





Abstract
Idiopathic pulmonary arterial hypertension (IPAH) is a pulmonary vasculopathy of unknown aetiology. Dyspnoea, peripheral airway obstruction and inefficient ventilation are common in IPAH. Data on respiratory muscle function are lacking.
This prospective single-centre study included 26 female and 11 male patients with IPAH in World Health Organization functional classes II–IV. Mean±sd pulmonary artery pressure was 48.6±16.9 in females and 53.1±22.9 mmHg in males; cardiac output was 3.7±1.3 and 4.2±1.7 L·min−1.
Maximal inspiratory pressure (PI,max) was lower in the female patients than in 20 controls (5.3±2.0 versus 8.2±2.0 kPa). In the male patients, PI,max was lower than in 25 controls (6.8±2.2 versus 10.5±3.7 kPa). Maximal expiratory pressure (PE,max) was lower in the female patients than in controls (6.2±2.6 versus 9.5±2.1 kPa), and in male patients as compared to controls (7.1±1.6 versus 10.3±3.9 kPa). There was no correlation between PI,max or PE,max and parameters of pulmonary haemodynamics or exercise testing. The ratio of mouth occlusion pressure within the first 0.1 s of inspiration and PI,max was higher in IPAH than in controls (females 0.067±0.066 versus 0.021±0.008; males 0.047±0.061 versus 0.023±0.016).
In conclusion, this study provides the first evidence of inspiratory and expiratory muscle weakness in idiopathic pulmonary arterial hypertension. The pathomechanisms and the prognostic significance should be further investigated.
Idiopathic pulmonary arterial hypertension (IPAH) is defined as a pulmonary vasculopathy of unknown aetiology, predominantly affecting females 1. Minute ventilation (V′E) is increased at rest and during exercise 2. The ventilatory response to exercise in IPAH patients, i.e. the ratio of V′E to carbon dioxide production (V′CO2) during exercise (V′E/V′CO2 slope), is also increased and is a predictor of poor prognosis 2, 3. The increased V′E/V′CO2 slope indicates inefficient ventilation in IPAH, which can partly be attributed to pulmonary-perfusion abnormalities 2. It has been shown by the current authors' group and others that, in congestive left ventricular failure, inefficient ventilation is associated with reduced inspiratory muscle strength 4–6. Moreover, inspiratory muscle function has recently been identified as a prognostic predictor in congestive left ventricular failure 7. Risk stratification of patients with congestive left ventricular failure is improved by using the combination of maximal inspiratory pressure (PI,max) and peak oxygen consumption (V′O2) 7.For editorial comments see page 6.
Inspiratory and expiratory muscle strength have not been studied in IPAH. Therefore, this prospective study investigated respiratory muscle function and the mouth occlusion pressures in 37 patients with IPAH. PI,max and maximal expiratory pressure (PE,max) were prospectively assessed in IPAH patients with varying degrees of disease and exercise limitation. Moreover, invasive (right heart catheterisation) and noninvasive (6-min walking test (6MWT), cardiopulmonary exercise test) parameters of disease severity were evaluated 1, 2.
MATERIALS AND METHODS
Study subjects
This prospective study was conducted in a university tertiary referral centre (Dept of Cardiology and Respiratory Medicine, Heidelberg, Germany) for patients with pulmonary hypertension, and included 26 female and 11 male patients 1. The diagnosis of IPAH was made after ventilation–perfusion scan, spiral computed tomography, three-dimensional-angiography magnetic resonance tomography, or pulmonary angiography to rule out any pulmonary embolic aetiology, and exclusion of any underlying autoimmune disease, collagenous vascular disease, hepatic or HIV infection, and nocturnal deoxygenation.
Patients included in the study showed no clinical or radiological signs of cardiopulmonary decompensation, concomitant left heart disease or other pulmonary disease.
The study was approved by the local ethics committee and was in accordance with the recommendation found in the Helsinki Declaration 8. Patients gave written informed consent.
Haemodynamic measurements
During right heart catheterisation at rest, it was not possible to obtain reliable pulmonary capillary wedge pressures in all patients. Therefore, total pulmonary vascular resistance (TPVR) was calculated from mean pulmonary artery pressure (MPAP) divided by cardiac output.
