inclusion in the study. The patients were referred by their managing physicians. Patients were stable when LTOT was indicated and ≥3 months had passed since an acute exacerbation of the disease. Patients who were still active smokers were strongly advised to give up the habit.
The indication for LTOT was based on the criteria of the Spanish Society of Respiratory Diseases 18. Briefly, patients were selected for LTOT when room-air Pa,O2 was <7.3 kPa or 7.3–8.0 kPa and there were associated signs of cor pulmonale, polycythaemia or arrhythmia. The diagnosis of COPD was established by clinical assessment and pulmonary function testing (FEV1 <80% predicted and FEV1/forced vital capacity (FVC) ratio <70%). Patients with asthma or bronchiectasis were not included.
LTOT was withdrawn 3 months after initiation in patients whose blood gas results had improved (Pa,O2 >8 kPa) and in those who did not adhere to the treatment. Patients with any of the following factors were excluded from the study: 1) associated restrictive disorder (e.g. tuberculosis sequelae); 2) other clinically significant coexisting respiratory diseases (e.g. sleep apnoea/hypopnoea syndrome); 3) end-stage malignancies that might compromise short-term survival; or 4) inability to achieve Pa,O2 >8 kPa with oxygen administration. Patient selection is shown in figure 1⇓.
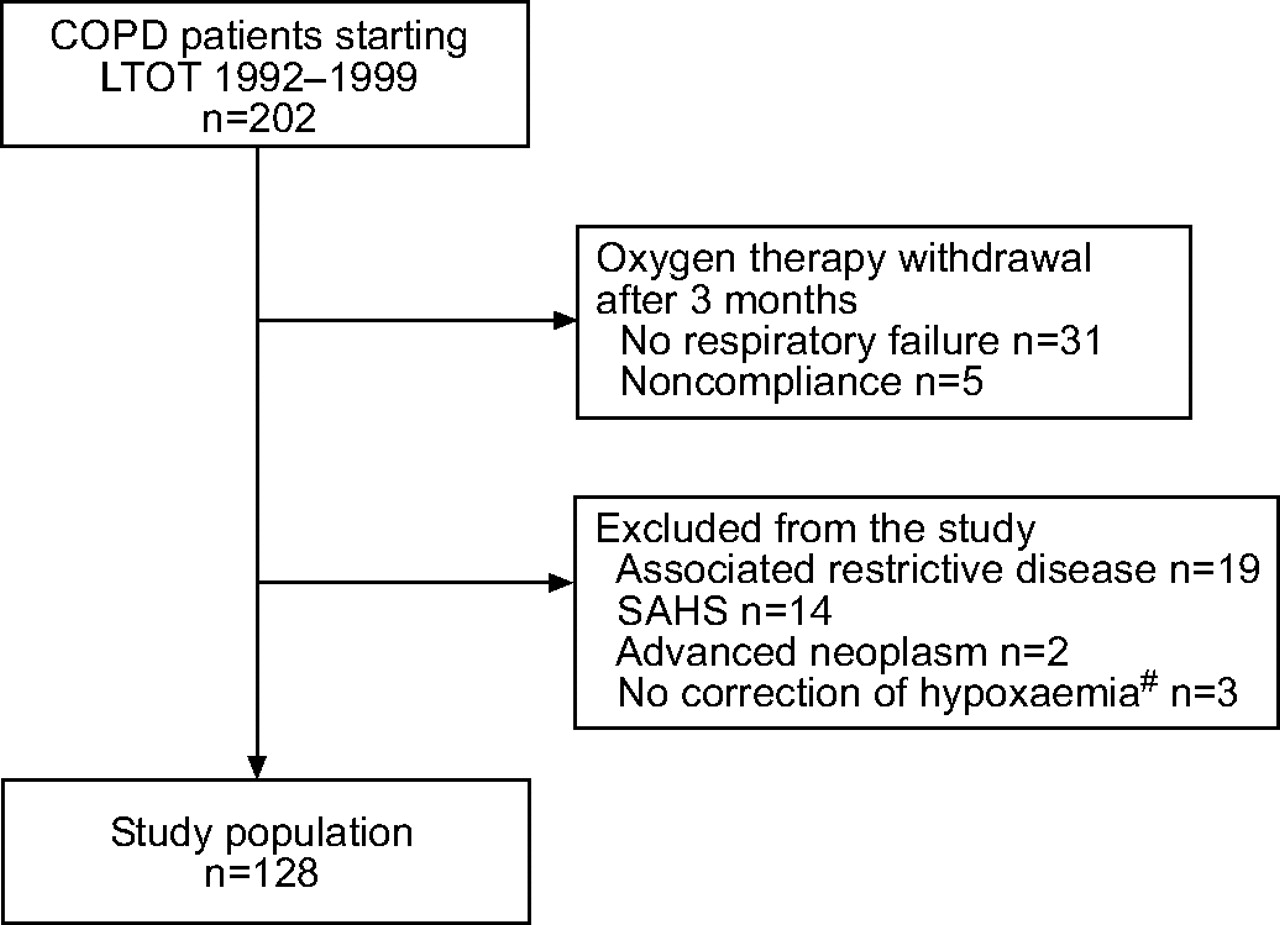
Chronic obstructive pulmonary disease (COPD) population included in the study. LTOT: long-term oxygen therapy; SAHS: sleep apnoea/hypopnoea syndrome. #: Two patients with concomitant pulmonary shunt and one patient with increasing hypercapnia precluding increased oxygen flow.
The study protocol was approved by the hospital ethics committee.
Baseline measurements and definitions
Baseline studies included history-taking and physical examination, electrocardiogram (ECG), chest radiograph, and spirometry study (Datospir 200; Sibel, Barcelona, Spain). The reference spirometry values were those reported by Roca et al. 19. Arterial blood gases were determined with a pH and blood gas analyser (IL-1306; Instrumentation Laboratories, Milan, Italy). Arterial blood gas testing was performed with the patient seated at rest and breathing room air, and again after 30 min of oxygen administration through nasal prongs, attempting to reach Pa,O2 values >8.6 kPa. Height and weight were measured and the BMI was calculated (weight in kg divided by height in m2).
