





Abstract
Baroreflex control of heart rate during sleep (baroreflex sensitivity; BRS) has been shown to be depressed in obstructive sleep apnoea (OSA), and improved after treatment with continuous positive airway pressure (CPAP). Whether CPAP also acutely affects BRS during sleep in uncomplicated severe OSA is still debatable.
Blood pressure was monitored during nocturnal polysomnography in 18 patients at baseline and during first-time CPAP application. Spontaneous BRS was analysed by the sequence method, and estimated as the mean sequence slope.
CPAP did not acutely affect mean blood pressure or heart rate but decreased cardiovascular variability during sleep. Mean BRS increased slightly during CPAP application (from 6.5±2.4 to 7.5±2.9 ms·mmHg−1), mostly in response to decreasing blood pressure. The change in BRS did not correlate with changes in arterial oxygen saturation or apnoea/hypopnoea index.
The small change in baroreflex control of heart rate during sleep at first application of continuous positive airway pressure in severe obstructive sleep apnoea was unrelated to the acute resolution of nocturnal hypoxaemia, and might reflect autonomic adjustments to positive intrathoracic pressure, and/or improved sleep architecture. The small increase in baroreflex control of heart rate during sleep may be of clinical relevance as it was accompanied by reduced cardiovascular variability, which is acknowledged as an independent cardiovascular risk factor.
Severe obstructive sleep apnoea (OSA) is a known cause of autonomic dysfunction 1–6 and increased cardiovascular risk and mortality 7, 8. Long-term treatment with continuous positive airway pressure (CPAP) is effective in counteracting the detrimental effects of OSA on the cardiovascular system. In addition, baroreflex control of heart rate was found to increase 1, 4, 5 sympathetic and hyperactivity decreased 9, 10, after prolonged CPAP treatment.
All studies of the effects of acute CPAP application in OSA patients agree that preventing apnoeas by effective CPAP decreases cardiovascular variability 9–13. Conversely, the effects of acute CPAP on systemic arterial blood pressure (BP) levels are still controversial 9–13, and may be more readily apparent in hypertensive subjects 14. Little is known about the effects of first CPAP application on baroreflex function in previously untreated patients with uncomplicated OSA. Acute CPAP application in normal awake subjects breathing at 12 or 15 breaths·min−1 caused bradycardia, and increased BP and the high-frequency component of the alpha index (a measure of the sensitivity of baroreflex cardiac modulation in the frequency domain) of baroreflex gain 15. Conversely, in patients with OSA and chronic heart failure (CHF), CPAP application during sleep increased spontaneous baroreflex control of heart rate (baroreflex sensitivity; BRS) but decreased BP in nonrapid eye movement (NREM) stage 2 sleep 16. Acute CPAP also improved BRS and decreased BP in patients with OSA and refractory hypertension 14. Finally, short-term (7–10 days) CPAP treatment increased BRS during NREM sleep in nonapnoeic snorers to levels found in nonsnorer controls 17.
To the current authors' knowledge, no study has assessed the effects of acute CPAP application on baroreflex control of heart rate during sleep in patients with severe uncomplicated OSA. The aim of the present study was to fill this gap. Specifically, the relationship between CPAP-induced acute correction of nocturnal intermittent hypoxaemia and changes in baroreflex control of heart rate was investigated. Based on the direct relationship between mean lowest arterial oxygen saturation (Sa,O2) during NREM sleep and BRS previously shown in untreated severe OSA 1, the current authors hypothesised that resolution of nocturnal intermittent hypoxaemia by CPAP might acutely improve baroreflex control of heart rate, as already demonstrated in the case of chronic treatment.
PATIENTS AND METHODS
Subjects
The study was conducted in 18 male patients with severe OSA (table 1⇓). Inclusion criteria were: normal daytime BP (<120/80 mmHg) or mild untreated hypertension (<145/95 mmHg) at repeated office BP measurements; no evidence of heart failure or other disease causing autonomic dysfunction; no treatment with cardiovascular drugs; and normal pulmonary function. Alcohol and caffeine intake were <30 g·day−1, and 2–4 cups·day−1, respectively. Ten patients were current smokers (cigarettes·day−1: <20: n = 8; ≥20: n = 2). All subjects refrained from caffeine, alcohol and smoking on the days of the study.