Pulmonary and respiratory muscle function testing
Vital capacity (VC), forced expiratory volume in one second (FEV1), total airway resistance (Rtot), single-breath carbon monoxide diffusing capacity (DL,CO) and mouth pressures were determined with the patients sitting upright and breathing through a flanged mouthpiece inside the lips (MasterLabPro 4.2; Jaeger, Würzburg, Germany) 9–11. In brief, PI,max was determined during a deep inspiration from functional residual capacity against a shutter with a minor air leak preventing undesirable glottis closure. PE,max was measured during maximal expiratory effort at total lung capacity. PI,max and PE,max were determined from the best of five consecutive manoeuvres (varying <20%). A total of 2 min of rest was allowed between two manoeuvres when necessary. Mouth occlusion pressure 0.1 s after the onset of inspiration (P0.1) was measured during spontaneous breathing at rest. PI,max and P0.1 are negative pressures with respect to atmosphere, but are expressed as positive values. The P0.1/PI,max ratio was calculated to prevent underestimation of neural respiratory drive due to weakness of the inspiratory musculature 12, 13.
Spirometry results were compared with predicted normal values (VC, FEV1) 9. Since published reference values for PI,max, PE,max and P0.1 vary 10, 11, values determined in 20 female and 25 male healthy subjects served as controls. Other variables that have been shown to determine PI,max and PE,max (e.g. body surface area) did not differ between the patients and the control subjects 14.
For blood gas analysis, arterialised capillary blood samples were taken from the hyperaemic ear lobe with the patient at rest 15.
Exercise testing
During the symptom-limited exercise testing, work load was increased following a ramp protocol on a bicycle ergometer with the patient in a semi-supine position 5. V′E, V′O2 and V′CO2 were continuously monitored and averaged online from eight consecutive breaths (OxyconAlpha; Jaeger). Ventilatory efficiency was estimated from the slope V′E/V′CO2 over the linear part 16.
The results of the 6MWT were counted from the laps achieved on a 60-m course in a straight hospital hallway that was seldom used. The test equipment and the interaction with the patient were provided as recommended 17.
Data analysis
All results are expressed as mean±sd. Unpaired t-test and linear regression analysis were used as appropriate 18. A level of p<0.05 was accepted as statistically significant.
RESULTS
Pulmonary haemodynamics
At right heart catheterisation, all patients showed moderate-to-severe pulmonary hypertension (table 1⇓).
Haemodynamic and cardiopulmonary exercise characteristics in 26 female and 11 male patients with idiopathic pulmonary arterial hypertension
Lung volumes, diffusion and arterial blood gases
VC and FEV1 were within normal limits in both groups, i.e. ±20% of predicted (tables 2⇓ and 3⇓). VC was lower in IPAH patients than in controls (tables 2⇓ and 3⇓), and Rtot was not increased. The maximal expiratory flow at 50% of the expired VC was decreased in IPAH patients (tables 2⇓ and 3⇓).
Pulmonary function in 26 female patients with idiopathic pulmonary arterial hypertension(IPAH) and 20 controls
Pulmonary function in 11 male patients with idiopathic pulmonary arterial hypertension(IPAH) and 25 controls
In IPAH patients, blood gas analysis at rest showed compensated respiratory alkalosis (pH 7.44±0.04 in female and 7.45±0.05 in male patients), hypocapnia (carbon dioxide arterial tension (Pa,CO2) 4.3±0.8 and 4.3±0.9 kPa, respectively), and hypoxaemia (8.7±1.8 and 8.8±1.9 kPa, respectively).
Pronounced hypoxaemia, i.e. arterial oxygen tension <7.9 kPa (<60 mmHg), was present in 12 female patients (46%) and six male patients (55%). None of the patients was hypercapnic. In contrast, Pa,CO2 was reduced to <4.7 kPa (<35 mmHg) in 17 female patients (65%) and eight male patients (75%).
Dl,co was reduced in female and male IPAH patients to 64.3±18.8 and 75.0±26.8% predicted, respectively.