Cor pulmonale was defined as the presence of two or more of the following criteria: 1) right ventricular hypertrophy or right atrial enlargement on the ECG; 2) enlarged pulmonary arteries on the chest radiograph; and 3) pedal oedema. Baseline comorbid conditions were recorded as a Charlson Index 17. This system, developed to predict the impact of comorbidity on prognosis in longitudinal studies, assigns each disease a score of 1 to 6, which is proportional to the disease-related risk of death. A score of 1 is allocated to myocardial infarction, congestive heart failure, peripheral vascular disease, cerebrovascular disease, dementia, connective tissue disease, ulcer disease, mild liver disease and diabetes. A score of 2 is assigned to diabetes with end-organ damage, hemiplegia, renal disease and malignancies, including leukaemia and lymphoma. A score of 3 is ascribed to moderate or severe liver disease, while AIDS and metastatic malignancies are attributed a score of 6. COPD was excluded from the list for the present study. The baseline characteristics were recorded systematically in a computer database.
Oxygen treatment
The prescription for oxygen treatment was >15 h·day−1, at a flow rate determined in the laboratory, usually 1–3 L·min−1. The oxygen supply was provided by an oxygen concentrator in most patients and by liquid oxygen in a few cases. The patients and their families were instructed in the use of the oxygen delivery system. The oxygen equipment was provided by the supplier, which also carried out technical servicing in the patient's home. All costs were covered by the National Health System, which provides the population with total medical coverage.
Follow-up
Patients were managed clinically by their referring physicians, who were unaware of the ongoing study. All patients were seen at least once a year in the oxygen therapy control unit in order to assess LTOT compliance and adapt oxygen flow, if necessary.
Patients were included in the study at the time that LTOT was indicated, and follow-up ended in December 2000. Data on the patient's vital status was obtained from the Catalan Death Registry, which provided the basic causes of death compiled from the death certificates and coded according to the 10th revision of the International Classification of Diseases (ICD)-10 20.
