





Abstract
Patients with nonsmall cell lung cancer (NSCLC) have been shown to have a higher prevalence of comorbidity associated with age and tobacco consumption. The objective of the present study was to determine the impact of comorbidity on survival after surgery of stage I NSCLC.
In total, 588 consecutive patients operated on for a pathological stage I NSCLC between January 1, 1979 and December 31, 2003 were studied. Comorbidities were analysed individually. Overall comorbidity was assessed using the Charlson index of comorbidity (CCI). Survival data were collected for each patient from the date of operation, with a median duration of follow-up of 104 months. Survival analyses and Cox proportional hazards model analyses were used.
The mean age of patients was 62.7 yrs, and 529 (89%) patients were male. The distribution of overall comorbidity severity was as follows. CCI grade 0: 47.1%; grade 1–2: 43.7%; grade 3–4: 8.3%; and grade ≥5: 0.8%.
The 2, 3 and 5 yrs survival were 69, 62 and 50%, respectively. Multivariable analysis showed that T stage, age, a concomitant history of moderate-to-severe liver disease, a past history of cured cancer, cerebrovascular disease and CCI were independent predictors of survival (Hazard Ratio for CCI grade >2: 1.81; 95% confidence interval 1.25–2.63).
In conclusion, comorbidity has a significant impact on survival after surgical resection of patients with stage I nonsmall cell lung cancer. The use of a validated index of comorbidity in prognostic analyses of resected nonsmall cell lung cancer is recommended.
Of all lung carcinomas ∼45% are limited to the chest, where surgical resection is not only an important therapeutic modality, but in many cases, the most effective method of controlling the disease. Patients with T1N0 and T2N0 tumours are curable by resection, with 5-yr survival rates in the range of 50–80% for patients with T1N0 status 1. However, despite a complete resection 30% of patients with stage I nonsmall cell lung cancer (NSCLC) die within 5 yrs of surgery. The site of first recurrence is distant in 74% of patients 2, demonstrating the high incidence of occult metastatic disease at the time of diagnosis.
This subset of patients with stage 1 NSCLC is well suited for prognostic studies. Hence, the standard of care is homogenous and anatomic lobectomy is the surgical treatment of choice in most cases. Furthermore, the outcome of these stage I NSCLC is not biased by organ failures complicating tumour compression or involvement. Many prognostic studies have been performed to evaluate the impact of various pathological or molecular markers. These studies have shown promising, but sometimes conflicting results and discrepancies. The current authors suggest that despite a correlation with classical clinical factors (i.e. age, sex and T1 versus T2), unrecorded data on comorbidities might bias, to a certain extent, these prognostic studies.
These prognostic studies will be complicated in the future by the recent development of multiple gene DNA arrays and their subsequent statistical cluster analyses, and from the clinicians point of view by the introduction of adjuvant chemotherapy in NSCLC stage I and II 3.
Lung cancer is associated with age and smoking, and both age 4, 5 and smoking 6, 7 are strongly associated with comorbidity. Thus, it is expected that comorbidity has an important impact in lung cancer patients, yet to date comorbidity has not been well studied in this population.
This last point emphasises the need for databases with baseline clinical data including comorbidities.
The Charlson comorbidity index (CCI) was developed by Charlson et al. 8 in 1987. Nineteen conditions were found to significantly influence survival in the study population and were given a weighted score based on the relative mortality risk (table 1⇓). The sum of the weighted scores of all of the comorbid conditions present in cancer patients was then scaled to establish the CCI. The CCI reflects both the number and seriousness of comorbid diseases. In the present study the prevalence and prognostic impact of each comorbidity and the overall impact of comorbidities is analysed in a large series of resected pathological stage I NSCLC using the CCI. In future studies on biological and genetic markers, performed in the same cohort of patients, CCI will be used to summarise all comorbidities.
Charlson comorbidity index(CCI) scoring
PATIENTS AND METHODS
Between January 1, 1979 and December 31, 2003, 588 patients (529 males; 59 females), underwent pulmonary resection for a pathological stage I NSCLC at Hôpital Albert Michallon (Grenoble, France).
Data collection
All cases of surgical resection of cancer were prospectively registered on a computerised database since 1988. A retrospective revision of cases prior to 1988 was also performed and these cases were retrospectively registered.
Histological typing occurred according to the World Health Organization histological typing of lung tumours 9. The post surgical (pathological) stages of the patients were determined according to the international tumour node metastasis (TNM) classification for lung cancer 10.
