





Abstract
Accurate staging of the mediastinum in lung cancer is essential for optimising treatment strategies. Conventional transbronchial needle aspiration (TBNA) is a blind procedure, reliant upon prior computed tomography (CT) or ultrasound imaging, but has low sensitivity. The current study reports the initial experience of using a prototype endobronchial ultrasound (EBUS) probe that allows TBNA under real-time imaging.
In 20 patients selected by CT scanning, a linear-array ultrasound bronchoscope was used to visualise paratracheal and hilar lymph nodes, and TBNA was performed under direct ultrasonic control. In seven cases, sequential endoscopic ultrasound (EUS) was used to assess postero-inferior mediastinal lymph nodes. All procedures were performed under conscious sedation.
EBUS-TBNA was undertaken in 18 out of 20 cases and EUS-guided fine-needle aspiration in six out of seven cases. Cytology showed node (N)2/N3 disease in 11 out of 18 EBUS-TBNA cases and provided a primary diagnosis for eight patients. EBUS-TBNA cytology was negative in six cases, which was confirmed by mediastinoscopy or clinical follow-up in four. EUS provided additional information in all cases. There were no procedural complications. Sensitivity, specificity and accuracy for EBUS-TBNA were 85%, 100% and 89%, respectively.
In conclusion, endobronchial ultrasound with real-time transbronchial needle aspiration offers improved sensitivity and accuracy for staging of the middle mediastinum, and, combined with endoscopic ultrasound, should allow investigation of the majority of the mediastinum.
- Endobronchial ultrasound
- endoscopic ultrasound
- fine-needle aspiration
- lung cancer
- mediastinal lymphadenopathy
Accurate staging of lung cancer is essential in order to plan effective treatment and to optimise survival rates. Locoregional spread involves mediastinal lymph node involvement, and this is a key arbiter of surgical resectability. Current scanning modalities, such as computed tomography (CT) and positron emission tomography (PET), although useful, are not sufficiently sensitive or specific to determine mediastinal nodal involvement. Recent pooled data on CT and PET scanning showed that the sensitivity and specificity for predicting malignant involvement of mediastinal lymph nodes were 60% and 81%, and 84% and 89%, respectively 1. Due to these problems, lymph node sampling is regarded as the most accurate predictor of nodal status. For many years, mediastinoscopy has been regarded as the “gold standard” for staging of the mediastinum, but it is invasive, requires a general anaesthetic and is costly. While a standard cervical mediastinoscopy permits access to paratracheal lymph node stations (levels 2 right (R), 2 left (L), 3, 4R and 4L) and usually the anterior subcarinal lymph node station (level 7), access to the posterior and inferior mediastinum is limited and requires either extended cervical mediastinoscopy or a thoracoscopy. Furthermore, the sensitivity for mediastinoscopy is still only 80–90%, and, in 10–15% of cases, the technique returns a false-negative diagnosis 2, 3. Failure to identify mediastinal disease pre-operatively contributes to tumour relapse rates, despite apparently successful resection. The development of methods to improve mediastinal staging will diminish the incidence of futile thoracotomy and will allow initial treatment plans to be optimised.
The current authors describe their initial experience of a novel prototype linear-array endobronchial ultrasound (EBUS) probe with a fine-needle biopsy facility for real-time imaging and aspiration biopsy of paratracheal and parabronchial lymph nodes (stations 2, 3, 4, 7, 10 and 11). When combined with conventional endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) for assessment of the postero-inferior mediastinum (stations 4L, 5, 7, 8 and 9), these techniques offer the potential of staging the majority of the mediastinum using minimally invasive methods under local anaesthetic and conscious sedation.
