





Abstract
In order to evaluate chronic effects of long-term exposure to cotton dust on respiratory health, and the role of dust and endotoxin, longitudinal changes in lung function and respiratory symptoms were observed prospectively from 1981 to 2001 in 447 cotton textile workers, along with 472 silk textile controls.
The results from five surveys conducted over the 20-yr period are reported, including standardised questionnaires, pre- and post-shift spirometric measurements, work-area inhalable dust sample collections and airborne Gram-bacterial endotoxin analysis.
Cotton workers had more persistent respiratory symptoms and greater annual declines in forced expiratory volume in one second (FEV1) and forced vital capacity as compared with silk workers. After exposure cessation, in the final 5-yr period, the rate of FEV1 decline tended to slow in nonsmoking males, but not in nonsmoking females. Workers who reported byssinotic symptoms more persistently suffered greater declines in FEV1. Chronic loss in lung function was more strongly associated with exposure to endotoxin than to dust.
In conclusion, the current study suggests that long-term exposure to cotton dust, in which airborne endotoxin appears to play an important role, results in substantial adverse chronic respiratory effects.
Cotton-dust exposure may induce acute and reversible airflow limitation, expressed as byssinosis and cross-shift declines in forced expiratory volume in one second (FEV1). However, the magnitude of chronic airway disease after long-term exposure to cotton dust remains unclear. Several studies have indicated that long-term exposure may lead to chronic respiratory disease 1–3 and excessive loss of lung function 4, 5, whereas others have not 6, 7. Due to a scarcity of longitudinally collected data, some important questions remain unresolved. For instance, what is the magnitude of the chronic airflow obstruction in cotton dust-exposed populations? Are adverse chronic effects reversible if the exposure ceases entirely? Is there a connection between byssinosis and long-term loss in lung function? What are the causative agent(s) and determinants of cotton dust-related obstructive lung disease? This longitudinal cohort study was designed to address these questions.
The results of a cohort study that followed a group of Chinese textile workers exposed chronically to cotton dust have been reported previously 8, 9. One of the features of the cohort was that >50% of the workers were nonsmoking females, which allowed an assessment of the effects of cotton-dust exposure without confounding by smoking. These cotton workers were found to have a higher cumulative incidence of respiratory symptoms and an excessive chronic loss in lung function. To provide confirmatory evidence for the chronic respiratory effects of exposure to cotton dust, the current authors continued to observe these workers, and extended the study to 20 yrs. During the last 5-yr period, a major change in the cohort was that almost all (96%) of the workers retired from the textile industry. In the current study, the magnitude of the chronic lung function changes and respiratory symptoms was determined, and the respective roles of exposure to dust and endotoxin in the development of chronic airway obstruction were evaluated. In addition, it was assessed whether cessation of exposure leads to an improvement of chronic airway obstruction.
SUBJECTS AND METHODS
The initial cohort was established in 1981, and consisted of 447 cotton and 472 silk textile workers who were recruited in Shanghai, China 8. The four follow-up surveys were undertaken in 5-yr intervals. At the last survey, 346 cotton and 342 silk workers returned, reaching follow-up rates of 84% in the cotton and 77% in the silk group, after excluding 62 workers who were identified as deceased during the follow-up time. Overall, 559 workers (61%) participated in all five surveys, 114 (12%) in four, and 175 (19%) in three or two.
Inhalable air samplings on airborne cotton dust in the various work areas were measured at all surveys, except the final one, using vertical elutriators. Endotoxin assays were performed on the dust samples using the Limulus amoebocyte lysate assay, chromogenic method 10. Throughout the study, identical samples, sampler-location handling techniques and measurements were used. The sampling methods and calculated cumulative personal exposure to dust and endotoxin at each time period have been described previously 9.
A standardised questionnaire on work history, respiratory symptoms/diseases and smoking history was administered at each survey 11. In the current study, the symptoms of interest included byssinosis, chest tightness, chronic bronchitis, chronic cough and dyspnoea, as defined previously 9. Byssinosis was not ascertained at the last survey, since all of the workers had left the industry by that time.
