





Figures
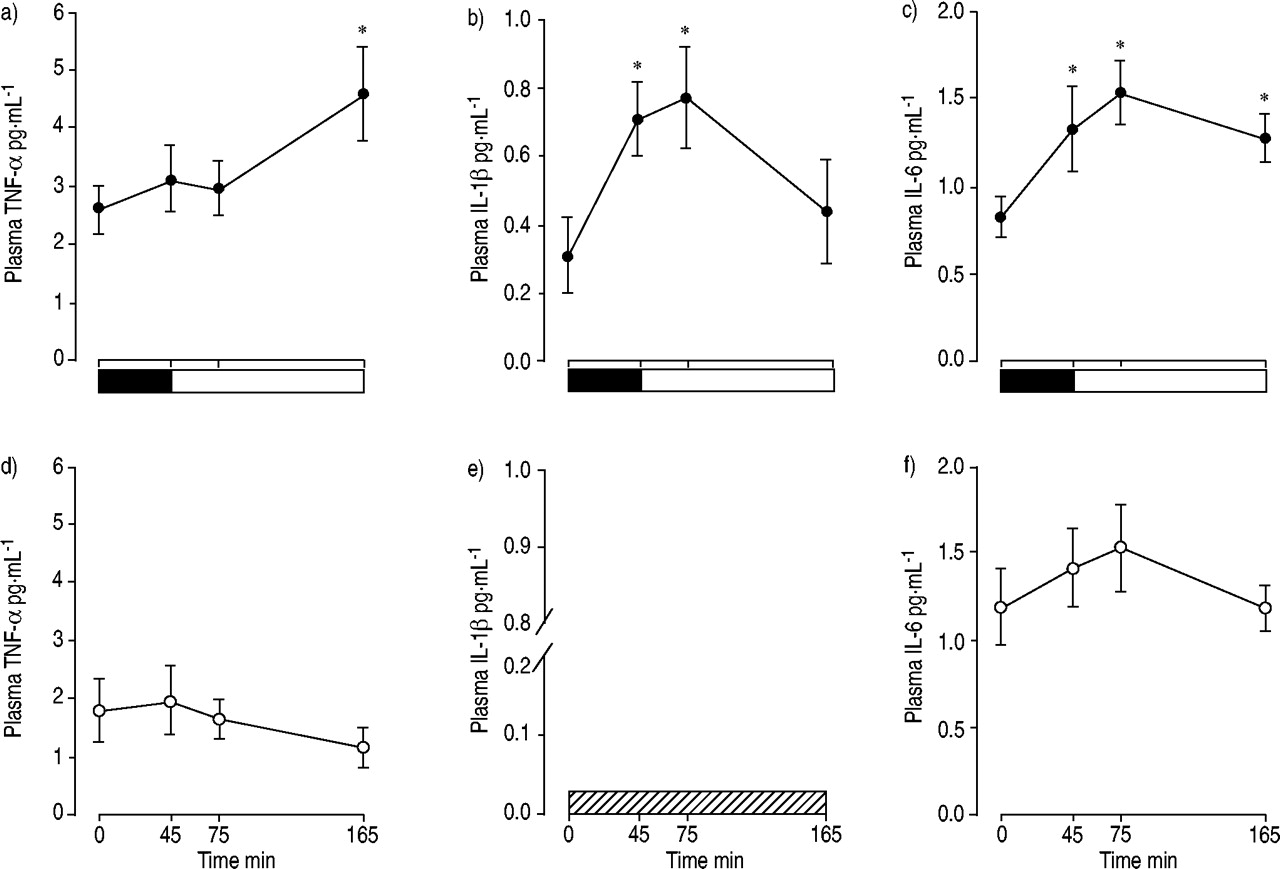
- Fig. 1.—
The plasma cytokine response to resistive breathing before (•; a, b and c) and after (○; d, e and f) antioxidants. The mean plasma tumour necrosis factor (TNF)-α (a and d), interleukin (IL)-1β (b and e), and IL-6 concentrations (c and f) before the resistive breathing session (0 min), at the end of resistive breathing (▪: load; 45 min), and 30 and 120 min after the end of resistive breathing (□: recovery; i.e. 75 min and 165 min after the beginning of the resistive breathing session) were recorded. The plasma IL-1β was below detection limit after antioxidant supplementation (└; e). *: p<0.05 compared with baseline values (0 min). Modified from 6 with permission.