METHODS
A total of 20 patients with known or suspected lung cancer were referred for EBUS-guided transbronchial needle aspiration (TBNA) evaluation of mediastinal lesions. Patient selection was based on CT findings showing mediastinal lymph node enlargement or the presence of paratracheal or parabronchial masses. In general, mediastinal lymph nodes were regarded as enlarged if >1 cm in short-axis dimension. All patients signed informed consent, and approval for the use of this new technique was granted by the Royal Infirmary of Edinburgh, Edinburgh, UK. All procedures were performed on an outpatient basis, under conscious sedation using midazolam and fentanyl. EBUS was performed using a novel prototype linear-array ultrasonic bronchoscope (XBF-UC260F-OL8; Olympus Ltd, Tokyo, Japan; fig. 1⇓). The instrument is similar to a standard bronchoscopic videoscope, with an outer diameter of 6.9 mm, a 2.0-mm instrument channel and 30° oblique forward-viewing optics. An electronic convex-array ultrasound transducer is mounted at the distal tip and is covered by a water-inflatable balloon sheath. Scanning is performed at a frequency of 7.5 MHz and allows a penetration of 20–50 mm. Image processing is performed by an Olympus ultrasound processor (EU-C2000; Olympus Ltd). The probe was passed through the mouth and vocal cords to the main carina, the balloon partially inflated (0.3–0.5 mL of water), and paratracheal and hilar lymph node stations (stations 2, 3, 4, 7, 10 and 11) 4 were systematically identified and measured (short-axis diameter) during slow withdrawal and rotation of the transducer. The location of lymph nodes in each station was determined by the position of the bronchoscope within the airway, in conjunction with the CT scan and ultrasonic image. In the current authors' experience, partial inflation of the balloon, in order to improve the ultrasonic image, is required when scanning from within the trachea, but balloon inflation is rarely required in the main bronchi or subdivisions because the transducer wedges against the airway wall more easily.

Distal end of the endobronchial ultrasound probe (XBF-UC260F-OL8; Olympus Ltd, Tokyo, Japan), showing the curved-array ultrasound transducer with the balloon inflated and a 22-gauge aspiration needle protruding from the biopsy channel.
TBNA was performed by passing a dedicated prototype 22-gauge needle (XNA-200C-5; Olympus Ltd) through the airway wall and into the lymph nodes under real-time ultrasound control. Needle punctures were performed using the “jabbing” method 5. On occasion, cartilage rings prevented needle puncture. In this case, the bronchoscope was moved a few millimetres cranially or caudally and repeat puncture was performed. Integrated colour-power Doppler ultrasound was used to exclude intervening vessels immediately prior to needle puncture. To minimise cough during needle aspiration, 1% lignocaine was applied to the airway wall prior to needle puncture. In practice, needle puncture invariably displaces the balloon/transducer from contact with the airway wall with consequent loss of the ultrasonic image. However, imaging can be restored by gentle inflation of the balloon with water so that it is brought back into contact with the airway wall.
Additional EUS examination was performed in patients in whom the staging CT scan had demonstrated enlarged lymph nodes in the posterior or inferior mediastinum, inaccessible by an endobronchial approach (i.e. stations 5, 8 and 9, and postero-inferiorly placed lymph nodes in station 7). EUS-FNA was performed using a curved linear-array echoendoscope Olympus GF-UC240P-AL5 (KeyMed Ltd, Southend-on-Sea, UK). Initially, the instrument was passed into the stomach, and the left adrenal gland and left lobe of the liver were identified and imaged. Then, during slow withdrawal and rotation of the probe through the oesophagus, the lymph node stations of the posterior and inferior mediastinum were systematically identified and examined. FNAs were performed through the wall of the oesophagus under real-time guidance using Wilson-Cook 22-gauge FNA needles (EUSN-3; Cook UK Ltd, Letchworth, UK).
For both EBUS-TBNA and EUS-FNA, successive passes were made until the endoscopist judged an adequate specimen had been obtained, i.e. when macroscopically visible material had been obtained from 2–3 needle passes. At the Royal Infirmary of Edinburgh, no cytopathologist was present during the procedure. Samples were collected into cytological fixative (Cytolyt; Cytyc Corporation, Boxborough, MA, USA) for cytological examination. All patients were observed for 2 h post-procedure before discharge.
