





Abstract
Exposure to organic dust in a swine house causes acute airway inflammation and increased bronchial responsiveness to methacholine in healthy subjects. The aim of this study was to investigate whether an inhaled glucocorticoid, fluticasone propionate, alters the acute airway responses induced by exposure in a swine barn.
In 15 healthy subjects, analysis of nasal lavage fluids, serum samples and bronchial methacholine responsiveness were performed before and after exposure to organic dust in a swine house for 3 h. Seven subjects received fluticasone propionate (500 µg b.i.d. by inhalation and 100 µg intranasally once daily) and eight subjects received placebo during the 2 weeks prior to exposure.
Post-exposure plasma interleukin (IL)-6 levels and body temperature were significantly lower in the fluticasone group than in the placebo group. Intranasally administered fluticasone propionate significantly attenuated the plasma protein (assessed as albumin concentrations) leakage and IL-8 and tumour necrosis factor-α response induced by exposure. Fluticasone propionate inhalation exerted no influence on the increased bronchial responsiveness to methacholine induced by exposure.
In conclusion, glucocorticoid treatment attenuated the inflammatory response to inhaled organic dust without influencing the increased bronchial responsiveness to methacholine.
This study was supported by Glaxo Smith Kline (Greenford, UK) and the Swedish Council for Work Life Research, the Swedish Farmers' Foundation for Agricultural Research, the Swedish Heart Lung Foundation and the Karolinska Institute (all Stockholm, Sweden).
Exposure in a swine confinement building for 3 h causes increased airway responsiveness and a massive influx of inflammatory cells into the airways in healthy subjects 1–3. In bronchoalveolar lavage (BAL) fluid, a 75-fold increase in neutrophil numbers, more than doubling of alveolar macrophage numbers and a three-fold increase in lymphocyte numbers have been found following exposure 1, 2, 4. In addition, the concentrations of pro-inflammatory cytokines (tumour necrosis factor (TNF)-α and interleukin (IL)-6 and IL-8) are elevated in nasal fluid and BAL fluid following exposure to swine dust 2, 4, 5. Inhalation of swine dust also causes leakage of plasma proteins into the airways, as assessed by increased levels of α2-macroglobulin, transferrin and albumin in BAL fluid 6. Exposure in swine barns also induces systemic effects, such as increased body temperature and increased plasma levels of acute-phase proteins and IL-6 1.
Glucocorticoids yield anti-inflammatory effects by modulating gene expression, mediated through the glucocorticoid receptor 7. An important part of the anti-inflammatory effects of glucocorticoids is repression of inflammatory mediators, particularly cytokines, and inhibition of inflammatory cell migration 8. It has previously been shown that fluticasone propionate almost totally inhibits swine-dust-induced IL-6 and IL-8 release from epithelial cells in vitro 9. Additionally, the inhibition by fluticasone propionate of the dust-induced IL-6 and IL-8 release from epithelial cells is, in part, mediated by inhibition of nuclear factor (NF)-κB activation 10. However, the precise molecular mechanism of glucocorticoid action is unclear in this context.
Glucocorticoids are thus capable of influencing different indices of the inflammatory process. In addition to the beneficial effects in asthma, inhaled glucocorticoids are also a remedy for other inflammatory airway diseases, such as severe chronic obstructive pulmonary disease. It is, however, not clear whether or not this treatment alters the airway responses to heavy exposure to organic dust. The aim of the present study was, therefore, to investigate whether 2 weeks of treatment with inhaled and intranasally administered fluticasone propionate alters the inflammatory response and the effect on bronchial responsiveness induced by exposure in a swine barn. The airway pulmonary tissue concentration of the steroid during inhalation treatment would be expected to be in the same order of magnitude 11 as that previously found to abolish cytokine release from epithelial cells in vitro 9.
