





Abstract
Pulmonary veno-occlusive disease (PVOD) is a rare cause of pulmonary arterial hypertension that affects predominantly post-capillary pulmonary vessels. A major concern with PVOD is the poor response to available therapies and the risk of pulmonary oedema with continuous intravenous epoprostenol.
The present authors hypothesised that alveolar haemorrhage may be a characteristic feature of pulmonary veno-occlusive disease, as compared with other forms of pulmonary arterial hypertension that predominantly involve pre-capillary pulmonary arteries.
This paper reports a series of 19 patients with either PVOD (n = 8) or idiopathic pulmonary arterial hypertension (IPAH; n = 11) who underwent bronchoalveolar lavage. Cytological analyses were performed and differential counts were made on Perls-stained preparations. The Golde score was used to assess alveolar haemorrhage. As compared with IPAH, PVOD was characterised by a higher percentage of haemosiderin-laden macrophages (40±37 versus 3±6%), resulting in elevated Golde scores (81±88 versus 4±10).
It was concluded that occult alveolar haemorrhage is a common feature of pulmonary veno-occlusive disease. Detecting occult alveolar haemorrhage may be of interest in the diagnostic approach of pulmonary veno-occlusive disease.
- Alveolar haemorrhage
- bronchoalveolar lavage
- pulmonary arterial hypertension
- pulmonary veno-occlusive disease
Idiopathic pulmonary arterial hypertension (IPAH) is a disease of the small pulmonary arteries that leads to progressive increase in pulmonary vascular resistance, ultimately causing right ventricular failure and death 1, 2. Pulmonary veno-occlusive disease (PVOD) is an uncommon cause of pulmonary arterial hypertension that affects predominantly post-capillary pulmonary vessels 3–6. The pathological hallmark of PVOD is the extensive and diffuse occlusion of pulmonary veins by fibrous tissue 3–6. Intimal thickening involves venules and small veins in lobular septa and, rarely, larger veins 3–6. Clinically, patients suffering from PVOD frequently present in a similar fashion to other forms of pulmonary arterial hypertension, and PVOD accounts for 5–10% of histological forms of cases initially thought to be “idiopathic” 7.
One of the main concerns with PVOD is the poor response to available therapies and the risk of pulmonary oedema with continuous intravenous epoprostenol 8, 9. It is well accepted that a definite diagnosis of PVOD requires histological analysis of a lung sample 6. However, surgical lung biopsy is too invasive for these frail patients, emphasising the importance of developing less invasive tools to obtain the diagnosis 10. The current authors, along with others, have previously shown that the diagnosis of PVOD could be suspected by analysis of clinical and radiological information, including high-resolution computed tomography (HRCT) of the chest showing a characteristic pattern combining centrilobular ground-glass opacities, septal lines and lymph nodes enlargement 11–13.
As PVOD affects the post-capillary vasculature, it may be responsible for elevated pulmonary capillary pressure and, by inference, occult alveolar haemorrhage. It was, therefore, hypothesised that alveolar haemorrhage may be a characteristic feature of PVOD, as compared with other forms of pulmonary arterial hypertension, such as IPAH affecting predominantly pre-capillary pulmonary arteries. The aim of this study was to evaluate whether occult alveolar haemorrhage was a characteristic feature of PVOD, as compared with IPAH.
METHODS
Patients
A total of 19 cases of “primary” pulmonary arterial hypertension, referred to Hôpital Antoine Béclère (Clamart, France) between January 1997 and May 2001, and in whom a bronchoalveolar lavage (BAL) had been performed, were retrospectively studied. Inclusion criteria were a mean pulmonary artery pressure >3.325 kPa (25 mmHg) and a pulmonary arterial wedge pressure (PAWP) <1.995 kPa (15 mmHg). Causes of pulmonary hypertension such as chronic thrombo-embolic disease, chronic obstructive or restrictive lung diseases, left-heart disease, congenital heart disease, connective tissue disorders, portal hypertension and human immunodeficiency virus infection were excluded at the time of diagnosis 14. Pulmonary function tests, arterial blood gases, carbon monoxide diffusion capacity, HRCT of the chest, right-heart catheterisation, and acute vasodilator challenge were performed in all cases 12, 15. In the study period, all patients with a histological confirmation of PVOD in whom BAL data were available (n = 8) were included. Pathological confirmation of PVOD was obtained by means of post mortem (n = 4), explanted lungs (n = 2), or open lung biopsies (n = 2). All IPAH patients in whom a BAL had been performed during the study period were also included (n = 11). The diagnosis of IPAH was established according to published guidelines on the basis of clinical, biological and haemodynamical analysis. In addition, this diagnosis was further supported by the absence of radiological abnormalities suggestive of PVOD (i.e. the absence of centrilobular pattern of ground-glass opacities, septal lines and enlarged lymph nodes on HRCT of the chest) and the absence of pulmonary oedema after initiation of chronic vasodilator therapy 7–9. A histological confirmation of plexiform pulmonary arteriopathy was obtained in four patients (two post mortem and two explanted lungs). In the remaining seven patients, the diagnosis of IPAH did not require any invasive procedure to obtain pathological confirmation 7, 10.