Statistical analysis
Assessment of baseline homogeneity between survivors and deceased patients was performed by means of the unpaired t-test for continuous variables, the Mann–Whitney test for ordinal variables and Fisher's exact test for qualitative variables. Results are expressed as mean±sd for quantitative variables, and as frequencies and percentages for qualitative and ordinal variables. The Kaplan–Meier method was used to estimate the survival function and the Cox proportional hazards model was used to perform the adjusted analysis 21.
The selection of independent variables for multivariate analysis was based on statistical significance obtained in the bivariate analysis (p<0.10) or on biological plausibility. A forward stepwise procedure was used and results are expressed as hazards ratio with 95% confidence intervals (CI). Data from cases receiving a treatment that could have modified the course of the disease were censored beyond that time point. Separate analyses were performed for all-cause mortality and respiratory mortality (ICD-10 codes J00–J99). BMI was stratified using standard categories (<20, 20–24.9, 25–29.9 and ≥30) and age was set at <70 or ≥70 yrs. Reference levels for categorical variables were selected according to the lowest risk (hazard ratio estimate) for mortality.
Statistical significance was set at a two-tailed p-value of ≤0.05 for all tests.
RESULTS
Clinical characteristics
From a total of 202 COPD patients initiating LTOT during 1992–1999, 128 were included in the study (fig. 1⇑). Characteristics of the total cohort at baseline, overall and according to vital status at the end of follow-up, are shown in table 1⇓. Most patients were male (98%), and ∼69 yrs old. Weight distribution was as follows: 15 (12%) were underweight (BMI <20), 50 (39%) were normal (BMI 20.0–24.9), 47 (36%) were overweight (BMI 25.0–29.9) and 16 (13%) were obese (BMI ≥30). The majority of patients (95%) were current or former smokers, and most had severe bronchial obstruction and mild hypercapnia (Pa,CO2 >6 kPa in 81 cases, 63%). Cardiovascular diseases and diabetes were the most frequent comorbid conditions (table 2⇓). Follow-up was performed by pulmonologists in 93 (73%) patients and by general practitioners in the remaining cases. Additional treatment administered for COPD is shown in table 3⇓.
Characteristics of 128 chronic obstructive pulmonary disease(COPD) patients on long-term oxygen therapy at baseline and by vital status at the end of follow-up
Chronic conditions at baseline according to the Charlson Index in 128 chronic obstructive pulmonary disease patients starting long-term oxygen therapy
Pharmacological treatment in 128 chronic obstructive pulmonary disease patients starting long-term domiciliary oxygen therapy
Follow-up and mortality
Patients were followed-up for a median of 3.2 yrs (interquartile range 1.1–6.9). In six survivors, follow-up ended before December 2000 because another treatment had been initiated: noninvasive mechanical ventilation in three patients, lung transplantation in two patients and surgery for pulmonary bullae in one patient. No patients were lost to follow-up.
By the end of follow-up, 78 patients (61%) had died. In the bivariate analysis, patients who died were older, had a lower BMI, and a higher frequency of cor pulmonale and comorbid conditions as compared to the survivors. The 1-, 3- and 5-yr survival rates were 0.79 (95% CI 0.72–0.86), 0.55 (0.46–0.64) and 0.34 (0.24–0.44), respectively (fig. 2⇓). The causes of death are shown in table 4⇓. Among the 78 deaths, 60 (77%) were due to respiratory causes.

Kaplan–Meier survival curve for all-cause mortality in 128 chronic obstructive pulmonary disease patients starting long-term oxygen therapy.