Cardiopulmonary exercise testing
During cardiopulmonary exercise testing, work load and peak V′O2 were reduced in IPAH patients, indicating exercise intolerance. Moreover, the ventilatory equivalents for O2 (V′E/V′O2) and CO2 (V′E/V′CO2) at rest (table 1⇑) increased during exercise to V′E/V′O2 52.7±18.6 and V′E/V′CO2 to 53.5±15.9 in female patients and to V′E/V′O2 49.5±21.8 and V′E/V′CO2 50.4±19.0 in male patients, respectively. Moreover, the ventilatory response to exercise (V′E/V′CO2 slope) was increased in female and male patients (table 1⇑).
In female patients with a peak V′O2 below the median (13.8 mL·min−1·kg body weight−1), the V′E/V′CO2 slope was significantly steeper (58.5±17.2) than in patients with a peak V′O2 ≥34.4±4.7 (p = 0.002). Similarly, in male IPAH patients with a peak V′O2 below the median of 12.5, the V′E/V′CO2 slope was increased (62.6±20.5 versus 37.4±7.5; p = 0.032). This indicates that inefficient ventilation was associated with exercise intolerance.
Mouth occlusion pressures
In IPAH patients, PI,max and PE,max were significantly lower as compared with their respective controls (figs 1a⇓ and b). Both parameters showed a linear correlation in female patients (fig. 2⇓), female controls (r = 0.56; p = 0.019), male patients (r = 0.78; p = 0.012) and male controls (r = 0.61; p = 0.002). The reduction in PI,max and PE,max was independent from pulmonary haemodynamics, lung mechanics, DL,CO, blood gases, exercise capacity, ventilatory efficiency or 6MWT by linear regression analysis. PI,max and PE,max did not differ between World Health Organization (WHO) functional classes. In two patients with reduced body mass index (14.3 and 17.0 kg·m−2, respectively), PI,max was reduced to 6.9 and 5.6 kPa, respectively, and PE,max was reduced to 6.8 and 6.6 kPa, respectively.
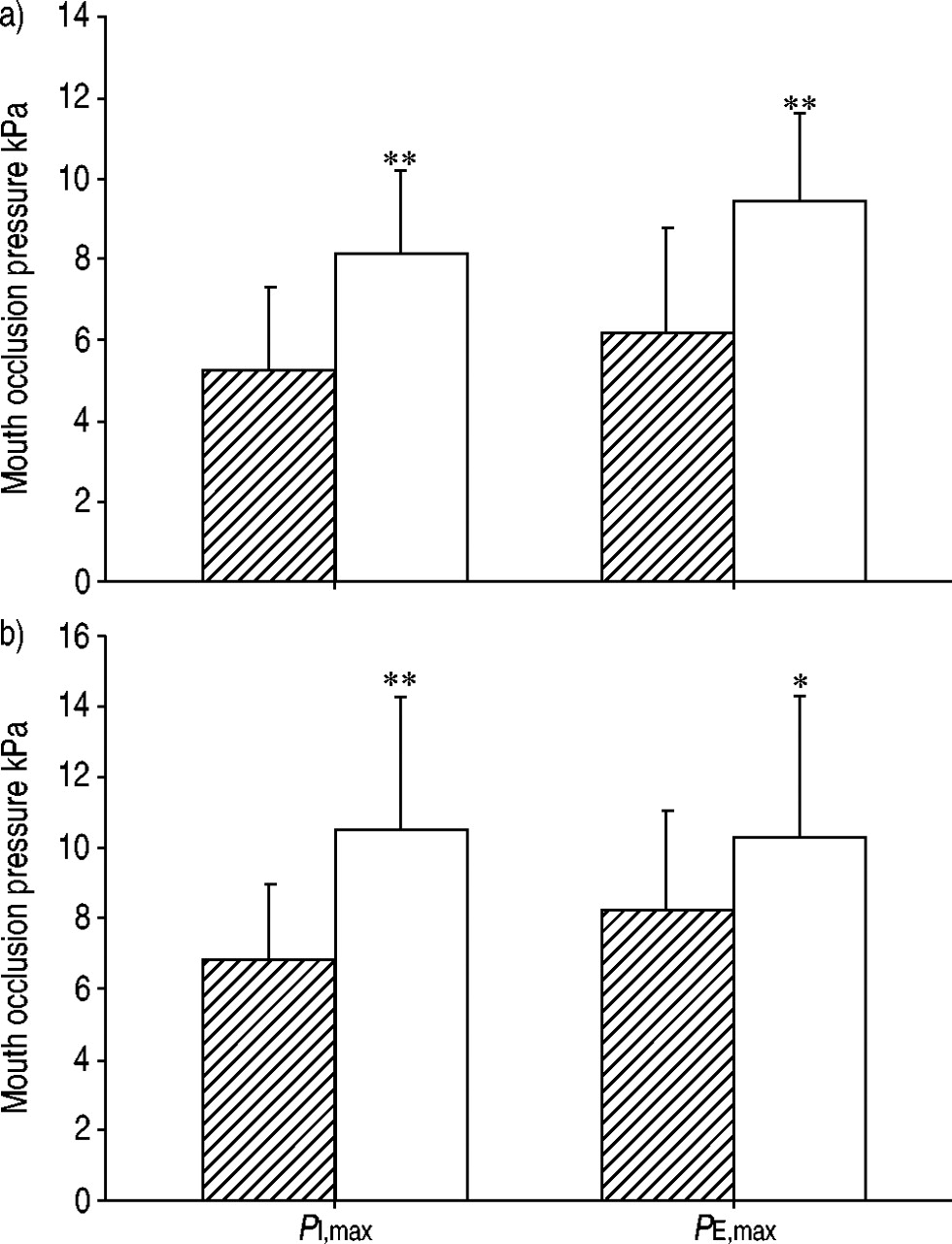
a) Maximal inspiratory (PI,max) and expiratory pressure (PE,max) in 26 female patients with idiopathic pulmonary arterial hypertension (IPAH; └) as compared with 20 female controls (□). b) PI,max and PE,max in 11 male patients with IPAH (└) as compared with 25 male controls (□). Data are presented as mean±sd. *: p<0.05; **: p<0.01.