Materials and methods
Subjects
A total of 16 healthy nonsmoking subjects (12 males) with a mean age of 27 yrs (range 21–46) participated in the study. In order to be considered eligible for participation, all subjects were required to show normal results on physical examination, chest radiography and spirometry. They had to have nohistory of asthma or allergic diseases, as evaluated by aquestionnaire. The study was approved by the ethics committee of the Karolinska Institute (Stockholm, Sweden) and was performed with the informed consent of all subjects.
Study design
The subjects were randomised to either receive fluticasone propionate (500 µg b.i.d. by inhalation and 100 µg intranasally once daily, 50 µg in each nostril; n=7, one female) or placebo (twice daily by inhalation; n=8, two females) for 10–14 days in a single-blind manner. The exposure took place after the last dose (∼1 h) while weighing pigs for 3 h in a swine barn, containing 700–900 pigs. The participants assisted the farmer and guided the pigs through weighing boxes. Analysis of nasal lavage (NAL) fluids, serum samples and bronchial methacholine responsiveness was performed at different time points before and after exposure, as follows.
Symptoms
After exposure, symptoms of shivering, headache, malaise, muscle pain and nausea were evaluated by the use of a questionnaire. The symptoms were graded according to severity on a scale of 1–5 (1: no symptoms; 5: severe symptoms). Only grades 4 and 5 were classified as significant. Oral temperature was measured directly before exposure, immediately after exposure and over the next 10 h at 2-h intervals.
Nasal lavage
NAL was performed before the start of medication, after 2 weeks of treatment (1 h before exposure) and 7 h after the start of exposure. The NAL procedure described by Pipkorn et al. 12 and Bascom et al. 13 was used with minor modifications. The subject flexed their neck 45° backwards and closed the soft palate while 5 mL 0.9% sodium chloride was instilled into one nostril using a needleless syringe. After 10 s, the neck was flexed forwards and the liquid expelled into a plastic basin, which was placed on ice during processing. The procedure was repeated on the other side. The volume of the combined lavage portions was measured and centrifuged for 10 min at 200×g at 4°C and the supernatant frozen at −70°C until analysis. The pellet was resuspended in 0.5 mL 9 mg·mL−1 NaCl containing 0.1% human serum albumin and the total number of recovered cells were counted in a Bürker chamber. Cytocentrifuge-prepared slides were stained with May-Grünwald Giemsa stain and 300 cells were assessed for differential cell counts. Less than 100 cells were considered too few cells for an accurate differential count.
Serum
Blood samples were collected before medication, 1 h before exposure and 4, 7 and 24 h after the start of exposure. Blood samples were allowed to coagulate at room temperature for 1 h before centrifugation (1,550×g for 10 min) and the serum was dispensed into several aliquots, which were kept at −70°C until analysis. Each sample underwent only one freeze/thaw cycle before assay.
Analysis
TNF-α and granulocyte-macrophage colony-stimulating factor (GM-CSF) levels in serum and NAL fluid were analysed using commercial high sensitive sandwich enzyme immunoassay kits (QuantikineTM; R&D Systems Europe, Abingdon, UK). The detection ranges were 0.5–32 pg·mL−1 for TNF-α and 1–64 pg·mL−1 for GM-CSF. IL-6 and IL-8 and RANTES (regulated upon activation, normal T-cell expressed and secreted) were measured using an ELISA developed in the authors' laboratory, together with an enzyme-amplified detection system when necessary. The IL-6 analyses were described in detail by Ek et al. 14 andthe lowest standard concentration was 0.125 pg·mL−1. For analyses of IL-8 and RANTES, commercially available antibody pairs, standards and QuantikineTM serum controls at three different concentrations (R&D Systems Europe) were used, and the lower detection limits were 25 and 2.34 pg·mL−1, respectively. Albumin in NAL fluid was quantified by ELISA, as previously described 4. The lower detection limit of the assay was 0.11 µg·mL−1. α2-Macroglobulin in NAL fluid was quantified using an ELISA as previously described 6. The lower detection limit of the assay was 0.5 pg·mL−1. Analysis of leukotriene (LT) E4 in NAL fluid was performed with an enzyme immunoassay using polyclonal antisera and an acetylcholinesterase-linked tracer, as previously described 15. The detection limit was 7.8 pg·mL−1. For all analyses, duplicates were measured and an intra-assay coefficient of variation of <10% andinter-assay coefficient of variation of <20% were accepted. Absorbance was measured using a Thermomax 250 reader (Molecular Devices, Sunnyvale, CA, USA).