Age was split into two categories, <70 yrs and ≥70 yrs in uni- and multivariable analyses 11, 12
Smoking data included pack-yrs smoked (the average number of packages of cigarettes smoked per day multiplied by the number of years smoked). Smoking status was defined as lifelong nonsmokers, active smokers or former smokers if they had stopped >1 yr before surgery 13.
Patients were considered to have a comorbid condition if a listed disorder was mentioned in the records or if the patient was treated for it. In total, 19 conditions found to significantly influence survival in cancer patients were registered. Chronic obstructive pulmonary disease (COPD) was defined as follows 14: 1) forced expiratory volume in one second (FEV1 % predicted) <70%; and 2) FEV1/forced vital capacity <70%.
The CCI was computed for each patient. This summary method produces an individual score. The weights range from 1–6 (0 if the comorbidity is absent) and four CCI classes were defined as 0, 1–2, 3–4 and ≥5.
Statistical analysis
Analyses comparing categorical variables were carried out using Fisher exact tests. Analyses comparing continuous variables were carried out using unpaired t-tests. Median follow-up was calculated using the method of Schemper and Smith15. Overall survival was calculated from the date of surgery to the last day of follow-up or death. All patients surviving >5 yrs were censored after this time in order to avoid biases due to late mortality associated with comorbidity. Deaths occurring during the first 30 days were considered as hospital mortality. The method of Kaplan–Meier and the log-rank test were used. Multivariable analysis was performed using forward stepwise logistic regression with survival as the outcome variable of interest. Multiple clinical factors and epidemiological factors were analysed for possible influence on survival. Variables significantly associated with survival in the univariable analysis were introduced into the multivariable model. Odds ratios and their 95% confidence intervals were calculated. A p-value <0.05 was considered statistically significant.
RESULTS
Patient demographic characteristics
In total, 588 patients with pathological stage I NSCLC (pT1 N0 M0 or pT2 N0 M0) underwent surgery and were analysed in the current study. The main baseline characteristics are shown in table 2⇓. Most of these patients were smokers or former smokers. In most cases these patients were in good condition and fit enough to undergo surgery. The five most frequent comorbidities were: 1) chronic pulmonary disease (15.3%); 2) peripheral vascular disease (13.4%); 3) coronary artery disease (12.7%); 4) peptic ulcer disease (10.7%); and 5) diabetes (6.63%; table 1⇑). Some of these comorbidities were associated with tobacco consumption (unpaired t-test with the number of pack·yr−1): chronic pulmonary disease (p = 0.031); peripheral vascular disease (p = 0.0005); and coronary artery disease (p = 0.03). Age was also associated with some of these comorbidities (unpaired t-test): chronic pulmonary disease (p = 0.006); peripheral vascular disease (p = 0.0009); coronary artery disease (p = 0.01); diabetes (p = 0.003); and cerebrovascular disease (p = 0.0004).
Main baseline characteristics of the 588 patients
Of the patients, 39 had a previous history of malignancy within 5 yrs of surgery for lung cancer. These previous tumours were: 1) head and neck (26 patients); 2) head, neck and bladder (one patient); 3) head, neck and oesophagus (one patient); 4) oesophagus (one patient); 5) bladder (nine patients); and 6) carcinoma in situ of the bronchus (one patient). All of these tumours were associated with tobacco consumption.
No comorbidities or mild comorbidities (CCI 0–1) were found in 76% of patients. The CCI was associated with age (p = 0.0005) and the number of pack·yr−1 (p = 0.0023).
Pathological diagnosis, stage and treatment modalities are shown in table 3⇓. Most patients (84.2%) underwent lobectomy for treatment of NSCLC. However, 53 patients (9%) required a more extensive operation to ensure complete resection. Forty patients (6.8%) underwent limited pulmonary resection by segmentectomy or wedge excision.
Pathological diagnosis, stage and treatment modalities
Survival
Survival data were collected for each patient from the date of operation, with a median duration of follow-up of 104 months. In total, 27 patients were lost to follow-up (4.5%). The median actuarial survival for the entire group was 60 months. The 2, 3 and 5 yrs survival were 69, 62 and 50%, respectively. At the time of the current study 353 patients had died. During the 30 days following surgical resection 26 (4.4%) patients died due to: 1) bronchial fistula (seven patients); 2) cardiorespiratory failure (five patients); 3) sudden death (four patients); 4) infection (three patients); 5) cancer (two patients); 6) pulmonary embolism (one patient); 7) haemoptysis (one patient); 8) gastrointestinal haemorrhage (one patient); and 9) unknown cause of death (two patients). No prognostic variable of early death was found among the patients studied.