Causes of death
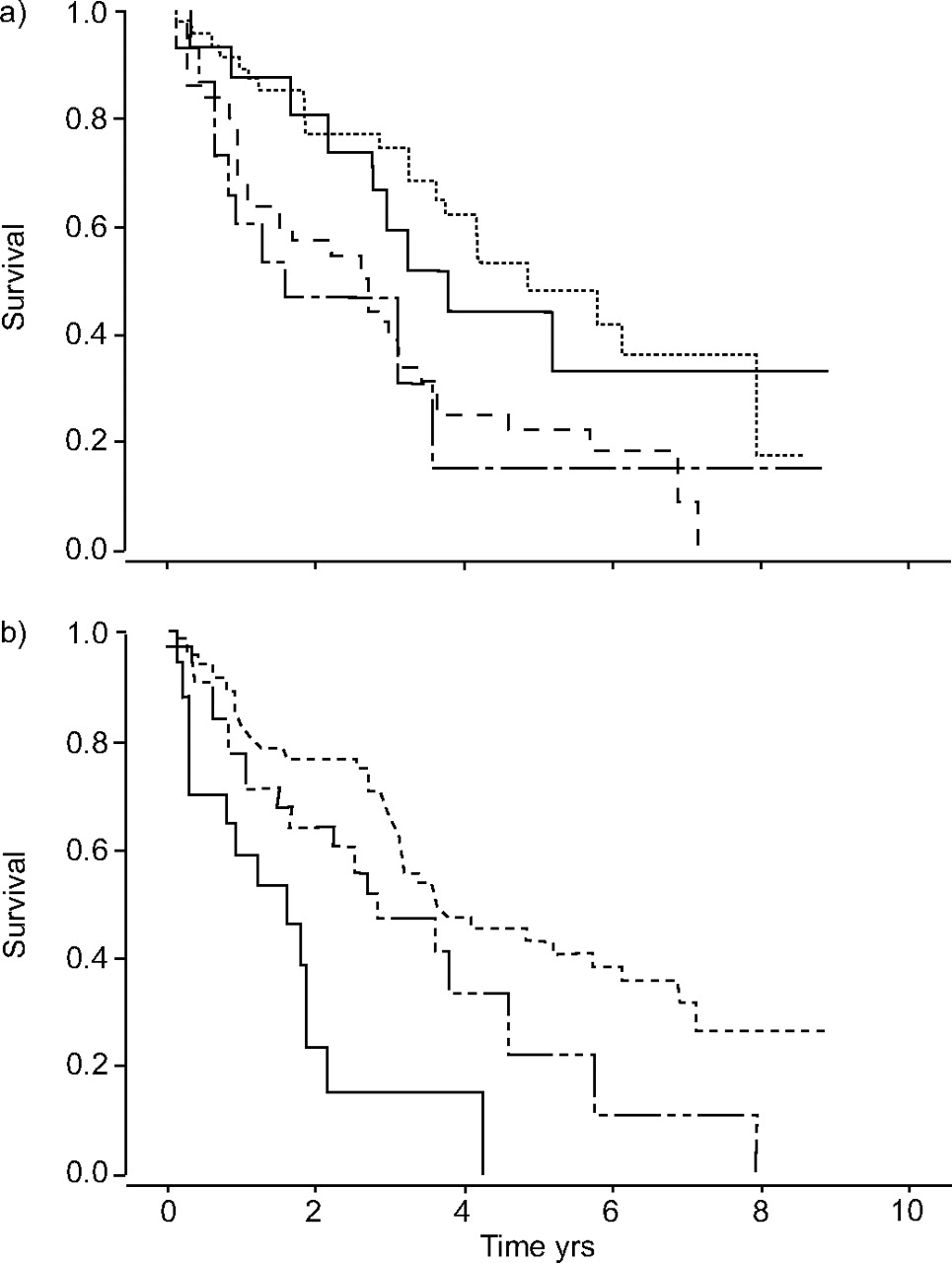
Multivariate Cox analysis included the following variables: age, sex, BMI, FEV1 (% pred), FVC (% pred), Pa,O2, Pa,CO2, cor pulmonale, oral corticosteroid therapy, comorbid conditions and COPD-related hospitalisation in the previous year. The independent predictive factors for overall mortality in these patients are presented in table 5⇓. Presence of cor pulmonale and age ≥70 yrs were associated with increased mortality. Another significant factor was the presence of comorbid conditions. The risk of death increased at least three-fold for a Charlson index ≥2, assuming the lower limit of the 95% CI as the minimum risk associated with the present data. The relationship between BMI categories and hazard ratio for mortality is shown in figure 3⇓. When BMI 25–29.9 was taken as the reference category, values <25 were associated with increased mortality (table 5⇓). Using a BMI of 20–24.9 as a reference, the relative hazard ratios were 1.73 (95% CI 0.81–3.67; p = 0.15), 0.33 (0.19–0.58; p<0.001) and 0.57 (0.26–1.24; p = 0.15) for BMI <20, 25–29.9 and ≥30, respectively. In the analysis of death exclusively by respiratory causes, only the BMI and comorbidity were significant predictive factors (table 5⇓). Kaplan–Meier survival curves for all-cause mortality according to BMI and comorbidity categories are shown in figure 4⇓.