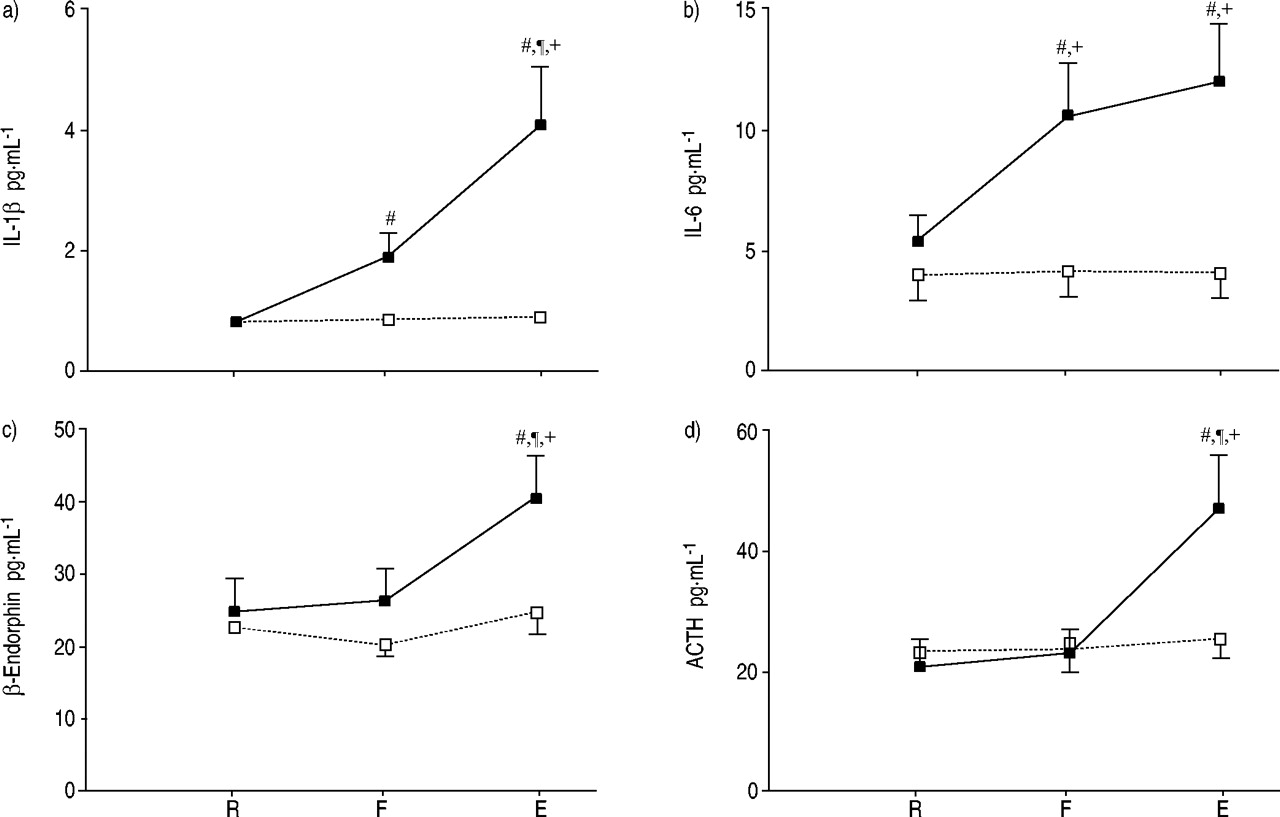
- Fig. 2.—
The plasma cytokine and hypothalamic pituitary responses to resistive breathing. Mean plasma level of interleukin (IL)-1β (a), IL-6 (b), β-endorphin (c) and adrenocorticotropin hormone (ACTH; d) at rest (R), at the point where the subjects could not generate the target maximum inspiratory pressure (75% of maximum, 45 min after the beginning of resistive breathing; F), and at the end of resistive breathing (15 min later, at 60 min from the beginning; E). From F to E, subjects were put through an alinear resistance to the maximum they could achieve. Data are presented as mean±sem. ▪: high-load run; □: moderate-load run. #: statistically significant difference (p<0.05) from R; ¶: statistically significant difference (p<0.05) from F; +: statistically significant difference (p<0.01) from the moderate-load run. Modified from 5 with permission.