Anthropometric and sleep data
Patients were studied at baseline and during CPAP titration. CPAP studies were performed 18±9 days after baseline study (range 1–30 days). During this interval, no patient received any treatment, or changed weight or smoking habits. CPAP was titrated manually. From the nasal mask, the pressure applied was continuously measured by a pressure transducer while flow was sampled and integrated by a pneumotachograph to detect apnoeas, hypopnoeas and inspiratory flow limitation. The CPAP level was considered appropriate when respiratory events, including flow limitation episodes, were abolished in all sleep stages in the supine position. The data analysed were obtained after an effective CPAP level was attained. Subjects gave their informed consent, and the study protocol was approved by the local ethical committee.
Measurements and data analysis
The protocol of night studies has been reported previously 1. During full nocturnal polysomnography (Somnostar 4100; SensorMedics Corporation, Yorba Linda, CA, USA), arterial BP was noninvasively monitored on a beat-by-beat basis (Finapres 2300, autocalibration mode; Ohmeda, Englewood, CO, USA). Finger-cuff inflation was stopped for 5 min every 40 min to prevent finger discomfort during the recording. The hand equipped with the Finapres cuff was held in a constant position at heart level.
Sleep was scored in 30-s epochs 18. Epochs of NREM stages 1 and 3–4, and epochs without BP recording (periodic interruption, Finapres calibration, or BP artefacts) were not analysed.
Apnoea was defined as an interruption of airflow ≥10 s, and scored as obstructive or central according to persistence or absence of thoraco-abdominal movements, respectively. Hypopnoea was defined as a decrease in airflow ≥50%, associated with arousal and/or decreased Sa,O2 ≥4%. Apnoea/hypopnoea index (AHI), mean Sa,O2 during wakefulness, and mean lowest Sa,O2 in NREM stage 2 and REM sleep were calculated.
Cardiovascular variables were analysed by considering 2-min segments showing a stable polysomnographic stage 18 and good quality BP signal for ≥85% of their duration 1. Analysed sleep segments showed recurrent apnoeas at baseline, and regular unobstructed breathing during CPAP as indirectly confirmed by the absence of snoring and of pulsus paradoxus on the BP signal. Mean systolic (S) and diastolic (D) BP and pulse interval (PI), and their standard deviations (sd) taken as estimates of variability, were calculated during nocturnal wakefulness, NREM stage 2 and REM sleep.
Baroreflex function was analysed according to the sequence method described in detail elsewhere 1, 2, 19–22. Spontaneous sequences of three or more consecutive beats in which PI and SBP progressively increased (+PI/+SBP, up sequences) or decreased (−PI/−SBP, down sequences) were identified. BRS was assessed as the slope of the regression line between PI and SBP values within each sequence. Mean BRS, the number of sequences per hour (sequence index), and mean SBP and PI at beginning and end of sequences were calculated in each stage.
Statistics
Data are reported as mean±sd. Unpaired t-test was used to compare variables between smoking and nonsmoking OSA patients. Paired t-test was used to compare variables recorded under no treatment and under CPAP, separately for the considered sleep stages. Differences among sleep stages in each condition were tested by ANOVA with Bonferroni's correction. Relationships between variables were analysed by linear regression. Statistical significance was set at p<0.05.
RESULTS
Demographic and sleep data
The patients studied were on average middle-aged, obese, and most (n = 11) showed slightly increased BP values during wakefulness (table 1⇑). Their OSA was severe, as indicated by an AHI ranging between 58 and 143 events·h−1 and low Sa,O2 values during sleep. Pulmonary function tests during daytime were in the normal range (group means for forced expiratory volume in one second and forced vital capacity were 102.0±17.5% and 104.1±17.8% of predicted values, respectively), and mean Pa,O2 and Pa,CO2 were 10.9±1.3 and 5.57±0.4 kPa, respectively.
Mean age, body mass index (BMI), spirometry, AHI or sleep stage distribution did not differ between smoking and nonsmoking patients. Mean Pa,O2 during wakefulness was lower in smokers (9.92±0.69 kPa) than in nonsmokers (1.58±0.2 kPa, p<0.005). Diastolic BP during wakefulness was significantly higher, while mean Sa,O2 during NREM sleep was significantly lower in smokers than in nonsmokers (table 1⇑).