Lung function tests and methacholine provocation
Lung function (forced expiratory volume in one second (FEV1) and vital capacity) was measured using a wedge spirometer (Vitalograph®; Medical Instrumentation, Buckingham, UK) according to the criteria of the American Thoracic Society 16. Local reference values were used 17, 18. Peak expiratory flow was measured with a mini-Wright peak flow meter (Clement Clarke, London, UK); the best of three blows was registered.
Bronchial responsiveness was assessed by methacholine challenge. Inhalation of diluent was followed by inhalation of doubling methacholine concentrations, starting at 0.5 mg·mL−1 and up to 64 mg·mL−1 or until there was a 20% fall in FEV1, as previously described 19. The results were expressed as the provocative concentration (PC20) or cumulative dose (PD20) of methacholine causing a 20% fall in FEV1. In one subject pre-exposure FEV1 did not fall by 20% at the maximum concentration. This subject was assigned a PC20 of 65 mg·mL−1 for nonparametric statistical calculations.
The methacholine provocation and lung function tests were performed ∼1–2 weeks before medication and 4 h after cessation of exposure in the swine house.
Exposure measurements
Total dust and endotoxin levels were measured in inhalable and respirable dust as previously described 14.
Statistics
Oral temperatures and lung function data are presented as mean±sem/sd, as indicated, and comparisons were made using ANOVA and/or a t-test. Data on bronchial responsiveness, cell count, soluble products in NAL fluid and serum (except for IL-6) are given as median (interquartile range), and comparisons were made using the Wilcoxon signed-rank-sum test and Mann-Whitney U test. Serum levels of IL-6 were compared by ANOVA and t-tests after confirmation ofnormal distribution of pre-exposure data ( Z-score). A p-value of <0.05 was considered significant. Spearman rank coefficients (rho) were calculated for correlations. Concentrations below the detection limits were assigned a fixed value slightly lower than the lower detection limit for statistical comparisons.
Results
One subject in the fluticasone group was excluded from all analyses due to an upper airway infection that commenced during the pre-exposure treatment period. In addition to severe symptoms of airway infection, all inflammatory marker levels measured were highly elevated 1 h prior to exposure compared to the pre-treatment values obtained 2 weeks previously in this subject.
Symptoms
Five of the eight participants in the placebo group and two of the seven in the fluticasone group experienced symptoms (grades 4 and 5) following exposure. Two participants in the placebo group experienced shivering, one headache and two malaise, and the two individuals in the fluticasone group experienced malaise.
Oral temperature was 35.9±0.5 and 35.9±0.3°C (mean±sd) immediately before exposure in the placebo and fluticasone groups respectively (fig. 1⇓). The temperature increased after exposure in both groups to a maximum 9–11 h after exposure (p<0.01). The increase in temperature was significantly lower in the fluticasone group than in the placebo group (F=3.5, p=0.007).

Oral temperature in healthy subjects before and after exposure (▪) in a swine house. The subjects were treated with placebo (○; n=8) or fluticasone propionate (•; n=7) for 2 weeks prior to exposure. Data are presented as mean±sem. The increase in body temperature was significantly smaller in the fluticasone group than in the placebo group (F=3.5, p=0.007). *: p<0.05; **: p<0.01 versus pre-exposure values.
Nasal lavage fluid
In the placebo group, exposure caused a significant increasein total cell (p=0.01) and neutrophilic granulocyte concentration (p=0.02), whereas no significant changes in total cell (p=0.5) or neutrophil concentration (p=0.18) were found in the fluticasone group (fig. 2⇓, table 1⇓). There was, however, no significant difference between the groups with regard to total cell (p=0.3) or neutrophil concentration (p=0.4).