RESULTS
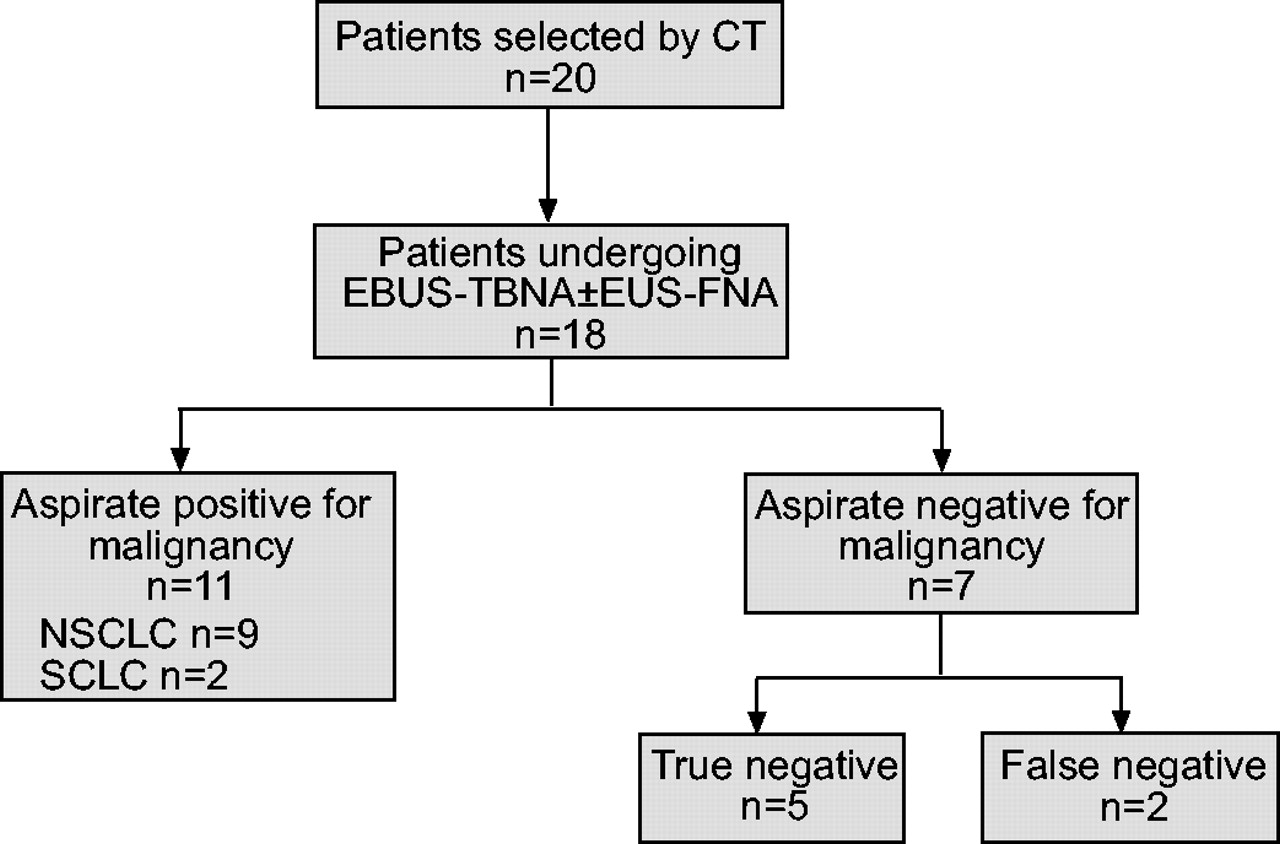
EBUS was performed in 20 patients (10 male; median (range) age 65 yrs (45–86)), of whom seven underwent combined EBUS and EUS examinations. EBUS-TBNA was undertaken in 18 out of 20 cases and additional EUS-FNA in six out of seven cases (table 1⇓; fig. 2⇓). It should be noted that two of the combined EBUS/EUS cases have previously been described in more detail 6.