Due to a relapse of lung cancer, 172 patients have died and 155 have died of other causes (table 4⇓).
Causes of death of patients other than hospital mortality
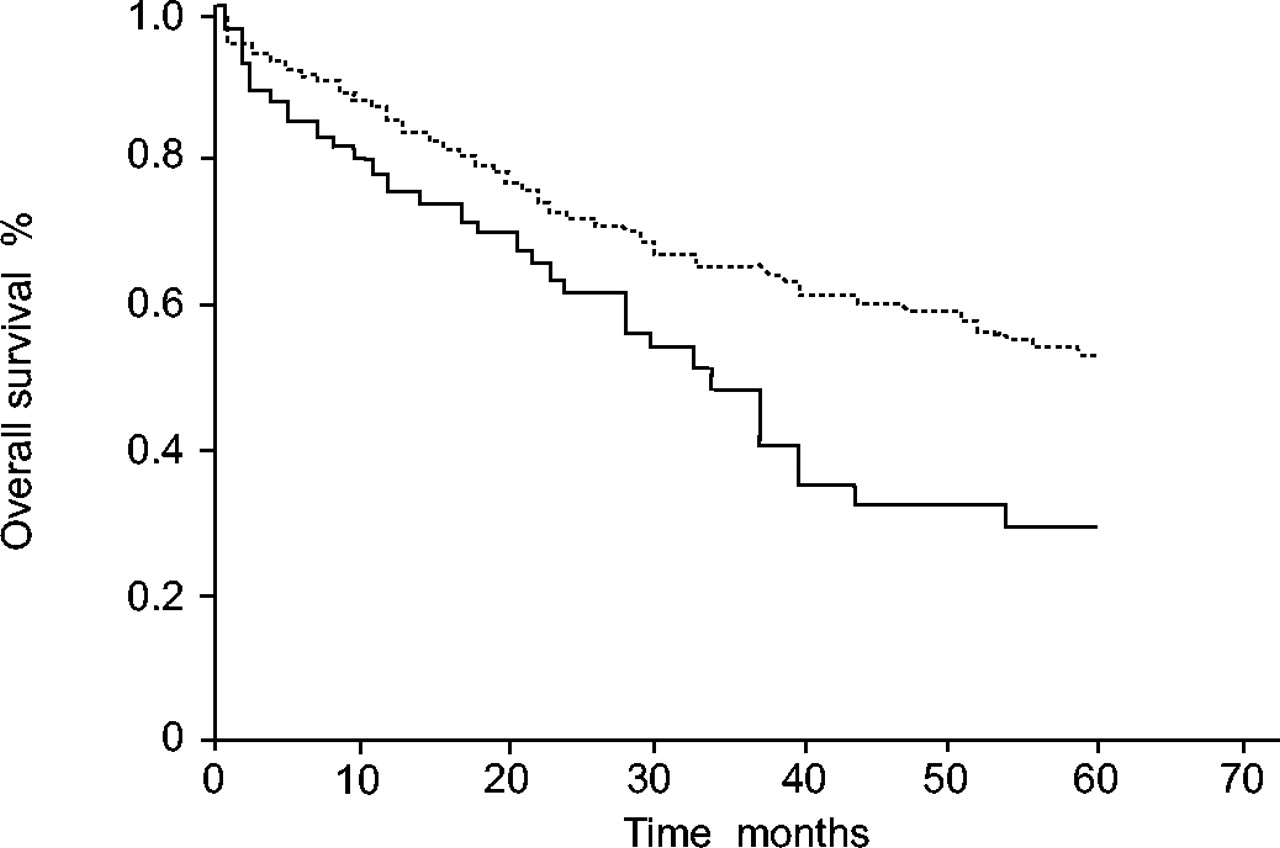
The survival rates of patients with reference to various variables are shown in tables 5⇓ and 6⇓. Univariable analyses identified eight of them as significant for a poor prognosis due to: pathological T2 status; aged ≥70 yrs, CCI and the following comorbidities: cerebrovascular disease; any prior tumour; moderate-to-severe liver disease; and connective tissue disease. Incomplete resection R1 (p = 0.08), histology (p = 0.058) and a past history of peripheral vascular disease (p = 0.09) were at the threshold of statistical significance. No difference in survival between patients with CCI grade 0 and those with CCI grade 1–2 (log rank test p = 0.37) was found. The current authors did not find any difference either between CCI grade 3–4 and CCI grade ≥5 (log rank test p = 0.96). However, the difference between CCI grade 1–2 and 3–4 was highly significant (log rank test p = 0.002; fig. 1⇓).

