





Abstract
Mortality studies of males and females with chronic obstructive pulmonary disease (COPD) and asthma have suggested that females have a poorer prognosis than males, but the results are either not unanimous or based on poorly characterised patients. The current study analysed the mortality of 279 asthma patients and 869 COPD patients, who were seeking pension due to disability, and compared mortality rates with expected rates derived from the general population.
The mean follow-up period was 13.3 yrs (range 2.5–22.4 yrs) during which time 96 (34.4%) and 671 (77.2%) deaths were identified among asthma and COPD patients, respectively. The average age at study entry was 46.8 and 56.6 yrs, and the average forced expiratory volume in one second (FEV1) was 68.8 and 44.1 % predicted in the two diagnostic groups. After adjustment for predictors of survival (age, FEV1 % predicted, chronic bronchitis, body mass index, smoking status, oral prednisolone, ischaemic heart disease, and cor pulmonale), the relative risk of death was 1.21 (95% confidence interval: 0.77–1.89) and 0.98 (0.83–1.16) in females compared with males, in asthma and COPD patients, respectively.
The standardised mortality rate (SMR) for males was 1.54 (1.10–2.09) and 2.7 (2.5–3.0), and for females 1.91 (1.44–2.49) and 4.8 (4.2–5.4), in asthma and COPD patients, respectively. Direct comparison of the SMR of males and females showed that females had higher mortality than males, with a rate ratio of 1.24 (0.82–1.84) and 1.8 (1.5–2.0), in asthma and COPD patients, respectively. Poisson regression analysis with control for the confounders did not change this result.
Females and males with the same level of obstructive lung disease appear to have the same level of mortality. However, using standardised mortality rates, females have a higher mortality than males, suggesting that the protective effect of being female is lost in chronic obstructive pulmonary disease patients.
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of morbidity and mortality and, while the mortality rate is stable among males, it is increasing among females 1–4. Several studies have shown that mortality is increased in patients with asthma and COPD, with increasing excess mortality related to low forced expiratory volume in one second (FEV1) 5–12. Studying asthma patients, Markowe et al. 7 and Sunyer et al. 11 found higher excess mortality in females compared with males, although other studies reported no sex difference 5, 8, 9. Some of these studies are dated, and patients were treated according to guidelines created before the introduction of inhaled corticosteroids.
The existence of sex-related survival differences in COPD has also been considered 11. In a study of COPD patients who visited emergency rooms, Sunyer et al. 11 showed that excess mortality from all causes and respiratory disease was higher in females compared with males. However, they have not reported data on lung function, smoking habits, medication, pulmonary symptoms or comorbidity. In this prospective study of patients with asthma and COPD, sex-related differences in mortality rates and excess of mortality were studied.
METHODS
From 1977–1997, ∼2,200 patients with pulmonary symptoms were referred to two specialists in pulmonary medicine for medical evaluation of disability. Before the patients, always as outpatients and during stable medical condition, were evaluated, most had been in contact with a specialist practice or a hospital. Before the evaluation by the pulmonary specialists, most of the patients had a reversibility test with inhaled β2-agonists and some with oral corticosteroids. If the result of such a test was ambiguous or had not been performed, a reversibility test using 2 mg of terbutaline from an inhalator was administered (49.7% of the patients). COPD was defined as FEV1 <80% of predicted value, a FEV1/forced vital capacity (FVC) ratio <70%, and exclusion of other obstructive airway diseases, such as asthma and bronchiectasis. The two pulmonary specialists made the diagnosis after an evaluation, including a file of previous examinations as an outpatient or during hospitalisation, a lung function test, reversibility tests and, frequently, additional tests (total lung capacity in 48.1% and diffusion capacity in 1.9%). In this study, the asthma diagnosis was used if the patient had any asthmatic component, including an absolute increase in FEV1 >250 mL after β2-reversibility test. Chronic bronchitis was defined as phlegm ≥3 months in 2 consecutive yrs. All patients were asked the same questions and had FEV1 and FVC measured with a spirometer (Vitalograph, Ennis, Ireland) 12. The study comprised 1,148 subjects. COPD was diagnosed in 869 cases and asthma in 279 cases. Patients with comorbidity from actual cancer, previous pulmonary resection, ciliary dyskinesia, bronchiectasis, cystic fibrosis, α1-antitrypsin deficiency, simple chronic bronchitis with normal lung function, actual or previous pulmonary tuberculosis or pneumothorax, and 17 patients with both COPD and asthma were excluded.