Spirograms were performed at each survey by a trained technician with consistent methods, according to American Thoracic Society criteria 9. An 8-L water-sealed filled spirometer (W.E. Collins, Braintree, MA, USA), calibrated twice a day with a 3-L syringe, was used to record spirometric manoeuvres throughout the surveys. Workers were asked to refrain from smoking for ≥1 h before performing the test. Acceptable FEV1 tracings were allowed to vary by no more than 10% or 200 mL, whichever was greater, and the best values of FEV1 and forced vital capacity (FVC) from three acceptable curves were used, regardless of whether they were on the same tracing.
The longitudinal changes in pulmonary function were evaluated as annual declines (the differences in pre-shift FEV1 or FVC between the last and baseline survey divided by 20). The average annual declines in FEV1 and FVC were compared between cotton and silk workers as a whole group, and as stratifications by sex and smoking using unpaired t-tests. In addition, annual declines over the last 5 yrs were assessed for the potential effect of exposure cessation during this period. Subsequently, least square means of annual declines in FEV1 by reported times of byssinosis were obtained using ANCOVA, adjusted by age, height, sex and smoking. Respiratory symptoms were grouped into 0–4 categories according to reported times over the 20-yr period. The persistence of symptoms between cotton and silk workers was compared using the Cochran–Armitage test for trend.
To identify determinants for longitudinal changes in lung function, generalised estimating equation (GEE) models 12 were applied. This approach performs iterative generalised least squares, and makes full use of the repeated measurement data. Identity link function and exchangeable correlation structure were used. The values of lung function measured at each period were outcome variables, whereas age, sex, height, smoking, pack-yrs, years since last worked (i.e. time away from work-related exposure) and exposure to cotton dust were predictive variables. All variables except sex were time-dependent variables. Two separate models were applied as follows. First, the data from cotton and silk workers were combined into one model and possible interactions were examined. The second model fitted the data from the cotton workers only, and added repeated individual estimations of exposure to cotton dust and endotoxin.
A generalised linear model was fitted to explore possible exposure–response relationships between annual declines in lung function and the cumulative exposure to dust and endotoxin in cotton workers. The Genmod procedure fits a generalised linear model to the data by maximum likelihood estimation of the parameter vector β. An identity function was chosen to model these data. Cumulative exposure was expressed as quartiles (lowest, low, high and highest), according to the average values of estimated individual exposure. The lowest level served as a reference category in the models. Meanwhile, sex, age and height at the last survey, smoking habit and smoking amount over 20 yrs were adjusted.
RESULTS
Similar to the initial cohort, there were no differences in age, height and sex between cotton and silk workers at the last survey (table 1⇓). The cotton group contained smokers with more pack-yrs. Almost all smokers were male, with the exception of seven females in the cotton group. In contrast to the baseline data, in which FEV1 was 2.92 L in cotton workers and 2.88 L in silk workers, the average FEV1 at the last survey was lower in the former (2.31 L versus 2.36 L). Cotton workers had higher frequent symptoms of chest tightness, chronic bronchitis and chronic cough.
Demographic data of participating subjects at the last follow-up survey
In comparison with silk workers, cotton workers had greater annual declines in FEV1, either as a whole group, or as sex- or smoking-specified groups (table 2⇓). Similar trends were seen for FVC. In cotton workers, the rates of FEV1 over the last 5 yrs were similar to those over the 20 yrs, but smokers had a greater loss and nonsmokers had a smaller loss over the last 5 yrs. A similar result was obtained after the current authors excluded those who continued to work in cotton mills during the last period (n = 65). Silk workers, however, had generally smaller declines in FEV1 over the last 5 yrs than over the entire 20 yrs.
Annual declines in lung function(mL·yr−1) over the 20-yr period and the final 5-yr period#
There were 32% and 28% of cotton workers who reported byssinosis and chest tightness at least once, respectively (table 3⇓). For other nonspecific respiratory symptoms, persistence (reported twice or more times) was more common in cotton than in silk workers. All of the differences between cotton and silk workers were statistically significant.