The level of CPAP applied during the study was 11.2±3.0 cmH2O. CPAP prevented obstructive events and normalised Sa,O2 during sleep in all patients independent of their smoking status. Compared with the baseline study, the amount of stage 2 NREM sleep decreased, and that of REM sleep increased during CPAP application. NREM stage 3–4 sleep was recorded for very short periods in seven OSA patients at baseline, and in 12 patients during CPAP application, preventing satisfactory analysis of BRS in this sleep stage.
Blood pressure and pulse interval
The average number of 2-min segments analysed under no treatment and during CPAP application, respectively, were: 10±7 and 21±11 for nocturnal wakefulness, 65±21 and 36±16 for NREM stage 2 sleep, 11±7 and 15±16 for REM sleep. Mean SBP tended to decrease during CPAP application, while DBP and PI did not differ between studies in any sleep stage (table 2⇓). The variability of SBP, DBP and PI during sleep, estimated as their sd, decreased markedly during CPAP (table 2⇓).
Mean systolic and diastolic blood pressure(SBP and DBP) and pulse interval (PI), and their variability (standard deviation) in the entire group (n = 18)
SBP and DBP values during sleep were similar in smokers and nonsmokers under no treatment and during CPAP application. Instead, cardiovascular variability during wakefulness and sleep was significantly higher in smokers compared with nonsmoker OSA patients under no treatment; this difference disappeared during CPAP application. For example, sd of SBP during the entire polysomnographic study under no treatment was 15.3±4.2 mmHg in smokers and 12.2±2.7 mmHg in nonsmokers (p<0.01). Corresponding values during CPAP were 6.1±1.5 and 6.5±1.4 mmHg (nonsignificant). DBP and PI variability were also increased in smoking OSA patients under no treatment only (not shown).
Baroreflex sensitivity
In the baseline night, mean BRS during wakefulness was lower in smokers compared with nonsmokers (smokers: 4.8±1.9 ms·mmHg−1; nonsmokers: 7.2±1.2 ms·mmHg−1, p<0.01). Differences in BRS during sleep did not reach significance (NREM stage 2: smokers 5.4±2.3 ms·mmHg−1, nonsmokers 7.2±1.3 ms·mmHg−1, p = 0.07; REM: smokers 7.9±3.0 ms·mmHg−1, nonsmokers 7.4±2.7 ms·mmHg−1, nonsignificant). During CPAP application, mean BRS increased from 6.5±2.4 to 7.5±2.9 ms·mmHg−1 (p<0.05), without differences between normotensive and slightly hypertensive patients or according to smoking status (not shown).
When sequences characterised by baroreflex activation (+PI/+SBP) and deactivation (−PI/−SBP) were analysed separately (fig. 1⇓ and 2⇓), OSA patients under no treatment showed a higher mean sequence slope in +PI/+SBP than in −PI/−SBP sequences (7.9±4.5 versus 5.9±2.6 ms·mmHg−1, p<0.01). Acute CPAP application increased only the slope of −PI/−SBP sequences without differences according to the smoking status (fig. 1⇓ and 2⇓). The number of sequences per hour was unaffected by CPAP (figure 3⇓).

Individual (○: nonsmokers; •: smokers) and mean (outermost symbols±sd) spontaneous baroreflex control of heart rate (BRS) for the analysed recordings obtained under no treatment and during acute continuous positive airway pressure (CPAP) application. a) shows baroreflex activation sequences; and b) shows baroreflex deactivation. #: significant difference compared with baseline.

Spontaneous baroreflex control of heart rate (BRS) in obstructive sleep apnoea patients at different sleep stages (nocturnal wakefulness, nonrapid eye movement (NREM) and rapid eye movement (REM)). Continuous positive airway pressure (CPAP) application did not modify BRS in +PI/+SBP sequences (a), but increased BRS slightly in −PI/−SBP sequences (b). Statistical analysis was by paired t-test in each sleep stage. □: under no treatment; ░: during acute application of CPAP; ▒: control subjects (data from 1).