All-cause mortality according to body mass index (BMI) in 128 chronic obstructive pulmonary disease patients starting long-term oxygen therapy. BMI 20–24.9 (•) and 25–29.9 (▪) kg·m−2 were used for reference. BMI: body mass index; HR: hazard ratio.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curves for all-cause mortality according to a) body mass index (BMI) and b) comorbidity (Charlson Index), in 128 chronic obstructive pulmonary disease patients starting long-term oxygen therapy. a)———: BMI ≥30 kg·m−2; --------: BMI 25–29 kg·m−2; – – – –: 20–24 kg·m−2; — - —: BMI <20 kg·m−2. b)- - - - - : Charlson Index 0; — -- —: Charlson Index 1; ———: Charlson Index ≥2.
Prognostic factors according to Cox models for all-cause and respiratory mortality
DISCUSSION
In this study, a BMI <25 kg·m−2 and the presence of comorbid conditions as assessed by the Charlson Index were predictive factors for all-cause and respiratory mortality in a cohort of COPD patients treated with LTOT.
A low BMI (<20) has been found in 20–30% of patients with advanced COPD 7, 22 and has proved to be a predictive factor for mortality in these patients regardless of pulmonary function status 22–25. The role of body weight as an indicator of mortality in the COPD population treated with LTOT was assessed in two prior studies, which showed discordant results. Whereas one reported an inverse relationship between BMI and mortality 7, the other showed no relationship between these factors in the adjusted analysis 9. The present results showed that the BMI category associated with the lowest risk of mortality was 25–29.9. Therefore, 25–29.9 was chosen as the reference category for analysing this factor, rather than 20–24.9, which is considered to represent the normal weight in the general population. On that basis, a higher risk of death was found not only in patients with BMI <20, but also in those with BMI 20–24.9. As is clearly seen figure 3⇑, the risk of death increases both above and below 25–29.9, regardless of the BMI taken as reference. These findings concur with results from other studies, which show a gradual increase in the risk of death as weight decreases in patients with COPD 7, 22–25. However, the fact that patients with a normal BMI were at a higher risk cannot be clearly explained. Schols et al. 26 described depletion of the fat-free mass in 9% of patients with COPD and a normal BMI. In fact, a measure of this fat-free mass, the mid-thigh muscle cross-sectional area assessed by computed tomography, has been shown to be a better predictor of mortality than BMI in patients with COPD 27. Furthermore, fat-free mass has recently been identified as an independent risk factor for mortality in COPD patients, regardless of the fat mass 28. Hence, protein depletion may be a negative feature in the prognosis of these patients, even though their weight is normal. This evidence may help to explain why 25–29.9 was the BMI category with the lowest associated risk of death. Thus, as has been shown in previous studies 7, 22–25, being overweight may have a positive effect on the prognosis in the COPD population.