{kind=link}
Overall survival curves (%) according to the Charlson comorbidity index. – – –: Charlson 0, 1 or 2; –––: Charlson >2.
Relationship between categorical variables and survival of patients with surgically resected pathological stage I nonsmall cell lung cancer
Comorbidity prevalence in the population of 588 patients and univariable analysis of prognostic factors
Cox proportional hazard models were prepared evaluating the independent hazard associated with baseline covariables and five specific adverse comorbidities (model A), and additionally adjusted for Charlson comorbidity grading (model B).
Age and T status were associated with a prognostic significance (table 7⇓). In the Cox model a previous history of connective tissue disease did not confirm its prognostic significance, however, a previous history of cancer, severe liver disease or cerebrovascular disease were important predictors of survival (table 7⇓; model A). When the model was adjusted for baseline covariables and CCI, which summarises all concomitant comorbidities affecting a patient, patients with significant comorbidities (CCI > 2) had the worse prognosis (table 7⇓; model B).
Hazard ratios for variables in multivariable Cox models excluding and including baseline variables and comorbidities
DISCUSSION
Lung cancer is frequently associated with concomitant diseases. Of lung cancers >50% arise in patients aged ≥65 yrs 16. The impact of aging accounts for an increased risk of disease and disability, however, tobacco consumption, which is the main causative risk factor associated with lung cancer, explains as well the high frequency of concomitant disorders. In patients amenable to surgical resection, there is a careful selection before surgery to prevent excessive morbidity and mortality. Thus, most of these patients have mild or medically well-controlled concomitant disease. Among these, special attention is given to respiratory and cardiovascular disorders. Among surgically treated patients, the prognosis of post-operative stage I NSCLC may be explained further by the biological characteristics of the tumour, than by the tumour burden. This is the rationale for studying pathological and biological prognostic factors in this population. With the introduction of DNA and RNA arrays, multiple factors may be studied at the same time leading to complex statistical analyses and to the possibility of biases and misinterpretation. In the current article, the present authors hypothesise that concomitant diseases, even mild and medically well controlled, may impact the prognosis of resected stage I NSCLC.
In the current population of 588 patients surgically treated in the same institution, and followed during a long period of time (median duration of follow-up: 104 months) the 2, 3, and 5 yrs survival were 69, 62 and 50%, respectively. These survival figures are comparable with previously reported surgical series on stage I NSCLC 17. Of the patients 91% were smokers or former smokers. The five most frequent concomitant diseases were: 1) COPD (15.3%); 2) peripheral vascular disease (13.4%); 3) coronary artery disease (12.7%); 4) peptic ulcer disease (10.7%); and 5) diabetes (6.63%). More than 90% of patients had none or mild comorbidities. As expected, comorbidities such as COPD, peripheral vascular disease and coronary artery disease were associated with tobacco consumption with a high degree of statistical significance. Age was also associated with some of these comorbidities, i.e. COPD, peripheral vascular disease, coronary artery disease, diabetes and cerebrovascular disease. Pre-surgical selection of patients and a younger age (mean 62.7 yrs) explains, to a certain extent, a lower prevalence of comorbidities than reported in the literature. Janssen-Heijnen et al. 12 reported on a series of 3,864 lung cancer patients registered in the population-based registry of the Comprehensive Cancer Centre of Eindhoven (The Netherlands). The most frequent concomitant diseases in this unselected population were cardiovascular diseases (23%), COPD (22%) and other malignancies (15%).
In the present study comorbidities such as moderate-to-severe liver disease and a past history of cured cancer and cerebrovascular disease were significant prognostic factors of survival both in univariable and multivariable analyses. Surprisingly, COPD was not a prognostic factor. Lung cancer and COPD are common fatal diseases, and lung cancer is far more common in patients with COPD than in those with normal airflow obstruction 18. COPD is a well-established risk factor for post-operative complications following resection for NSCLC and for noncardiac thoracic surgical procedures in general 14, 19. The impact of COPD on survival remains, however, a matter of discussion, hence Sekine et al. 14 have shown a negative prognostic impact of COPD in univariable analysis, but this data was not confirmed in a multivariable analysis. The present data do not confirm the prognostic significance of a concomitant COPD, however, it should be stressed that only patients with an adequate pulmonary reserve are amenable to surgical resection of lung cancer and furthermore, careful care is provided to patients with COPD in the post-operative setting.