Analysis of nasal lavage fluid from healthy subjects before and after exposure in a swine house: a) cell concentration, and b–g) concentrations of b) interleukin (IL)-6, c) IL-8, d) tumour necrosis factor (TNF)-α, e) albumin, f) α2-macroglobulin, and g) leukotriene (LT)E4. The subjects were treated with placebo (○; n=8; n=6 for LTE4 analysis) or fluticasone propionate (•; n=7; n=5 for LTE4 analysis) for 2 weeks before exposure. Owing to the limited volume of lavage fluid, only 11 LTE4 analyses could be performed. Data are presented as median (interquartile range). Fluticasone propionate treatment did not significantly alter concentrations of cells IL-6, IL-8, albumin or α2-macroglobulin before exposure. PM: premedication; BE: before exposure; AE: after exposure. *: p<0.05 versus pre-exposure values; #: p=0.6; ¶: p=0.3; +: p=0.07; §: p=0.06; ƒ: p=0.03; ##: p=0.02 difference between groups before and after exposure.
Nasal lavage fluid cell densities before and after exposure in a swine house#, in subjects treated with placebo or fluticasone propionate¶
There was a significant increase in IL-6 and IL-8 and TNF-α levels after exposure, whereas LTE4, albumin and α2-macroglobulin levels increased significantly only in the placebo group (fig. 2⇑). There were significantly lower increases in the fluticasone group with regard to IL-8 (p=0.02), TNF-α (p=0.03) and albumin (p=0.02). GM-CSF concentrations in NAL fluid (1 h before and 7 h after exposure) were below the detection limit (<1 pg·mL−1) in both groups. The RANTES concentration in NAL fluid was below the detection limit (<2.3 pg·mL−1) in 14 of the 16 subjects before medication, in 13 of the 16 subjects before exposure and in 10 of the 16 subjects after exposure.
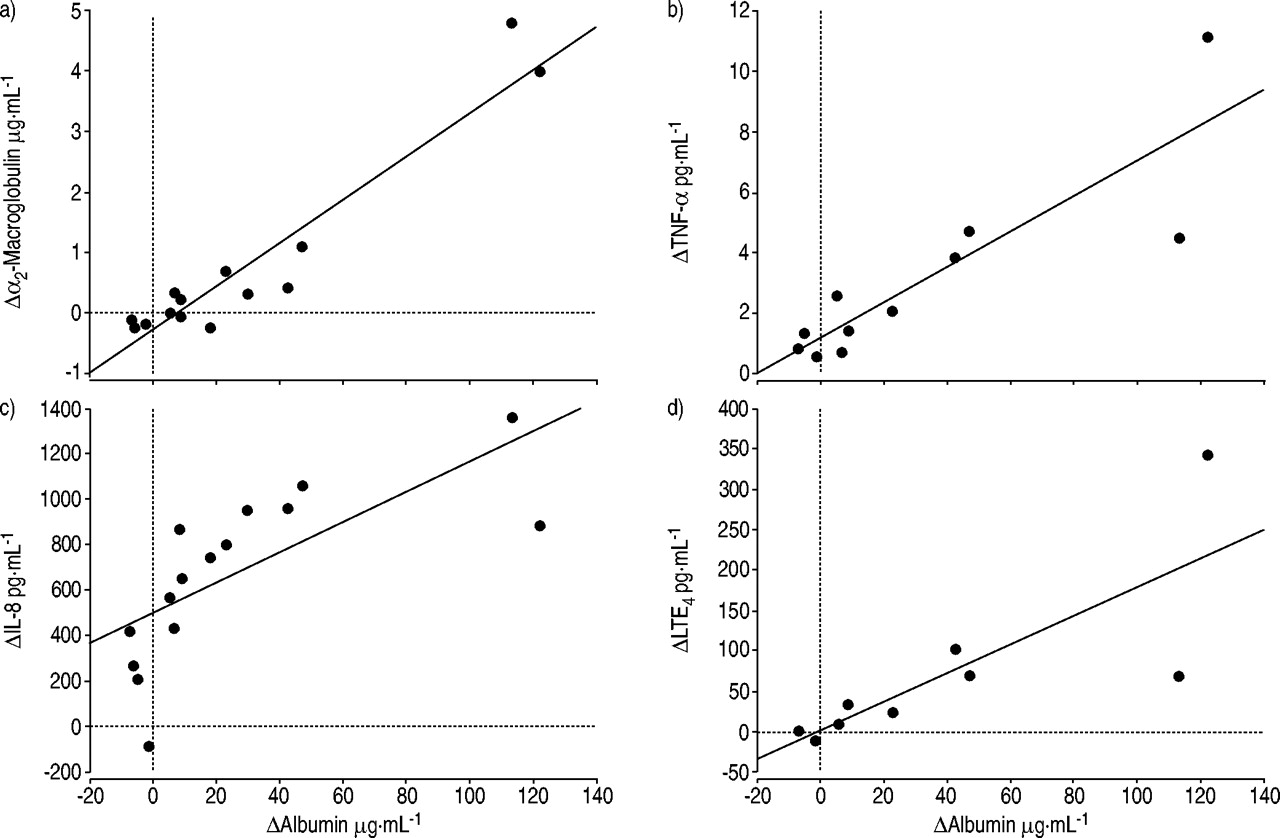
There were significant correlations between post-exposure increases in levels of albumin and of α2-macroglobulin (rho=0.79, p=0.003), IL-8 (rho=0.90, p=0.0007), TNF-α (rho=0.84, p=0.004) and LTE4 (rho=0.92, p=0.004) (fig. 3⇓).