Bronchoalveolar lavage
Fibreoptic bronchoscopy with BAL 16 was proposed to patients with PVOD because of abnormal radiological findings compatible with this diagnosis. In IPAH, it was performed either to explore a pulmonary opacity (n = 2) or before initiation of continuous intravenous epoprostenol (n = 9), after informed consent and ethics committee approval, in the context of a study, as previously described 17. Lidocaine was used for local anaesthesia. Three 50-mL aliquots of saline were instilled in the right middle lobe or in the subsegment that appeared to be pathological on a chest radiograph. Bacteriological and cytological analyses were performed using Gram and Papanicolaou stainings, respectively. Differential cell counts were performed on Perls-stained preparations. The Golde score was used to assess alveolar haemorrhage 18; 200–300 macrophages were counted and each cell was graded for haemosiderin on a scale of 0–4. A mean score for 100 cells was calculated, 0 being the minimum and 400 the maximum score 18. Haemosiderenic resorption was considered as normal if the Golde score ranged from 0–20, medium from 20–70 and high >70 18. The Golde score was obtained in a blinded fashion in all cases.
Statistical analysis
Statistical analysis was performed using nonparametric Mann-Whitney U-test and the Chi-squared test. Data were presented as mean±sd. A p-value of <0.05 was considered as significant.
RESULTS
Clinical, functional and haemodynamic information
There was a nonsignificant male predominance in PVOD and a female predominance in IPAH (male to female ratio of 1.7:1 and 0.4:1, respectively; tables 1⇓–⇓3⇓). Moreover, there was a nonsignificant predominance of tobacco smokers in the PVOD patients (75 versus 36%). Dyspnoea was the main symptom in all patients, and most of them were New York Heart Association functional class III or IV. The 6-min walk distance was 216±138 m in PVOD versus 372±82 m in IPAH (p = 0.02). PVOD was associated with a more severe hypoxaemia and a more pronounced reduction of carbon monoxide diffusing capacity (DL,CO) as compared with IPAH (p = 0.007 and p = 0.008, respectively; table 1⇓). Haemodynamics demonstrated severe pre-capillary pulmonary hypertension in all patients.
Clinical characteristics, haemodynamic parameters, lung function tests and bronchoalveolar lavage results in eight patients with pulmonary veno-occlusive disease (PVOD) and 11 patients with idiopathic pulmonary arterial hypertension (IPAH)
Individual data in eight pulmonary veno-occlusive (PVOD) disease patients
Individual data in 11 idiopathic pulmonary arterial hypertension(IPAH) patients
HRCT of the chest
HRCT of the chest was normal in nine of the IPAH patients. In the remaining two IPAH patients, there was a mild panlobular ground-glass opacity, which led to the indication of fibreoptic bronchoscopy. All of the PVOD patients had abnormal HRCT of the chest, showing the presence of ground-glass opacities (particularly with a centrilobular distribution), septal lines, and adenopathy (table 2⇑). One patient had these three major criteria, six patients had two criteria and one patient had only one of the criteria. Septal lines and enlarged lymph nodes were the most frequently present signs.