Correlation between maximal expiratory (PE,max) and inspiratory pressure (PI,max) in female patients with idiopathic pulmonary arterial hypertension (r = 0.73; p<0.01).
Mouth occlusion pressure within the first 0.1 s of inspiration (P0.1) tended to be higher in IPAH than in controls, without reaching statistical significance, in female patients (0.24±0.19 versus 0.20±0.12 kPa) and in male patients (0.28±0.27 versus 0.21±0.14 kPa), respectively.
The ratio P0.1/PI,max was significantly higher in female IPAH patients than in controls (0.062±0.066 versus 0.021±0.008 kPa; p<0.01). In male patients, P0.1/PI,max tended to be higher than in controls, without reaching statistical significance (0.047±0.061 versus 0.023±0.016 kPa; p = 0.07). There was a significant correlation between the ratio P0.1/PI,max and V′E/V′CO2 slope (fig. 3⇓).

{kind=link}
{kind=link}
{kind=link}
Correlation between mouth occlusion pressure within the first 0.1 s of inspiration (P0.1)/maximal inspiratory pressure (PI,max) and minute ventilation (V′E)/carbon dioxide production (V'CO2) slope in female patients with idiopathic pulmonary arterial hypertension (r = 0.78; p<0.01).
DISCUSSION
The present study provides the first evidence of respiratory muscle dysfunction in IPAH, as follows: 1) both inspiratory and expiratory muscle strength (PI,max and PE,max) are reduced in patients with IPAH as compared with respective controls; 2) inspiratory and expiratory muscle weakness occurs independently from pulmonary haemodynamics, exercise capacity or ventilatory inefficiency.
Patients' characteristics
The pulmonary vascular disease in the present patients is of varying severity, as determined by WHO functional classes, 6MWT, peak V′O2 or pulmonary haemodynamics 1, 2. Lung mechanics at rest are within the predicted normal range, except for a mild reduction in VC, FEV1 and in end-expiratory airflow, as described previously 19. During lung function and exercise testing, the supine position was avoided, since this position induced an increase in airflow resistance, an aggravated expiratory flow limitation and a decrease in lung compliance in patients with left ventricular failure 20–22. In IPAH patients, the effects of assuming a supine position have not been investigated so far.