Correlations between differences (Δ: after exposure–before exposure) in nasal lavage fluid (whole material) levels of albumin and: a) α2-macroglobulin (rho=0.79, p=0.003), b) tumour necrosis factor (TNF)-α (rho=0.84, p=0.004), c) interleukin (IL)-8 (rho=0.90, p=0.0007), and d) leukotriene (LT)E4 (rho=0.92, p=0.004) (n=15 (n=11 for LTE4 analysis)).
Serum
The concentration of IL-6 in serum increased significantly in both groups (p<0.05), with a lesser increase in the fluticasone group (F=3.2, p=0.03) (fig. 4⇓). In the placebo group (but not in the fluticasone group), there was a correlation between the maximum increase in serum IL-6 concentration and the maximum increase in body temperature (rho=0.79, p=0.04). The serum concentration of TNF-α 1 h before exposure was 2.0 (1.9–2.2) pg·mL−1 in the placebo group and 2.6 (1.5–2.8) pg·mL−1 in the fluticasone group, and did not change after exposure. The RANTES concentrations 1 h before exposure were 71 (51–83) ng·mL−1 in the placebo group and 71 (67–79) ng·mL−1 in the fluticasone group, and did not change after exposure. Exposure or medication did not significantly affect the serum concentrations of TNF-α or RANTES. GM-CSF concentrations in serum were below the detection limit (<1 pg·mL−1) in all but one subject.

Interleukin (IL)-6 concentrations in serum from healthy subjects before and after exposure (▪) in a swine house. The subjects were treated with placebo (○; n=8) or fluticasone propionate (•; n=7) for 2 weeks prior to 3 h of exposure. Data are presented as median (interquartile range). There is a significant difference between the groups (F=3.2, p=0.03). PM: premedication. *: p<0.05; **: p<0.01 versus pre-exposure values (1 h before exposure).
Lung function
Exposure caused a slight but significant decrease in vital capacity and FEV1 in all subjects, and there was no significant difference between the groups (table 2⇓).