Persistence of respiratory symptoms over 20 yrs in cotton and silk workers#
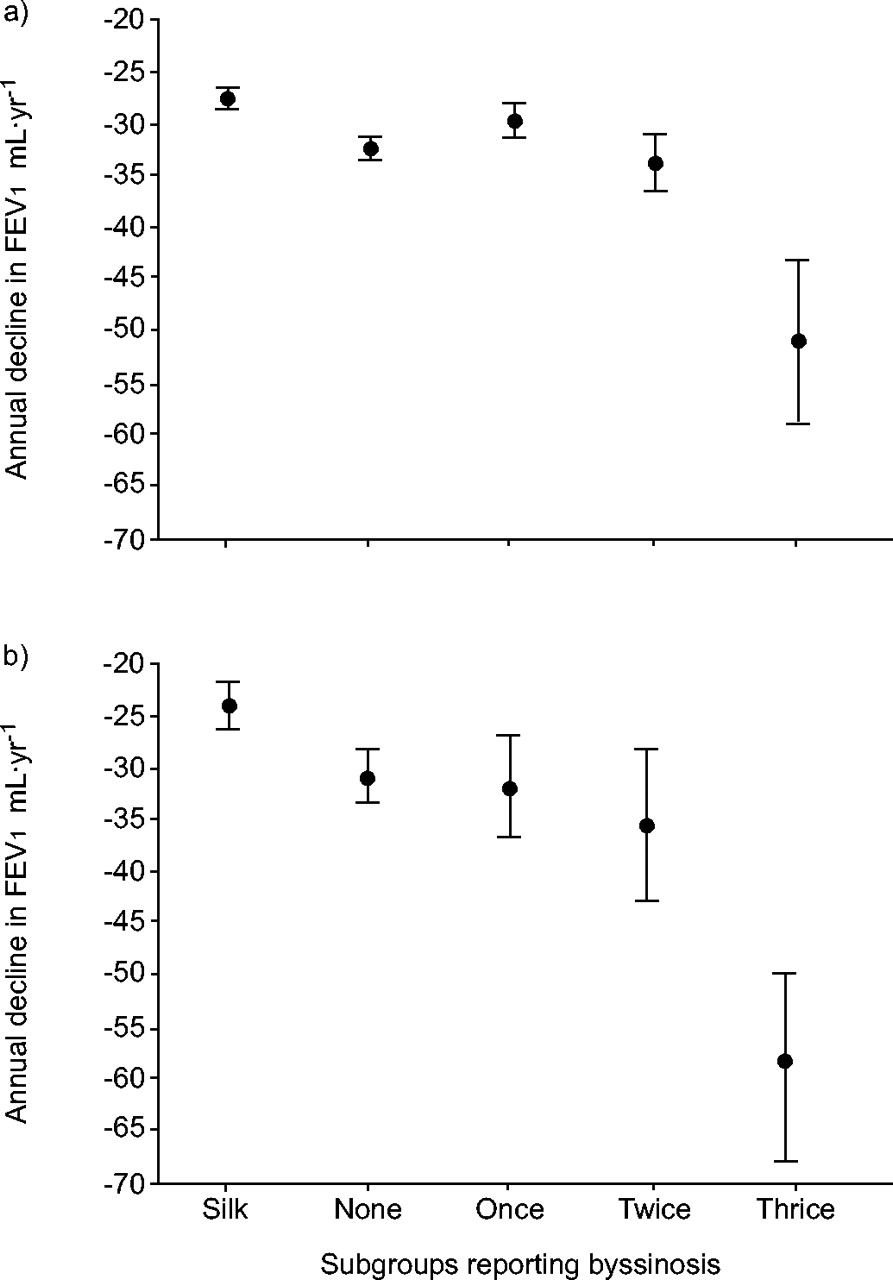
The adjusted annual declines in FEV1 in subgroups defined by the number of times reporting byssinosis, along with silk workers as referents, were compared (fig. 1⇓). Cotton workers, with or without byssinosis, had greater declines in FEV1 over both the last 5 yrs and the entire 20 yrs than silk workers. The FEV1 change tended to be greater as the reporting frequency of byssinosis increased. There was a significant difference (p<0.05) between the most persistent symptom subgroup and any of the other subgroups.