Hypocapnia and compensated respiratory alkalosis at rest are compatible with hyperventilation. The present hypoxaemia and the reduced diffusion capacity indicate impaired pulmonary diffusion. Moreover, ventilation is inefficient in IPAH at rest and worsens even further during exercise, as indicated by an increase in V′E/V′O2 and V′E/V′CO2 at rest, which is more pronounced during exercise. This is in unison with the increased V′E/V′CO2 slope, an indicator of inefficient ventilation, disease severity and unfavourable prognosis in IPAH 2, 3. It can be hypothesised that the present ventilatory inefficiency is partially compensated by increased V′E at rest and during exercise 2. However, increased ventilation might contribute to the stress on the respiratory muscles 23, 24.
Respiratory muscle weakness
The present reduction in PI,max in IPAH is in accordance with a 28% reduction of PI,max in 245 patients with congestive left ventricular failure observed by the current authors and others 5, 7, 25, 26. There are, however, marked differences between the changes in IPAH and in congestive left ventricular failure: in IPAH, changes in PI,max and PE,max are independent from haemodynamic and clinical parameters, such as MPAP, TPVR, 6MWT, WHO functional class and peak V′O2. In contrast, in congestive left ventricular failure, the reduction in PI,max is closely associated with functional parameters, including New York Heart Association (NYHA) functional class or peak V′O2 7. Moreover, in congestive left ventricular failure, the reduction in PI,max exceeds the reduction in PE,max 5, 7, 26, whereas, in the present IPAH patients, there is a close correlation between PI,max and PE,max. This is in concert with the parallel reduction in inspiratory and expiratory pressures seen in chronic obstructive pulmonary disease (COPD) patients 27.
The underlying mechanisms responsible for the respiratory muscle weakness in the present IPAH patients are not known and were not the main focus of the present study. However, for COPD and left heart failure, various mechanisms leading to a reduction in respiratory muscle strength have been suggested. These include the reduced cross-sectional area of all types of fibres of the diaphragm and ribcage muscles 28, type I fibre atrophy and changes in the type I and type IIb fibre ratio in the diaphragm 29, 30, the reduced number of actin–myosin cross-bridges in the diaphragm 31, and abnormal intracellular Ca2+ profiles 32. However, so far, none of these mechanisms has been addressed in right heart failure due to pulmonary hypertension. This also applies for potential mechanisms leading to respiratory muscle dysfunction: impaired muscle perfusion 6, 33, decrease in number and size of mitochondria 34, and decreased oxidative enzymes 35. Electrolyte disturbances 36 and steroid therapy 37 have been identified to play a role in the development of inspiratory and expiratory muscle weakness. However, the present IPAH patients had no electrolyte status abnormality or steroid therapy. In congestive left heart failure, malnutrition, wasting and “cardiac cachexia” lead to atrophic loss of the skeletal muscle bulk and may contribute to respiratory muscle weakness 38. In two of the present IPAH patients with reduced respiratory muscle strength, a reduced body mass index indicated malnutrition.
In COPD patients, inspiratory muscle strength improved after lung transplantation. However, weakness of the expiratory muscles and ankle dorsiflexors persisted, suggesting that these muscle groups are vulnerable to some factor that does not affect the diaphragm or because the diaphragm is constantly active 23, 39. Activation of the inspiratory muscles, including the diaphragm, is promoted by the ventilatory or central neural drive, which can be assessed indirectly by the measurement of P0.1. In the present IPAH patients, the increased P0.1/ PI,max at rest indicates augmented ventilatory drive.
Controversially, it can be disputed whether this is a consequence of respiratory muscle weakness in IPAH or a contributing cause of it, i.e. chronic “overload” of respiratory musculature. In patients with congestive left heart failure, respiratory muscle function was improved by unloading respiratory muscles with noninvasive continuous positive airway pressure ventilation 40 or, conversely, by selective respiratory muscle training 41. Future studies in IPAH should evaluate the prognostic impact of these therapeutical interventions.
Clinical implications and conclusions
This study provides the first evidence of significant inspiratory and expiratory muscle weakness in idiopathic pulmonary arterial hypertension. The underlying pathomechanisms, the response to treatment and a potential role as a prognostic marker of the present respiratory muscle dysfunction need further investigation.
Acknowledgments
N.B. Pride (National Heart and Lung Institute, London, UK) is gratefully acknowledged for his most valuable discussions. C. Seitz, I. Hillenbrand and M. Schwertfeger are acknowledged for expert technical assistance.
- Received August 15, 2004.
- Accepted August 20, 2004.
- © ERS Journals Ltd
References