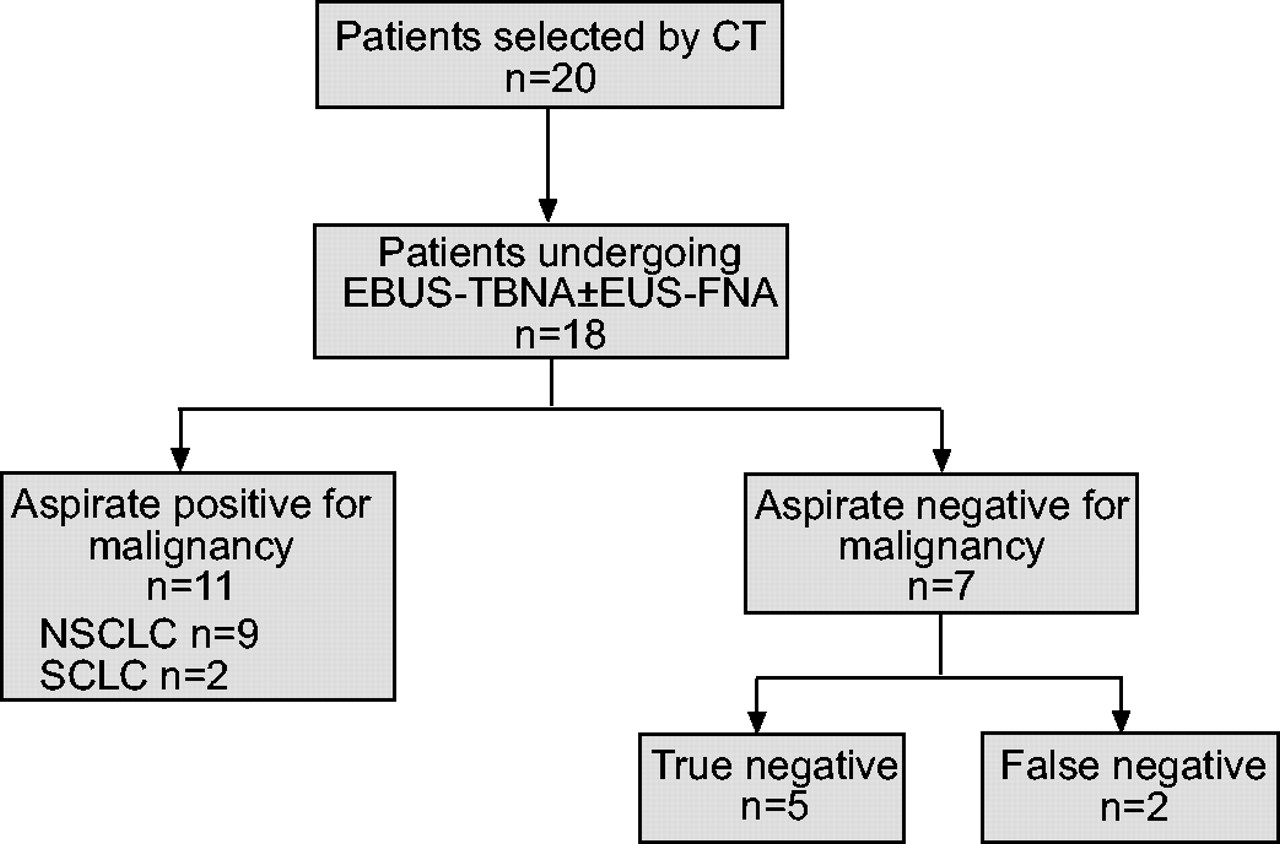
Diagnostic outcome for patients with suspected lung cancer with enlarged mediastinal lymph nodes on computed tomography (CT) who underwent endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA)±endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA). NSCLC: nonsmall cell lung cancer; SCLC: small cell lung cancer.
1 Details of the indications, lesions targeted, cytology and outcomes of patients undergoing endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) alone or combined procedures
EBUS-TBNA was used to sample 26 lymph nodes from 17 patients: 10 in station 7, nine in station 4R, four in station 3, two in station 10R, and one in station 2R (table 1⇑). Lymph node size ranged 6–20 mm in short-axis diameter. In one further patient, a peri-bronchial mass lesion was aspirated. The mean number of passes per lesion was two (range 1–3). A positive cytological diagnosis showing node (N)2 or N3 disease was achieved in 11 of the 18 cases that underwent EBUS-TBNA. Of these, nine showed nonsmall cell lung cancer and two showed small cell lung cancer (SCLC). In eight of the 18 patients, EBUS-TBNA gave a primary tissue diagnosis. Of the 11 patients who were shown to have N2/N3 disease, 10 were treated with chemotherapy.
In five patients, EBUS-TBNA cytology from lymph nodes was negative for malignancy, although lymphocytes were present in all specimens confirming accurate targeting. In four of these cases, subsequent surgical staging did not reveal any malignant lymph node involvement and final staging was pathological tumour (pT)2N0/1 or sarcoidosis (one case). In the fifth case, CT scanning has shown no disease progression after 1 yr. The EBUS-TBNA results of these five cases were recorded as true negative (i.e. correct assessment of N2/N3 nodes for malignancy).