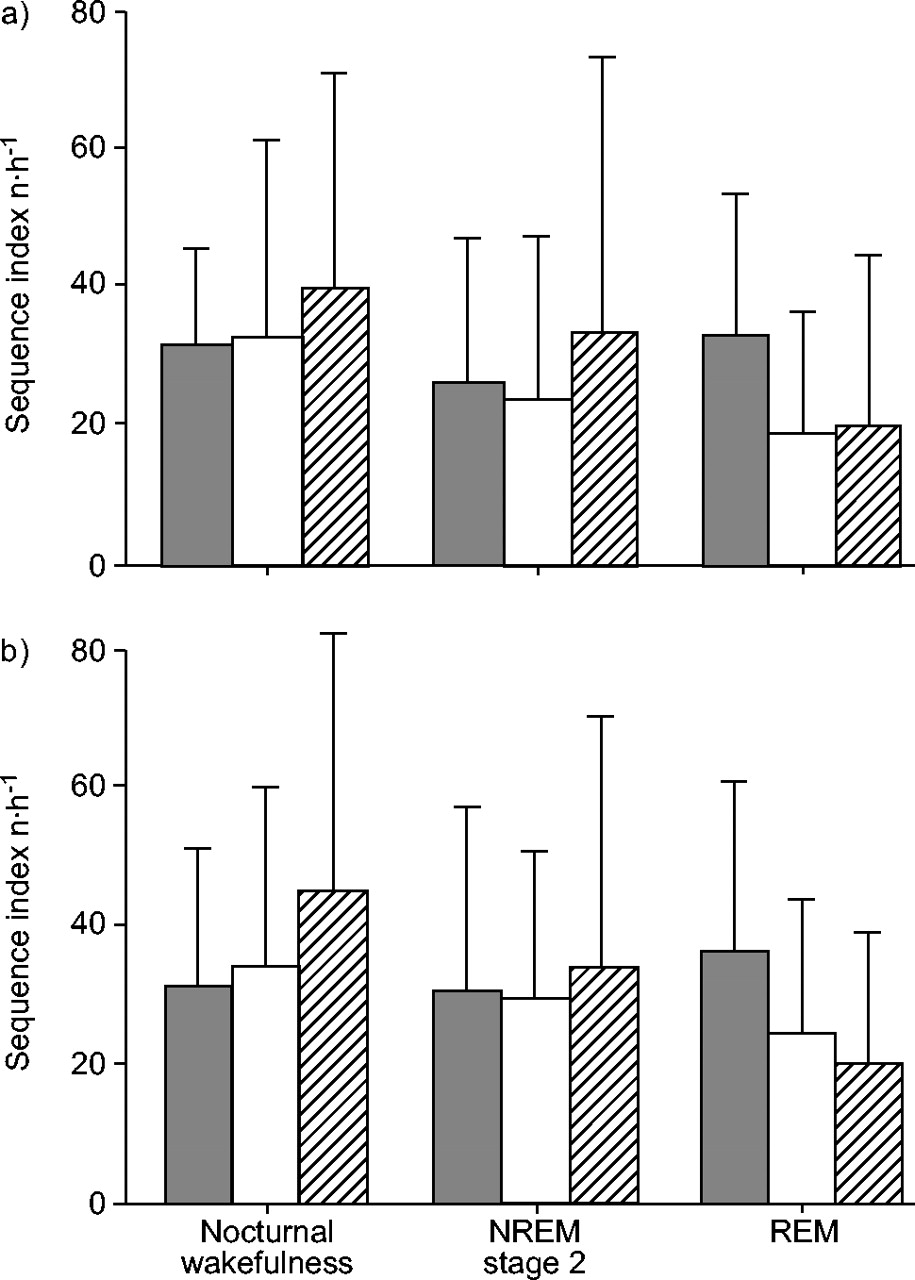
Sequence index (number of sequences·h−1) in obstructive sleep apnoea (OSA) patients at different sleep stages (nocturnal wakefulness, nonrapid eye movement (NREM) and rapid eye movement (REM)). All comparisons between baseline and acute continuous positive airway pressure (CPAP) application conditions were not significant. □: under no treatment; ░: during acute application of CPAP; ▒: control subjects (data from 1).
The mean range of SBP changes during baroreflex sequences (table 3⇓) decreased from the baseline night (+PI/+SBP: 14.7±2.6 mmHg; −PI/−SBP: 17.3±4.8 mmHg) to the CPAP night (+PI/+SBP: 11.4±3.1 mmHg; −PI/−SBP: 10.5±4.1 mmHg, p<0.0001 for both comparisons), especially in smoker OSA patients who showed a high cardiovascular variability under no treatment. Mean PI at the beginning of +PI/+SBP sequences increased significantly during wakefulness and NREM stage 2 sleep (table 3⇓).