The number of pack-yrs of tobacco was calculated (one cigarette = 1 g, one cheroot = 3.5 g, one cigar = 5 g, pipe tobacco: actual number of grams). As ischaemic heart disease is a frequent contributor of pulmonary symptoms in tobacco smokers, this disease was also reported. A diagnosis of ischaemic heart disease was based on the previous files, and from the history and physical examination obtained by the pulmonary specialist, a diagnosis of ischaemic heart disease was made.
The National Health Services Central Register ascertained vital status until September 1, 2003. The mean follow-up period was 13.1 yrs (range 2.5–22.4 yrs), during which time 767 (66.8%) deaths were identified among the 1,148 patients. Eight patients had emigrated, and survival until emigration was included.
Statistics
Cox proportional hazards regression was used to determine whether sex was associated with increased mortality from all causes. The hazard ratios (relative risks (RR)) were calculated for the following covariates, which were defined a priori: age, FEV1 % predicted (<40, 40–59, 60–79 and ≥80), body mass index (<20, 20–24.9, 25–29.9 and ≥30 kg·m−2), pack-yrs of smoking (0, 1–19, 20–39 and ≥40), smoked tobacco at evaluation (0, 1–14 and ≥15 g·day−1), treatment with prednisolone (yes/no), treatment with inhaled corticosteroids (yes/no) comorbidity from ischaemic heart disease (yes/no), chronic bronchitis (yes/no), and, finally, cor pulmonale (yes/no). The hazard ratios were adjusted for those covariates, which were related to death. Adjusting for period of entrance did not change the results.
Continuous variables were transformed into the standardised categories as listed above if linearity was not present. Assumption of linearity was assessed by categorising the variable into multiple dichotomous variables of equal units on the variable's scale. The estimated coefficients of each dichotomous variable were compared. The period of follow-up for survival calculation was taken from the date of the first examination, to the date of death, emigration, or September 1, 2003, whichever came first. Expected survival rate was calculated from age, calendar time, and sex-specific mortality tables of the Copenhagen (Denmark) area published by the Danish Statistical Bureau. The rate ratios for mortality were calculated as the ratio of the observed number of deaths per person year of follow-up to the expected death rate. These rate ratios are referred to as RR. Chi-squared tests were used for univariate analysis and Poisson regression analysis used for multivariate analysis of mortality rates.