Lung function before and after exposure in a swine house# in subjects treated with placebo or fluticasone propionate¶
Methacholine provocation
Bronchial responsiveness to methacholine increased significantly in both groups after swine house exposure, with no significant difference between the groups (p=0.4) (fig. 5⇓). In the placebo group, the PD20 fell from 1.90 (1.24–5.23) mg before to 0.25 (0.08–0.35) mg after exposure (p=0.01) and, in the fluticasone group, from 1.39 (0.52–2.34) mg before to 0.12 (0.08–0.15) mg after exposure (p=0.02). Thus bronchial responsiveness to methacholine increased by 3.2 (2.8–4.1) doubling concentration steps in the placebo group and 2.5 (1.5–3.9) doubling concentration steps in the fluticasone group.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bronchial responsiveness to methacholine before medication and 7 h after the start of the exposure in a swine house in healthy subjects pretreated with placebo (n=8) or fluticasone propionate (n=7) during the 2 weeks prior to exposure (….: highest inhaled concentration of methacholine). The change in bronchial responsiveness calculated from the decrease in doubling concentration steps did not significantly differ between the groups (p=0.4). PC20: provocative concentration of methacholine causing a 20% fall in forced expiratory volume in one second. *: p<0.05 versus pre-exposure values.
Exposure measurements
The concentration of inhalable dust, assessed by the use ofpersonal samplers, was 27.2 (19.8–36.4) mg·m−3, 842 (396–1,197) ng·m−3 of which was the endotoxin concentration. The concentration of respirable dust was 0.98 (0.72–1.27) mg·m−3, 33 (15–51) ng·m−3 of which was the endotoxin concentration 14. There were no significant differences in exposure between the groups.
Discussion
In the present study, it has been demonstrated that 2 weeks of fluticasone propionate treatment significantly attenuated the systemic effects induced by exposure to organic dust in a swine barn. Thus, the increase in body temperature and serum IL-6 levels after exposure were significantly lower in the fluticasone group than in the placebo group. Furthermore, intranasally administered fluticasone propionate had a major influence on the exposure-induced plasma leakage into the upper airways and significantly attenuated the nasal IL-8 and TNF-α response. However, fluticasone propionate inhalation did not alter the increased bronchial responsiveness to methacholine induced by exposure.
Exposure in swine houses causes airway inflammation with an increase in levels of inflammatory mediators, such as IL-6, in lavage fluid and blood 4. Therefore, there is reason to believe that the airway is the source of the elevated IL-6 levels found in blood. IL-6 is an endogenous circulating pyrogen, responsible for induction of fever during infection and inflammation 20; increased levels of IL-6 are found in the blood of patients following injury and correlate significantly with the increase in body temperature 21. In the present study, a correlation was found between the maximal increase in serum IL-6 level and body temperature after exposure in the placebo group but not in the fluticasone group. Therefore, a causal relationship might exist between the post-exposure attenuation of serum IL-6 level and body temperature in the fluticasone group. Fluticasone propionate, however, did not alter IL-6 release neither in the nose (NAL) nor, as previously demonstrated 14, in the lungs following exposure. One reason for this could be that the major source of serum IL-6 might be the lower airways and BAL was performed too late (24 h after exposure) to detect a possible steroid-mediated effect on airway IL-6 release in that study. Recent unpublished findings in the present study laboratory support such a hypothesis, demonstrating that IL-6 release and expression decline in epithelial cells after a few hours of exposure to swine house dust in vitro. It has previously been shown that fluticasone propionate inhibits IL-6 secretion from alveolar macrophages stimulated by lipopolysaccharide and abolish IL-6 secretion from swine dust-stimulated epithelial cells at a concentration (1×10−9 M) that can be anticipated to occur in lung tissue during treatment with the doses used in the present study 9, 11. In addition, it has recently been shown that the transcription factor NF-κB is involved in organic-dust-mediated cytokine release (IL-6 and IL-8) from epithelial cells, and that inhibition of IL-6 and IL-8 release by glucocorticoids is, in part, mediated by inhibition of this mechanism 10. These in vitro data are in agreement with the finding of lower IL-6 levels following exposure in the subjects who were treated with glucocorticoids. The effect on serum IL-6 might explain the attenuated increase in post-exposure body temperature in the steroid-treated group.