Initial systolic blood pressure(SBPi) and pulse interval (PIi) at the beginning of sequences and their changes during sequences (ΔSBP, ΔPI) during wakefulness and sleep under no treatment and during acute application of continuous positive airway pressure (CPAP)
Although average PI values during sleep did not differ significantly between studies (table 2⇑), the changes in BRS from baseline to CPAP application were positively correlated with development of bradycardia during NREM stage 2 sleep assessed as the change in mean PI (+PI/+SBP sequences: r = 0.70, p<0.005; −PI/−SBP sequences: r = 0.78, p = 0.001). Instead, no correlation was found between the change in BRS and baseline AHI or the change in mean lowest Sa,O2 during sleep on CPAP (fig. 4⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in mean baroreflex sensitivity (BRS) during continuous positive airway pressure application versus changes in arterial oxygen saturation (ΔSa,O2) during sleep (a) and baseline apnoea/hypopnoea index (b). All correlations were not significant (r2: 0.055 and 0.003 for Sa,O2; 0.013 and 0.039 for apnoea/hypopnoea index, in nonrapid eye movement (•) and rapid eye movement sleep (▪), respectively).
DISCUSSION
The main result of the current study shows that in patients with uncomplicated severe OSA, acute application of CPAP during sleep prevented apnoeas and intermittent hypoxaemia, induced a significant and marked reduction in cardiovascular variability, and was responsible for a small but significant improvement in baroreflex control of heart rate, mostly in response to baroreceptor deactivation (down sequences). This improvement in BRS was smaller than BRS changes observed after prolonged CPAP treatment 1 and did not correlate with the increase in Sa,O2 during sleep. Therefore, the current authors' hypothesis that acute correction of nocturnal intermittent hypoxaemia might be associated with an acute improvement of BRS in patients with severe uncomplicated OSA was only partly confirmed. Full recovery of reflex cardiac modulation in severe OSA patients undergoing CPAP ventilation during sleep might require prolonged regular treatment.
However, other aspects of the current study deserve to be discussed. First, about half of our subjects were smokers, and this may have affected the results, as smoking is known to decrease BRS 23–25. Smokers and nonsmokers were comparable for anthropometric variables and AHI, but smokers were slightly hypoxaemic during wakefulness and showed a lower Sa,O2 during sleep, lower BRS values during wakefulness, and a larger cardiovascular variability under no treatment conditions. This is in line with previous data on the cardiovascular effects of cigarette smoking, which appear to characterise only the actual smoking period during the daytime and fade away 15–20 min after the last cigarette and in the absence of smoking during night-time sleep 26, 27. In fact, the effects of CPAP application did not differ between smoking and nonsmoking OSA patients, and the two groups no longer differed during CPAP application. However, further studies are necessary to explore this point given the strong impact of both smoking and OSA on cardiovascular risk 8.
Secondly, the acute application of CPAP did not affect mean BP and PI values, which is in line with previous observations 9–13. However, at variance with previous studies including hypertensive patients, in the current study only normotensive and mildly hypertensive untreated patients were recruited. The results therefore support the notion that CPAP may decrease BP mostly in patients with sleep-disordered breathing associated with a frank hypertensive condition 9, 14, 28. On the other hand, in line with previous studies 2, the data provide clear evidence that acute CPAP blunts the increase in cardiovascular variability from wakefulness to sleep typical of untreated OSA 1. This finding was also evident when focusing on the beat-by-beat SBP changes (SBP ramps), characterising spontaneous baroreflex sequences, since the range of SBP fluctuations during either up or down sequences, respectively leading to baroreceptor activation or deactivation, was clearly reduced during CPAP application.
The similar BP levels observed during the baseline and CPAP nights might depend on different pathophysiological mechanisms. The current authors speculate that under no treatment, BP mostly reflected OSA-associated cardiovascular perturbations 1; however, during CPAP application peripheral vasoconstriction evoked by reflex reaction to positive intrathoracic pressure may predominate 29–31. This interpretation is supported by the evidence that application of low levels of positive pressure ventilation in normal awake subjects increased diastolic BP 15. Similarly, baroreceptor-mediated adjustments were shown to occur in response to increased intrathoracic pressure 29, 30. Finally, in normal awake humans, CPAP at 10–12 cmH2O decreased central blood volume and redistributed cardiac output without affecting arterial BP or heart rate; however, calf resistance increased, indicating active autonomic adjustments on peripheral circulation 31. Thus, similar autonomic adjustments may have occurred in the normotensive or marginally hypertensive OSA patients in response to CPAP, and might have accounted for the apparent paradox of little or no change in BP despite normalisation of respiration, reduction in cardiovascular variability 1, 2 and reduction in muscle sympathetic nerve activity 10 already occurring at the time of the first CPAP application during sleep.