In two cases, EBUS-TBNA showed no evidence of malignancy, although the final diagnosis was that of carcinoma. In one case, in which a peribronchial mass lesion was aspirated, a subsequent thoracotomy revealed pT4N1 adenocarcinoma, although prior mediastinoscopy had also been negative for malignancy. In the other case, EBUS-TBNA and EUS-FNA of multiple lymph nodes were negative for malignancy, as was subsequent mediastinoscopy. However, at thoracotomy, a microfocus of malignancy was found in a single 4R node. The EBUS-TBNA result for these cases was, therefore, recorded as false negative.
In addition to the combined case noted earlier, five other patients also underwent EUS-FNA in conjunction with EBUS-TBNA, and additional findings attributable to EUS were noted in all cases. In one case, EUS-FNA revealed malignant involvement of lymph nodes in station 5, as well as a small malignant para-oesophageal mass lesion deep to the subcarinal nodes invading the pleura, which had not been seen by EBUS or on CT scanning. Following the combined procedure, the final staging for this case was T3N2. In two patients, postero-inferiorly placed subcarinal lymph nodes, inaccessible by EBUS-TBNA, were sampled and shown to be malignant. In two cases, EUS-FNA examination of stations 5, 7, 8 and 9 lymph nodes were negative (as were all nodes sampled by EBUS-TBNA), and the resection specimens were staged pT2N0 and pT2N1, respectively, i.e. the EBUS/EUS examinations were true-negative results.
One patient each underwent EBUS alone and combined EBUS/EUS, respectively, but did not have FNA performed. In one case, the CT scan had shown isolated mediastinal lymphadenopathy, and EBUS revealed lymph nodes containing pale-looking fatty centres, suggesting a benign appearance. However, due to intervening vascular structures, an aspirate was not performed. The patient remains well 6 months later, and repeat CT scans have shown regression of the lymphadenopathy that was thought to have been due to infection. In one patient known to have adenocarcinoma in the left upper lobe but no evidence of mediastinal lymphadenopathy on the CT scan, combined EBUS/EUS revealed only very small lymph nodes (3–5 mm), which were not amenable for aspiration. Subsequent resection confirmed pT3N0.
The mean duration of procedure for EBUS, including systematic identification of each lymph node group and TBNA of selected lesions, was 30 min, and, for combined EBUS and EUS examinations, the mean duration was 45 min. Patients tolerated both the EBUS-TBNA and the combined procedures well, and a complete examination was possible in all cases. None of the procedures was required to be terminated prematurely due to patient intolerance, and there were no periprocedural complications.
For the 18 patients who underwent EBUS-TBNA, the sensitivity, specificity and accuracy were 85% (95% confidence interval (CI) 54.6–98.1), 100% (95% CI 47.8–100) and 89% (95% CI 65.3–98.6), respectively.
DISCUSSION
Pathological evaluation of mediastinal lymph nodes in lung cancer is essential in order to accurately stage patients and plan management. In this report, it has been demonstrated that real-time EBUS-guided TBNA can be used to identify and aspirate lymph nodes adjacent to the trachea and main bronchi from lymph node stations 2, 3, 4, 5, 7, 10 and 11. Furthermore, under local anaesthetic and conscious sedation, EBUS can be combined with EUS, which allows access to the postero-inferior lymph node stations 5, 7, 8 and 9. Therefore, the combined use of EBUS and EUS offers the potential of more comprehensive access to mediastinal and hilar lymph nodes than is usually accessible by mediastinoscopy.