Analyses were employed for patients with asthma and COPD, separately. A two-sided p-value of <0.05 was considered significant.
RESULTS
Characteristics of the study groups are shown in table 1⇓.
Characteristics of patients applying for benefits due to disability according to respiratory disease and sex, and the number of deaths
Asthma patients
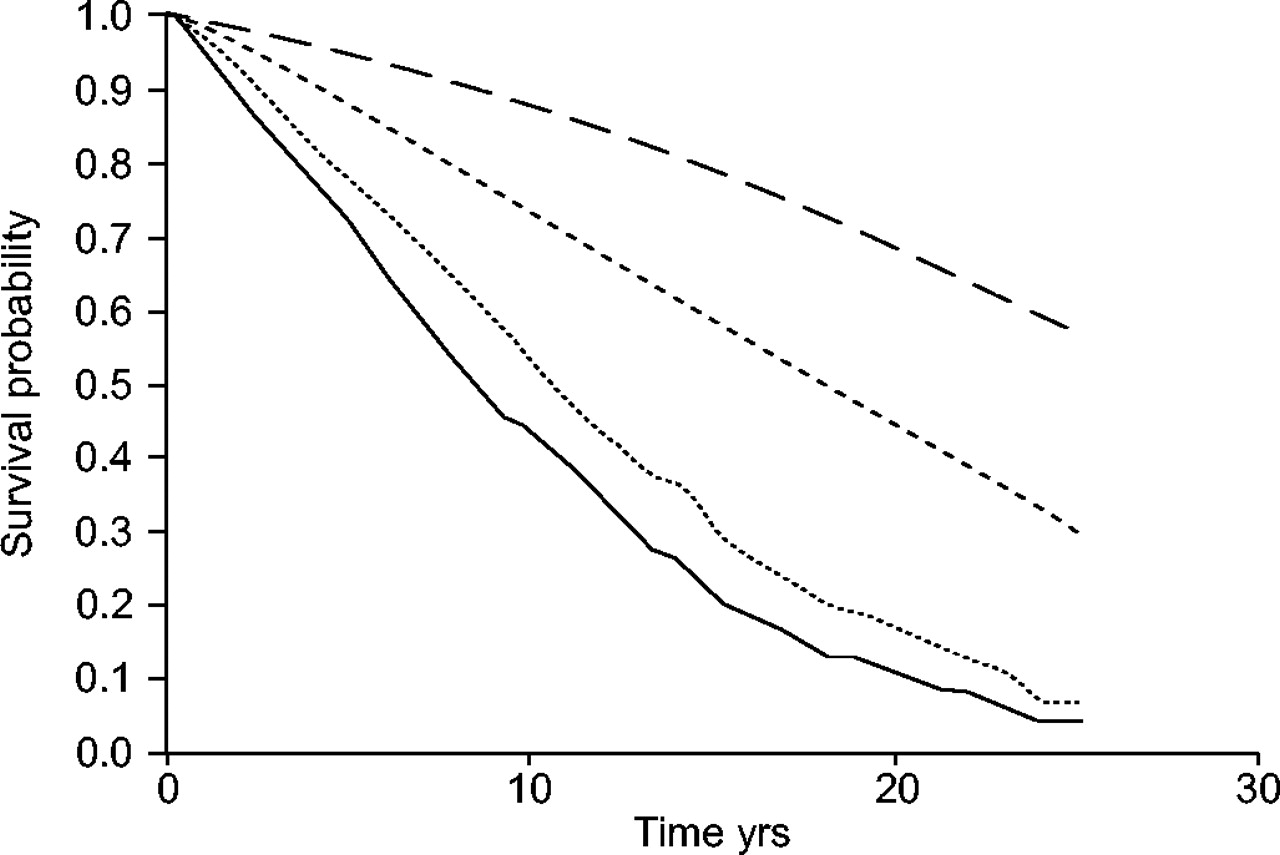
During the follow-up time, 96 of the 279 patients with asthma died. The median survival time was 17.7 yrs for patients with asthma, with a tendency towards a decreased risk of mortality for females (RR: 0.77 (0.51–1.15); fig. 1⇓). Adjustment for predictors of survival (covariables listed in statistics) increased the RR of mortality for females to 1.21 (0.77–1.89).

Observed and expected life table plot of males and females with asthma. – – –: females expected; …..: females observed; - - -: males expected; ––––: males observed.
Compared to an age-matched control group, the mortality rates were increased significantly by a factor of 1.54 (1.10–2.09) in males and 1.91 (1.44–2.49) in females with asthma (table 2⇓). This sex-related difference in excess of all cause mortality was not significant, with risk ratio of 1.24 (0.82–1.84; p = 0.33).
Excess of mortality in patients with asthma and chronic obstructive pulmonary disease (COPD) separately for each sex
COPD patients
During the follow-up time 671 of the 869 patients with COPD died. The median survival time for patients with COPD was 8.5 yrs, with a significantly lower risk of mortality in females compared with males (RR: 0.75 (0.64–0.88); fig. 2⇓). After adjustment for predictors of survival (listed in statistics), the RR of death was 0.98 (0.83–1.16) in females compared with males (table 3⇓).

{kind=link}
{kind=link}
Observed and expected life table plots of males and females with chronic obstructive pulmonary disease. – – –: females expected; …..: females observed; - - -: males expected; ––––: males observed.