In the normotensive and marginally hypertensive subjects, an increase in BRS during CPAP application was found without associated changes in BP or heart rate, at variance with the data obtained in subjects with OSA combined with refractory hypertension 14, or in patients with OSA and CHF 16. Differences in methods may partly explain these different results, as the data were obtained at first CPAP application, whereas hypertensive and CHF patients were studied after one or more treatment nights. Moreover, the larger effects recorded in patients with CHF and OSA may be due to positive haemodynamic changes exerted by CPAP in this context 32–35 besides the prevention of upper airway obstruction.
A third issue to be addressed is the finding that the significant albeit small increase in BRS during acute CPAP application was associated with decreased heart rate, suggesting improved parasympathetic and reduced sympathetic cardiac modulation. Fietze et al. 15 found that both the high frequency component of heart rate variability (commonly regarded as an indirect marker of parasympathetic cardiac modulation) and the so called “alpha index” (another measure of the sensitivity of baroreflex cardiac modulation in the frequency domain 36) increased in normal awake subjects during positive pressure ventilation at 0.05 Pa. The small increase in BRS observed in the uncomplicated OSA patients is in line with these observations.
In this context, however, it should be emphasised that only the response to baroreflex deactivation (−PI/−SBP sequences) improved during CPAP application. This indicates an asymmetry in the acute improvement of BRS associated with first night CPAP application, characterised by a more prompt recovery of the reflex response to baroreceptor deactivation than to baroreceptor activation. Such a finding is not entirely surprising, as an asymmetry characterising the sensitivity of baroreflex heart rate modulation was also observed in other clinical conditions 37. The observations during sleep appear to be in line with the selective impairment of baroreflex response to hypotensive agents found in untreated OSA during wakefulness 38. Overall, the current study confirms that long-term CPAP treatment is necessary to reverse chronic autonomic dysfunction during sleep 1, 4, 5, 8 and wakefulness 6, 8, 39, 40, possibly in relation to recovery of cardiac vagal fibres after protracted resolution of intermittent hypoxia 41. Thus, the autonomic dysfunction associated with severe OSA appears not to be as readily reversible as the decreased BRS in snorers 17.
Moreover, the finding that the increase in BRS did not correlate with the improvement in nocturnal Sa,O2 during CPAP application may also suggest that the improvement of gas exchange during CPAP and the improvement of autonomic cardiac modulation are characterised by different time constants.
Among other factors involved in the complex autonomic cardiovascular modulation in OSA, it cannot be excluded that improved sleep architecture could contribute to an increase in parasympathetic cardiac regulation. Indeed, this study confirms a partial recovery of deep sleep at first CPAP application 42. More importantly, differences in the level and/or pattern of change in intrathoracic pressure between baseline and CPAP nights may also play some role in this setting. There is evidence that respiratory efforts can affect nocturnal BP 43. Moreover, the overall output of aortic (intrathoracic) and carotid (extrathoracic) baroreceptors appears to be modulated by their exposure to different transmural pressures 44. Unfortunately, this issue could only be resolved by studies in experimental animals, which would be desirable to obtain a deeper insight into such a complex topic.
Finally, this study included only a relatively small number of patients, due to the focus on uncomplicated and untreated OSA patients. The observations therefore need to be further confirmed by future studies on a larger sample of subjects.
In conclusion, in previously untreated patients with uncomplicated severe obstructive sleep apnoea, acute continuous positive airway pressure application was associated with a significant, although mild, improvement of the baroreflex control of heart rate, without any clear relationship with the improvement in nocturnal arterial oxygen saturation or apnoea/hypopnoea index. The data suggest a possible role of either central neural influences or mechanical changes in obstructive sleep apnoea-dependent autonomic modulation during continuous positive airway pressure application in explaining such an improvement. They also indicate that improvement of reflex cardiac regulation has a longer time constant than the treatment-related improvement in respiratory parameters, and that acute application of continuous positive airway pressure is not sufficient to fully revert obstructive sleep apnoea-induced baroreflex dysfunction, for which prolonged and regular treatment appears to be necessary 1.
- Received April 13, 2004.
- Accepted September 28, 2005.
- © ERS Journals Ltd
References