Topical fluticasone propionate treatment inhibited the organic-dust-induced increase in IL-8 and TNF-α levels in NAL fluid following organic dust exposure, which is consistent with previous findings in vitro 9, 10. Neutrophilic granulocytes, which increase substantially in number after exposure 2, may, in addition to epithelial cells, be an important source of IL-8 and TNF-α, since both cell types are capable of producing both cytokines 22. In a recent study, glucocorticoids were found to be important inhibitors of IL-8 release from neutrophils in vitro 23. Mast cells are also important sources of TNF-α and IL-8 production 24. Mast cells seem to play a role in the organic-dust-mediated airway inflammatory response since urinary excretion of 9α,11β-prostaglandin F2, a prostaglandin D2 metabolite that is almost exclusively produced by mast cells, increases after exposure 25. In addition, inhalation of sodium cromoglycate alters the inflammatory reaction to swine dust exposure, probably by interacting with mast cells 26. It was recently shown that dexamethasone potently inhibits TNF-α production by activated mast cells in vitro 27. It is thus possible that fluticasone propionate treatment attenuates the organic-dust-induced cytokine level increase by interaction with epithelial cells and other cell types, such as mast cells and/or neutrophils.
Topical fluticasone propionate treatment also inhibited the leakage of plasma proteins (albumin and α2-macroglobulin) into NAL fluid following organic dust exposure. This finding indicates a major effect on plasma leakage induced by exposure and confirms previous data showing that glucocorticoids inhibit plasma exudation in inflammatory airways diseases 28. It is not known whether the anti-exudative efficacy of glucocorticoids in rhinitis and asthma 29, 30 reflects a direct effect of glucocorticoids on the microvascular wall in human airways or whether it reflects indirect action on cellular inflammatory responses. The possibility of direct action on the microvascular wall has been demonstrated in animal experiments 31. However, budesonide treatment did not affect the histamine-induced mucosal exudation of albumin in humans and it has, therefore, been claimed that the anti-exudative efficacy of topical glucocorticoids in airway disease reflects the ability of these drugs to suppress cellular mechanisms 32. A relationship was found between the release of IL-8 or LTE4 and albumin and α2-macroglobulin into NAL fluid. The increased vascular permeability observed under inflammatory conditions is suggested to be driven by cysteinyl LTs 33 and possibly IL-8, which may also induce plasma exudation 34. It is thus possible that the IL-8 and LTE4 released after exposure contribute to the plasma exudation observed, and the significant inhibition of exposure-induced IL-8 release by fluticasone propionate might, in part, lead to the inhibition of plasma leakage.
No effect of fluticasone propionate treatment on the increase in methacholine-induced airway responsiveness induced by exposure in a swine barn was found in healthy subjects. A recent meta-analysis on the dose/response relationship between inhaled corticosteroids and bronchial hyperresponsiveness in asthmatic subjects showed that glucocorticoids reduce airway hyperresponsiveness to methacholine by 0.45–3.47 doubling dose steps and that high doses confer greater improvement than low doses 35. However, the factors predictive of improvement in bronchial hyperresponsiveness with inhaled glucocorticoids are still largely unknown, and the relationship between inflammation and bronchial hyperresponsiveness is not clear. In agreement with the present findings, Nightingale et al. 36 found that inhaled budesonide did not protect against neither theozone-induced increase in methacholine reactivity nor the increase in sputum neutrophil numbers in normal subjects.
In conclusion, it was found that glucocorticoid treatment attenuated the upper airway response and the systemic response to inhaled organic dust without affecting the increased bronchial responsiveness.
Acknowledgments
Fluticasone propionate and placebo were generously provided by Glaxo Smith Kline (Greenford, UK). The authors would like to thank K-G. Kölbeck for work with subjects, S. Siljerud, C. Müller-Suur, B-M. Larsson, B-M. Sundblad, H. Saranius and I. Dehlin for skilful technical assistance and M. Kumlin for valuable advice.
- Received February 13, 2004.
- Accepted May 12, 2004.
- © ERS Journals Ltd
References