Bronchoalveolar lavage
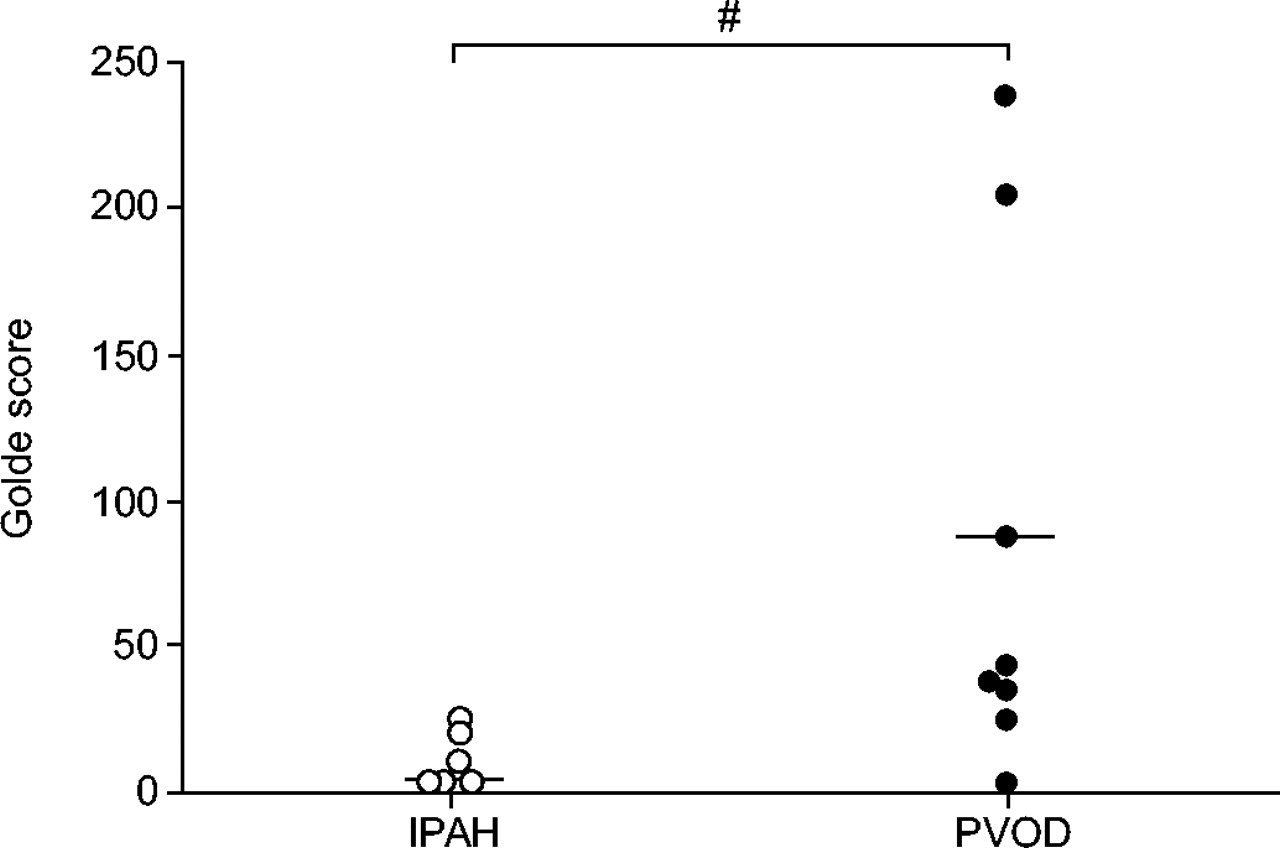
There was no evidence of infection and BAL fluids were carcinomatous cells free. As compared with IPAH, PVOD was characterised by a nonsignificant trend for elevated alveolar cell counts (410,250±366,500 cells·mL−1 versus 204,300±158,200 cells·mL−1), similar percentages of lymphocytes, neutrophils, and macrophages, but significantly higher percentages of haemosiderin-laden macrophages (40±37 versus 3±6%; p = 0.004; tables 2⇑–3⇑). Occult alveolar haemorrhage was better evaluated with the Golde score, which was markedly elevated in PVOD (81±88 versus 4±10; p = 0.002; fig. 1⇓). Only one PVOD patient had a Golde score <20 (fig. 1⇓).

Golde score in patients with idiopathic pulmonary arterial hypertension (IPAH) or pulmonary veno-occlusive disease (PVOD). #: p = 0.002.
DISCUSSION
PVOD is an uncommon cause of pulmonary hypertension, representing <10% of all pulmonary arterial hypertension cases, according to published series 3–6. In the most recent classification of pulmonary hypertension, PVOD was regarded as a subset of pulmonary arterial hypertension for several reasons 7. First, although showing predominant venous involvement, PVOD is characterised by histological changes of the small pulmonary arteries mimicking those of pulmonary arterial hypertension, including intimal fibrosis and medial hypertrophy 6, 7. Secondly, risk factors for PVOD and pulmonary arterial hypertension are similar, including systemic scleroderma, HIV infection, and appetite suppressant exposure 6, 7, 19–21. Thirdly, germline mutations of the gene encoding bone morphogenetic protein receptor II have been recognised in patients with familial pulmonary arterial hypertension and IPAH, as well as in cases of PVOD 22. Supporting the concept that these two conditions may overlap, there are reports of patients displaying PVOD or IPAH in the same families 7. Fourthly, clinical presentation of patients with PVOD is often undistinguishable from that of patients with IPAH 13.
According to recent guidelines, PVOD requires similar clinical management as other forms of pulmonary arterial hypertension 7. However, prognosis seems to be worse in this subset of patients, with a more rapid downhill course 7. In addition, vasodilators and especially continuous intravenous epoprostenol therapy have to be used with great caution because of the risk of severe pulmonary oedema 8, 9. As a result, it is critical to establish this diagnosis as early as possible, in order to consider lung transplantation for eligible patients 7–9.