The present results indicate that comorbidity as measured by the Charlson Index was associated with both all-cause and respiratory mortality. Prior studies have reported the Charlson Index to be a predictor of mortality in both medical 17 and surgical 29 patients. The Index has also been used in patients with COPD, but the results are not consistent; some authors have found an association with mortality 14–16, whereas others have not 30–33. This discrepancy may be due to methodological differences among the studies, particularly with regard to heterogeneity among the populations included, and the phase, exacerbated or stable, in which the disease was studied. The present study is the first to measure comorbidity as a risk factor for mortality in COPD patients receiving LTOT. In keeping with previous studies, COPD was excluded as a variable when calculating the Index 15. The association between comorbidity and all-cause mortality suggests that comorbidity may have exerted some influence on the non-respiratory causes of death. Nevertheless, the majority of the patients died of respiratory causes (77%) and comorbidity also proved to be a factor associated with respiratory death. As has been suggested 30, comorbidity may have an influence on the severity of the acute respiratory complications that determine death in these patients. Moreover, comorbid conditions might trigger events that would increase the frequency of exacerbations, such as pulmonary thromboembolism or vertebral fractures.
Among the variables that reflect the severity of COPD, only cor pulmonale was associated with all-cause mortality in the present study. However, the authors recognise that they used clinical criteria to define cor pulmonale, a fact that could limit the reliability of this finding. Cor pulmonale is a known factor of poor prognosis in COPD patients 34, 35, but the impact of this condition on those receiving LTOT is uncertain. In most studies, cor pulmonale was not included as a variable to be analysed. Another factor that is highly related to cor pulmonale, pulmonary hypertension as measured by cardiac catheterisation, was associated with mortality in another cohort of COPD patients undergoing LTOT 11. Pulmonary function and blood gas variables showed no association with mortality in the present patients. In previous studies, the results relative to this point are not concordant. FEV1, Pa,O2 and Pa,CO2 have shown associations in some studies 7, 9, 12 but not others 10, 11. Once again, these differences may partly be due to dissimilar characteristics of the patients studied. In addition, with regard to hypoxaemia, it is likely that initiation of LTOT as corrective therapy would cancel out the effect of this unfavourable prognostic factor.
Some potential limitations of the present study deserve comment. First, the lengthy period of inclusion and follow-up, which is necessary in a cohort study, can imply a series of changes in the diagnostic and therapeutic procedures used that might affect the results. However, during the study period, no substantial changes were incorporated into the management of these patients. In fact, Cox analysis in patients recruited in the early years of the study (1992–1995) versus those recruited later (1996–1999), showed no significant differences with regard to the factors predicting mortality (results not shown). Secondly, the cohort studied contains very few females. This can probably be attributed to the relatively late initiation of the habit of smoking among females in Spain 1. As a result and taking into account the fact that differences in mortality have been related to sex in patients with LTOT 5, 6, the present results cannot be generalised to the female COPD population. Another potential limitation centres on the validity of death certificates as the basis for determining the cause of death. Some authors have suggested that there is a tendency to underestimate COPD when multiple causes of death are not taken into account 36, 37. Despite this, in the present COPD was cited as the cause of death in 65% of the certificates and other respiratory diseases were cited in 12%. In keeping with the study by Zielinski et al. 38, who examined causes of death in 215 patients on LTOT in seven European countries, the majority of patients with advanced COPD undergoing this treatment died due to respiratory causes. Therefore, the present authors do not believe that underestimation of COPD as the cause of death has substantially affected the study's results.
In conclusion, the present findings suggest that among chronic obstructive pulmonary disease patients receiving long-term oxygen therapy, non-respiratory variables, such as body mass index <25 kg·m−2 and associated comorbid conditions, are highly relevant factors in both all-cause and respiratory mortality. This suggests that a multidisciplinary approach, which includes nutritional support and appropriate management of the comorbid processes, may be preferable in these patients.
Acknowledgments
The authors would like to thank: T. Codinachs for nursing assistance: the Registre de Mortalitat de Catalunya (Servei d'Informació i Estudis, Direcció General de Recursos Sanitaris, Departament de Sanitat i Seguretat Social, Barcelona, Spain) for providing mortality data; the Laboratori de Bioestadística i Epidemiologia (Universitat Autonoma de Barcelona, Barcelona, Spain) for advice on statistical analysis; and C. Cavallo for English translation.
- Received June 30, 2005.
- Accepted December 12, 2005.
- © ERS Journals Ltd
References