- Fig. 3.—
Effect of tumour necrosis factor (TNF)-α on diaphragmatic contractility. a) TNF-α depresses diaphragm force. Diaphragm fibre bundles treated with TNF-α 500 ng·mL−1 (○) developed lower forces than paired controls (•) at all stimulus frequencies (p<0.001). Data are presented as mean±sem. P0: maximal tetanic force. n=8 per group. b) TNF-α stimulates loss of force in single fibres. Values depict mean rates of force decline (%·h−1) measured by regression analysis using data from individual experimental fibres (n=5) before and after exposure to TNF-α 500 ng·mL−1. TNF-α accelerated the loss of force in each of five fibres studied (p<0.02). c, d) Depression of tetanic force transients by TNF-α. Individual tracings obtained from intact single fibres stimulated at 80 Hz before (––––) and after (……) 4-h incubation in either buffer alone (control fibre; c) or in TNF-α 500 ng·mL−1 (experimental fibre; d). e, f) Insensitivity of tetanic intracellular calcium ion concentration ([Ca2+]i) transients to TNF-α. Individual tracings obtained from intact single fibres stimulated at 80 Hz before (––––) and after (•;) 4-h incubation in either buffer alone (control fibre; e) or in TNF-α 500 ng·mL−1 (experimental fibre; f). Modified from 43 with permission.
- Fig. 4.—
Cytokines stimulate the hypothalamic pituitary adrenal axis. a) Changes in plasma concentration of adrenocorticotropin ([ACTH]) in capsaicin-desensitised (└; n=6) and control (□; n=6) groups after i.v. injection of interleukin (IL)-1β (2 µg·kg−1; arrow). *: p<0.05; ***: p<0.001. Modified from 68 with permission. Plasma immunoreactive ACTH (b) and cortisol (c) responses to a s.c. bolus injection of IL-6 (30 µg·kg−1). The grey areas represent the mean±sd responses of healthy normal volunteers to a standard bolus dose (1 µg·kg−1) of corticotrophin-releasing hormone and were included for comparison. Modified from 69 with permission.
- Fig. 5.—
Endorphins and resistive loading. The tidal volume (VT) response of unanaesthetised goats to 2.5 h of high inspiratory flow-resistive loading prior to and following the administration (open arrow) of naloxone (•) or saline (○). VT, which fell considerably after loading (shallow breathing), increased after naloxone administration, while saline had no effect. These data indicate that inspiratory resistive loading activates the endogenous opioid system, and that the reduction of VT in response to loading is partly mediated by β-endorphins. Data are presented as mean±sem. Modified from 76 with permission.
- Fig. 6.—
Integrated view of the origin and functional consequences of resistive breathing-induced cytokines. Resistive breathing results in the generation of oxidative stress and the induction of cytokines within the diaphragm, secondary to the increased muscle activation. Oxidative stress is a major stimulus for this cytokine induction. Tumour necrosis factor (TNF)-α compromises diaphragmatic contractility and contributes to the development of muscle cachexia. Interleukin (IL)-6 attenuates the TNF-α expression, secondary to strenuous diaphragmatic contraction. IL-6 mobilises glucose from the liver and free fatty acid (FFA) from the adipose tissue, which increases the energy available to the strenuously working respiratory muscles. At the same time, cytokines stimulate the hypothalamic-pituitary-adrenal axis either haematogenously or via stimulation of small afferent nerve fibres, leading to production of adrenocorticotropin (ACTH) and β-endorphins. The ACTH response may represent an attempt of the organism to reduce the injury occurring in the respiratory muscles through the production of glucocorticoids by the adrenals and the induction of the acute phase-response proteins. The β-endorphin response would decrease the activation of the respiratory muscles and change the pattern of breathing, which becomes more rapid and shallow, possibly in an attempt to reduce and/or prevent further injury to the respiratory muscles. POMC: pro-opiomelaninocortin; ROS: reactive oxygen species; TG: triglycerides.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}