Cerebrovascular disease is one of the many aspects of the vascular status of these patients. In the current study, cerebrovascular disease is a negative predictor of survival, whereas peripheral vascular disease or coronary artery disease do not impact on survival. In a study on 515 lung resections for stage I NSCLC, Thomas et al. 1 have shown that arteriosclerosis was a negative prognostic factor. The current authors have merged peripheral vascular disease, cerebrovascular disease and coronary artery disease in an arteriosclerosis group, but not demonstrate any prognostic significance in uni- or multivariable analysis (data not shown; p = 0.059). Despite a borderline p-value this variable is not an independent predictor of survival. The current authors might not exclude that differences in coding “arteriosclerosis” could explain the difference between the present study and the study presented by Thomas et al. 1.
As multiple diseases may occur in the same patient, the CCI was used to rate cumulative comorbidity in the current study. This scale has been used in several different clinical studies showing its validity in predicting mortality 20–25.
In surgically resected NSCLC, Birim et al. 26 in a series of 205 patients (stage I–IV, including 144 stage I) showed a prevalence of CCI >2 in 25% of patients. Firat et al. 27, in a series of 113 resected stage I NSCLC patients, reported a 32% prevalence of CCI grade >2. In these two studies, CCI has shown to be a strong predictor of survival. In the current group of 588 patients, 9.1% of them had CCI >2. Despite a lower prevalence of moderate and severe comorbidities, CCI has demonstrated both in uni- and multivariable analysis to be an important prognostic factor aside from clinical variables such as T stage and age. Patients with CCI grade >2 have an important increase in mortality (hazard ratio 1.81). The behaviour of patients with CCI 0 and those with CCI 1–2 did not seem to differ (log rank test p = 0.37). The same equivalence was noted for patients with CCI grade 3–4 and CCI grade >5 (log rank test p = 0.96). It should be recommended in future studies to split patients into two groups CCI ≤2 or >2. This subclassification has proved to be useful in the work of Firat et al. 27. Other comorbidity scales have been studied in NSCLC, Battafarano et al. 28 have studied the prognostic significance of the Kaplan-Feinstein Index (KFI) on a group of 451 patients followed during 35.7 months. The KFI is an overall comorbidity score (none, mild, moderate or severe) determined on the basis of the number of ailments and their individual degrees of decompensation. In this index, 11 organ systems and 22 diseases are considered. The KFI had a significant impact on survival after surgical resection of patients with stage I NSCLC.
Firat et al. 27 have also studied the impact of the Cumulative Illness Rating Scale for Geriatrics (CIRS-G). The CIRS-G 20, grades the severity of impairment of 13 organ systems from 0 (no problem) through to 4 (extremely severe impairment). Although, Firat et al. 27 noted some discrepancies between CCI and CIRS-G, both scales were significant predictors of overall survival. In the current authors' opinion, CCI is an easy to perform comorbidity scale. The present results, performed in the largest series of selected pathological stage I NSCLC followed-up over a long period of time, confirm its prognostic significance. The authors agree that CCI is a more restrictive way than other tests to rate comorbidity and that it may underestimate the prevalence of comorbidity, but this scale appears well suited for prospective and retrospective studies. Most of the items are easy to retrieve from patient's clinical records. Despite a pre-surgical selection of patients, CCI had a strong prognostic impact on overall survival.
In conclusion, comorbidities are critically important in the clinical care of patients with cancer as they can have a profound impact on so many aspects of care, from prevention, screening, and diagnosis to prognosis, cancer treatment, and health service needs. The influence of tumour or treatment-related factors, such as tumour size, T stage, histological features, grade, DNA ploidy, molecular abnormalities and type of surgery on overall survival has been tested in numerous studies, without comorbidity assessment. The present results suggest that occult biases related to comorbidities may have influenced the conclusion of these studies. Thus, the authors recommend the use of a validated comorbidity scale. As far as they are concerned they have introduced the Charlson comorbidity index into the clinical data associated with tumour specimens stored in the tumour bank of their institution.
Acknowledgments
The authors would like to thank J.F. Timsit who reviewed the statistical methods and results.
- Received December 20, 2004.
- Accepted May 30, 2005.
- © ERS Journals Ltd
References