More than 200 cases of PVOD have been reported in the literature. It affects all age groups without any geographical predilection. A male predominance has been shown in PVOD, as opposed to what is found in IPAH 13. The cause of PVOD remains obscure, but the process may be due to multiple factors that provoke a common pattern of vascular injury and repair 23. Some authors have proposed a viral aetiology, including infection with the HIV 21, 24. Haematological malignancies, as well as chemotherapy (bleomycin, gemcitabin, etc.), radiotherapy or bone marrow transplantation are other potential causes of PVOD 25–30. In this study, the current authors found a nonsignificant predominance of tobacco smokers in PVOD patients. It has been speculated that a toxic exposure could be responsible for occult alveolar haemorrhage and impaired function of alveolar macrophages: increased percentages of haemosiderin-laden alveolar macrophages were found in BAL fluid of cocaine smokers 31 and an impairment in nitric oxide production was observed in alveolar macrophages from smokers of marijuana and cocaine 32, 33. This chronic damage of the alveoli and of pulmonary microcirculation is not clear as far as tobacco exposure is concerned 31.
A definite diagnosis of PVOD is difficult to establish in the living patients. Indeed, examination of a surgical lung biopsy is necessary to obtain a histological confirmation, but this invasive procedure is too hazardous in patients with a major haemodynamic compromise 10. Therefore, less invasive methods to approach this diagnosis are now proposed in order to obtain a high index of suspicion 12.
Clinical presentation of these patients is often similar to that of patients with IPAH 13. However, findings suggestive of a diagnosis other than IPAH may be identified in PVOD, such as digital clubbing and bibasal crackles 13. Despite reports of elevated PAWP in cases of PVOD, haemodynamical parameters are, in fact, usually identical to that of IPAH with a normal PAWP despite post-capillary involvement 23, 34. This paradoxical normal PAWP is due to the fact that the disease process occurs in the small pulmonary septal veins with little or no obstruction of the larger pulmonary veins 4, 6, 25. Therefore, when PAWP is measured during right-heart catheterisation, the static column of blood produced is unaffected by the occlusion and reflects the normal pressure in the larger veins, not the elevated pressure in the capillaries 34, 35.
As compared with IPAH, the present data suggest that PVOD is associated with a more pronounced hypoxaemia and a severe reduction of DL,CO, while spirometry and lung volume measurements are within normal limits 36. These abnormalities may be explained by interstitial oedema and/or pulmonary capillary angiogenesis secondary to chronic pulmonary venous obstruction 37. Interstitial lung disease may indeed be identified in PVOD 12. HRCT of the chest allows a better analysis, and the current data confirm the results of previous studies, which have emphasised the relevance of this technique in the noninvasive approach of PVOD 12. Centrilobular pattern of ground-glass opacities, septal lines and enlarged lymph nodes are the main abnormal findings suggestive of PVOD 12. These abnormalities may be present on baseline HRCT of the chest and strongly correlate with a risk of life-threatening pulmonary oedema with continuous intravenous epoprostenol therapy 11, 12.
As PVOD mainly affects the post-capillary pulmonary vessels, it was hypothesised that it may be responsible for chronic occult alveolar haemorrhage. Therefore, cells harvested by BAL in patients with PVOD or IPAH were studied. As compared to IPAH patients, patients displaying PVOD indeed had a higher percentage of haemosiderin-laden macrophages and an elevated Golde score 18, confirming occult alveolar haemorrhage in most cases of PVOD.
This case series has several limitations. The analysis was retrospective. However, conducting a prospective trial would be extremely difficult in such a rare disorder and a majority of patients would not have a definite diagnosis of PVOD because lung biopsy is not recommended in these unstable patients. Lung transplantation or post mortem analysis of the lungs is available in only a minority of patients in any cohorts followed in pulmonary vascular centres. Moreover, BAL is not usually performed in patients with IPAH, unless there is some suspicion of associated pulmonary parenchymal disease. The current authors, therefore, proposed to use the results of a series of BAL that are available at their institution, as a comparator for this study 17. A histological confirmation was obtained in all eight PVOD patients and in four of the 11 IPAH patients. According to recent guidelines 7, the diagnosis of IPAH does not require any pathological confirmation. Indeed, examination of a surgical lung biopsy would be necessary to obtain a histological confirmation, but this invasive procedure is too hazardous in patients with a major haemodynamic compromise 10. Thus, a diagnosis of IPAH was established in all 11 patients on the basis of recently published guidelines 7, and was confirmed by the absence of radiological abnormalities suggestive of PVOD and the absence of vasodilator-induced pulmonary oedema.
In conclusion, the current study indicates that occult alveolar haemorrhage is a common feature of pulmonary veno-occlusive disease. The present authors propose that patients with a clinical suspicion of pulmonary veno-occlusive disease should benefit from a less invasive approach combining high-resolution computed tomography of the chest and bronchoalveolar lavage analysis to detect occult alveolar haemorrhage.
- Received May 6, 2005.
- Accepted August 23, 2005.
- © ERS Journals Ltd











{kind=link}