{kind=link}
Annual declines in forced expiratory volume in one second (FEV1) over the 20-yr period (a) and the last 5 yrs (b) by persistence of byssinosis in the cotton group, adjusted by age, height, sex and smoking with ANCOVA. The silk-worker group was included as a reference. The analysis was carried out among 346 cotton and 342 silk workers who participated in the last survey.
Longitudinal changes in lung function, estimated with GEE models that fit periodically repeated measurements in both cotton and silk workers, indicated that exposure status (cotton versus silk) was related to a significantly greater decline in FEV1 (table 4⇓). Although smoking did not exhibit a negative effect, it interacted strongly with sex on declines in lung function. Pack-yrs showed a marginally significant relationship with decreased FEV1. In the model restricted to fitting cotton-worker data only, similar results on smoking were observed. The level of exposure to endotoxin was negatively related to longitudinal changes in lung function. When the variable endotoxin or dust was included exclusively in the model, the relationship was unchanged. The number of years since last worked was positively associated with lung function, although this was not the case in the model that included both cotton and silk workers. Similar results were also observed for FVC (data not shown).
Estimates for change in forced expiratory volume in one second in lung function(mL) over a 20-yr period#
Furthermore, the relationships between cumulative individual exposures defined as quartiles and annual changes in lung function were assessed, while adjusting for age, sex, height at last survey and smoking habit, interaction of smoking and sex, and cumulative smoking amount (table 5⇓). Model 1, which fitted data from 165 cotton workers who participated in all of five surveys, showed a greater annual loss in FEV1 with increasing levels of exposure to endotoxin. Model 2, which used data from 306 cotton workers who had cumulative exposure data (from baseline to the last survey), showed a significantly greater loss of FEV1 in the highest level of endotoxin, in contrast to the lowest level, although the gradient was less obvious. Such a relationship was not seen in exposure to dust. Again, exclusively including endotoxin and cotton dust data did not lead to different results.
Adjusted annual changes# in lung function (mL) over a 20-yr period in relation to cumulative exposure level of dust and endotoxin in cotton workers
DISCUSSION
Substantial chronic respiratory effects in these workers were observed. First, the cotton workers reported more respiratory diseases and symptoms over the 20-yr period than the silk workers. In addition to byssinosis, which nearly one third of cotton workers reported at least once, the remaining possible symptoms were more common and persistent in the cotton workers. Secondly, and more importantly, the cotton workers had statistically significant excessive annual declines in FEV1 and FVC. For male smokers, the exposure effect over the 20 yrs was −9.2 mL·yr−1, whereas it was −2.6 mL·yr−1 for male nonsmokers and −3.1 mL·yr−1 for female workers, which suggested an additive effect between smoking and exposure. The result was consistent with that observed in male grain workers, in which annual losses in FEV1 were 28.7 mL for nonsmokers, and 41.7 mL for current smokers 13. Overall, the data provide further supportive evidence for the chronic effects of exposure to cotton dust, which has been suggested by the current authors' previous observations 8, 9 and by other cohort studies 4, 5.
It is generally believed that acute airway obstruction induced by a short-term exposure to cotton dust is reversible 14–16. However, it is not clear whether chronic airway changes associated with long-term exposure are reversible after the exposure ceases. Sparse data have provided inconsistent results 3, 17, 18. In this study, the rate of FEV1 decline did not change, as a whole group, during the last 5 yrs when the cotton workers retired from the industry entirely. However, in the last 5 yrs, nonsmoking male workers had a smaller rate of FEV1 decline (−28 mL·yr−1), in contrast to −35 mL·yr−1 over 20 yrs, and −40 mL·yr−1 over the first 15 yrs. Conversely, the decline rate in the smokers was accelerated (−48 mL·yr−1). The functional improvement in nonsmokers was supported by assessing the proportion of those who had an FEV1/FVC <70% (similarly defined as chronic obstructive pulmonary disease), where nonsmoking cotton workers had the largest improvement of FEV1/FVC over the last 5 yrs, from 35% at the 1996 survey to 26% at the 2001 survey, in contrast with 26% to 25% in the corresponding silk workers. These results imply that chronic airway obstruction may, to some extent, be reversible after the exposure ceases for those workers who do not smoke. Smokers appeared to have more persistent adverse effects due to the interaction between exposure to cotton dust and smoking 19.