Prior to the development of real-time EBUS-TBNA bronchoscopy, TBNA has been limited to “blind” needle puncture guided by static CT scans. This technique is highly operator dependent, and sensitivity varies between 20% and 89% 7–9. Yield is improved with at least seven passes of the TBNA needle and on-site cytopathology 10. More recently, Herth et al. 11 have demonstrated that a mechanical radial ultrasound mini-probe, introduced through the working channel of a flexible bronchoscope, can be used to localise target lymph nodes prior to sequential blind biopsy. By this method, sampling sensitivity rate rose to 86% 11. While this technique has improved TBNA yields, it does not allow ultrasound-guided control of needle puncture, and inadvertent puncture of vascular structures is a risk. Using real-time ultrasound-guided FNA, the current authors have achieved a sensitivity rate of 85% and an overall accuracy of 89%. Although these results should be regarded as preliminary due to the small numbers of patients involved, the sensitivity and accuracy are similar to those obtained by others using EBUS-TBNA 12, 13 and also in EUS-FNA series 14–16. Furthermore, the EBUS-TBNA results are for the first 20 cases performed in the current authors' institution using this method, indicating that a high sensitivity and accuracy rate can be obtained with relatively limited experience of the technique. The ability to be able to guide the needle into lesions under real-time control allows not only accurate sampling of lesions <1 cm in diameter, but also targeting of lesions in difficult locations. Lesions <1 cm are generally regarded as difficult to target using conventional “blind” techniques. Furthermore, the number of passes required to successfully acquire tissue for cytological analysis is reduced, which increases safety and saves time.
The utility of real-time EBUS-TBNA is illustrated by the case of a patient who presented with an autonomic neuropathy that was thought to be due to a paraneoplastic syndrome. CT scanning showed a pair of 7-mm lesions in the lung parenchyma, which were not amenable to CT-guided needle biopsy and beyond the reach of a conventional bronchoscope (fig. 3a⇓). A solitary 1-cm lymph node lying anterior to the trachea was identified on the CT scan, and EBUS-TBNA revealed SCLC (fig. 3b–d⇓). Diagnosis using EBUS-TBNA avoided the need for mediastinoscopy and allowed chemotherapy to be commenced the following day. In this series, EBUS provided a primary tissue diagnosis in eight of the 20 patients examined and avoided the need for a staging mediastinoscopy in 11 cases.

{kind=link}
{kind=link}
{kind=link}
a) Computed tomography (CT) image showing two small primary lesions (arrows), which were inaccessible for biopsy by percutaneous or standard bronchoscopic techniques. b) CT image showing a solitary lymph node (arrow) lying anterior to the trachea in lymph node station 4R. c) Endobronchial ultrasound image of the same lymph node as in b) (arrows), showing the needle lying within the node. d) Fine-needle aspirate cytology specimen of the lymph node showing small cell lung cancer. Scale bar = 10 μm.
Despite the potential utility of these techniques for upstaging patients, the possibility of false-negative cytology with FNA remains, and it is recognised that some patients may still require a surgical staging procedure prior to definitive surgery. Further larger, randomised, controlled trials examining whether combined EBUS-TBNA and EUS-FNA are as accurate at staging the mediastinum as surgical techniques are required.
However, it is believed that endobronchial ultrasound-guided transbronchial needle aspiration and endoscopic ultrasound-guided fine-needle aspiration are complimentary, with endobronchial ultrasound having better access to anterior and superior mediastinal lymph nodes and endoscopic ultrasound having better access to posterior and inferior lymph nodes. It is envisaged that a logical approach for evaluation of the mediastinum would be for patients to undergo standard bronchoscopy and/or endobronchial ultrasound-guided transbronchial needle aspiration and/or endoscopic ultrasound-guided fine-needle aspiration guided by results from prior computed tomography/positron emission tomography scanning. This “one-stop” approach would potentially minimise the number of procedures that the patient has to undergo whilst staging the mediastinum to the highest level. This strategy would also be particularly useful for patients who are medically unfit for surgical diagnostic procedures. Although the current authors have not performed an economic evaluation of such an approach versus mediastinoscopy, previous work comparing endoscopic ultrasound-guided fine-needle aspiration with mediastinoscopy favoured the nonsurgical arm, and it is anticipated this would be the case with combined endobronchial ultrasound/endoscopic ultrasound approaches too 17.
Acknowledgments
The authors wish to thank J. Wilson, J. Matthews and H. Chisholm of the Endoscopy Unit at the Royal Infirmary of Edinburgh, Edinburgh, UK, for their help with this study.
Footnotes
-
For editorial comments see page 400.
- Received August 14, 2004.
- Accepted November 12, 2004.
- © ERS Journals Ltd
References