Risk factors presented as hazard ratios among patients with chronic obstructive pulmonary disease for any cause of deaths, using Cox regression analysis
Compared to an age-matched control group, the mortality rates were increased significantly by a factor of 2.7 (2.5–3.0) in males and 4.8 (4.2–5.4) in females with COPD (table 2⇑). This sex-related difference in excess of all-cause mortality was significant with a risk ratio of 1.8 (1.5–2.0).
DISCUSSION
The major finding in this study is that although the survival of males and females was similar, comparison of standardised mortality rate (SMR), which adjusted for expected survival, showed that females had higher SMR than males, suggesting that females with COPD lose more years of their lives than males. The females had the same degree of disease severity (lung function and treatment with oral glucocorticoids) and were even smoking less. These results are in accordance with the studies of Sunyer et al. 11, Markowe et al. 7 and Lange et al. 14 (table 4⇓). Sunyer et al. 11 found ratios between females and males of 1.21 and 1.15, respectively, regarding the risk of excess mortality in COPD and asthma patients 11. Due to a high number of deaths in their study, these sex-related risks of excess mortality were statistically significant 11. In the current study, the mortality rates were similar for females (∼45/1,000 patient·yr−1) and slightly lower for males compared with the Spanish study (63 versus 90/1,000 patient·yr−1) 11. They had included a lower number of females with COPD, but a closer comparison is not possible, because they had not reported data on lung function, medication, smoking habits, pulmonary symptoms or comorbidity. Data from the Copenhagen City Heart Study, a prospective population study, showed that subjects with FEV1 <40% had an increased risk of mortality compared with a matched control group with normal FEV1, with a RR of 5.0 for females and 2.7 for males 14. Compared with a matched control group, Markowe et al. 7 found that asthma patients from general practitioners had an increased risk of mortality (RR of 2.19 in females and 1.39 in males) 7. A population-based study of patients with self-reported asthma and 161 deaths found a tendency towards higher excess of mortality in females compared with males (RR = 1.7 versus 1.5) 8. However, two older studies of asthma patients have reported no sex-related difference in excess of mortality (table 4⇓), and they have not presented data on smoking history 5, 9. In the current study, only 32.7% of the females were never-smokers, and this is expected to be less than in the old asthma studies 5, 9. This may explain why they did not find a higher excess of mortality in females compared with males. Using data from Danish population studies, Prescott et al. 15, 16 showed that, among smokers, females had an increased loss of lung function and risk of dying from respiratory and vascular diseases compared with males. In the current study, the excess mortality in females was independent of smoking status at evaluation (data not shown).
Studies examining the excess of mortality in patients with asthma, for each sex separately
It should be considered that the patients were only evaluated at the time of the referral, and they might later have changed smoking status. However, the current authors believe that this number is about the same for males and females. According to the Lung Health Study, which evaluated patients for 5 yrs, smoking cessation intervention leads to sustained smoking cessation in 18.3% of males and 15.7% of females 17. Misclassification of COPD and asthma is a known problem, especially among the elderly. A separation of asthma from COPD is based on several clinical parameters. In the current study, data on smoking history, symptoms (attack of dyspnoea, nocturnal dyspnoea and chronic bronchitis), and use of inhaled steroid support a correct separation in most cases. When the reduced life expectancy was seen in both COPD and asthma patients, any misclassification would only increase the risk for one subgroup at the expense of the other subgroup.
It cannot be excluded that seeking pension depended on sex. According to data from The Board of Danish Statistics, the percentage of unemployment in males was constantly ∼2% higher than for females in the studied area, and the number of males who received a pension in this area was constantly some 15% higher than for females. This indicates that more males than females were seeking a pension. However, the current patients were well characterised, and females seem not to have more severe disease compared with males.
The patients in the current study were characterised by having pulmonary symptoms, and all chronic obstructive pulmonary disease patients had moderate to very severe disease. Therefore, the present findings do not represent all asthma and chronic obstructive pulmonary disease patients. Further studies are needed in patients with mild chronic obstructive pulmonary disease. Data from the current study support previous findings that females with obstructive lung disease, especially chronic obstructive pulmonary disease, had higher excess mortality compared with males.
- Received August 25, 2004.
- Accepted December 10, 2004.
- © ERS Journals Ltd
References