It is noteworthy that females who were lifelong nonsmokers did not display an apparent improvement in FEV1 over the last 5-yr period. It was not clear why there was a sex difference in lung function improvement after exposure cessation in these workers. The exposure data between the males and females were compared, and no difference in work years and years since last worked was found. The males, however, had a significantly higher cumulative dust and endotoxin exposure than the females. It was assumed that an observed favourable effect was more notable from higher exposure previous to the exposure cessation. This assumption needs to be confirmed in further studies.
Few studies have examined the relationship between byssinosis and longitudinal changes in lung function. In the current study, it was found that the annual loss of FEV1 tended to be greater with reporting times of byssinosis, which suggested a connection between repeated attacks of byssinosis (probably chronic byssinosis) and excessive loss of lung function. When examining exposure intensity among subgroups by reporting times of byssinosis, the present authors found that exposure years were similar in the subgroups (ranging 24–28 yrs). Cumulative exposure to dust was highest in the most frequent reporting subgroup (three or more times), but similar among those with less persistent or no report. However, cumulative exposure to endotoxin exhibited a clear gradient with reporting frequency, implying that both repeated attacks of byssinosis and annual loss of FEV1 were related to the intensity of exposure, and especially to endotoxin.
A further analysis of the exposure–response relationship indicated that chronic loss of FEV1 was more highly associated with the level of exposure to endotoxin than to dust itself. These results support the hypothesis that airborne endotoxin is more likely to be a causative agent of chronic obstructive airway disease in workers exposed to cotton dust or to other organic dusts, which was consistent with previous cross-sectional and cohort studies conducted in different settings 9, 16, 20–25.
To the current authors' knowledge, this is the longest follow-up study, to date, in cotton textile workers. The large sample size and low attrition of the original cohort enhanced the study power to detect chronic respiratory effects due to exposure to cotton dust. Identical standardised methods, instruments and the same technicians were used throughout the study. Moreover, efforts were made to collect environmental exposure data, which has been rarely achieved in previous studies. However, the current authors were aware that there were two potential sources of biases in this study. First, despite generally high follow-up rates, there remained a small number in both groups who were lost to follow-up. To identify whether there was a differential loss to follow-up that might bias results, the present authors compared the health status at previous surveys between the followed subjects and dropouts at the next surveys. The dropouts generally had slightly lower FEV1 and there was a higher proportion of respiratory symptoms/diseases in both groups; however, none of the differences was statistically significant. The healthy-worker survivor effect could not have affected the current results substantially, given that it occurred in both groups. Secondly, the lack of personal air-sampling data was a possible source of exposure misclassification. Moreover, air sampling, collected from work areas, as periodic measurements of dust and bacterial endotoxin, was not performed throughout the entire period of follow-up, but instead at 5-yr intervals for ∼3–6 months' duration. Hence, the estimated personal cumulative exposure might not accurately reflect the actual level of individual exposure. Nevertheless, this study provided consistent evidence that airborne endotoxin played a more important role than dust itself in cotton dust-related diseases.
In conclusion, this study indicates that long-term exposure to cotton dust may result in excessive chronic annual loss in forced expiratory volume in one second, and in higher proportions of persistent respiratory symptoms or diseases, all of which were more highly related to exposure to cotton dust-associated endotoxin. A favourable effect of exposure cessation on lung function was observed in nonsmoking male workers, but not in smokers.
Acknowledgments
The authors would like to thank the members of the Shanghai field team; X-Q. Gu, P-L. Lu and T-T. Ye of Shanghai Medical University; the first Hospital of the Shanghai Textile Bureau; the workers and staff of the First and Second Textile Mills and the First Silk Mill (Putuo District, Shanghai); M. Chertok, J. Frelich and L. Pothier for research assistance; and M. Whitmer for assistance in endotoxin analysis.
- Received November 1, 2004.
- Accepted July 13, 2005.
- © ERS Journals Ltd
References









