





Abstract
The efficacy of antimicrobial agents against pulmonary infections depends on their local concentrations in the lung. The aims of the present study were to: 1) compare technetium‐99m diethylenetriaminepenta-acetic acid (99mTc‐DTPA) and urea as markers of epithelial lining fluid (ELF) dilution for measuring ELF concentrations of pharmaceuticals; 2) quantify ELF cefepime concentrations in normal and injured lung; and 3) measure the increase in permeability to cefepime following oleic acid-induced acute lung injury.
A modified bronchoalveolar lavage technique, based on equilibration of infused 99mTc-DTPA, was used to measure ELF volume. Cefepime was administered intravenously at steady plasma levels. Six serial bronchoalveolar lavages were performed 5 h after the beginning of infusion.
ELF to plasma cefepime concentration ratios were 95±17 and 100±14.5% in normal and injured lung respectively. When urea was used as marker, cefepime concentration ratios were underestimated at 16.4±2.7 and 73.9±8.4% respectively. Cefepime blood/airspace clearance increased from 3.8±0.7 µL·min−1 in controls to 39.8±4.9 µL·min−1 in acute lung injury.
It was concluded that: 1) cefepime concentrations in epithelial lining fluid were in equilibrium with those in plasma in both normal and injured lung after 5 h at steady plasma concentrations; 2) epithelial lining fluid cefepime concentration by the urea method was much less underestimated in injured versus normal lung; and 3) acute lung injury induces a 10‐fold elevation of cefepime blood/airspace clearance.
- Acute respiratory distress syndrome
- antibiotics
- blood/air barrier
- bronchoalveolar lavage fluid
- pulmonary alveoli
This study was funded by grants from the Bristol-Myers-Squibb Company (New York, NY, USA) and the French Cystic Fibrosis Association (Paris, France) (AFLM, RC99008).
Bronchoalveolar lavage (BAL) has been used extensively to study the chemical and cellular composition of epithelial lining fluid (ELF) and for aetiological diagnosis of lung infection. A major limitation of BAL is the unpredictable dilution of ELF by the instilled saline 1. Urea has often been used as an endogenous marker of ELF dilution. However, since urea rapidly diffuses into the BAL fluid (BALF) during the lavage procedure, this indicator leads to overestimation of ELF volume (VELF) 2, 3. A method based on the equilibration of technetium‐99m diethylenetriaminepenta-acetic acid (99mTc‐DTPA) between blood and ELF, which accounts for the diffusion of the indicator, as well as fluid exchange during lavage, was recently developed 4. The efficacy of antimicrobial therapy directly depends on drug concentrations at the site of infection. In bacterial pneumonia, microorganisms multiply in the alveolar acini and in the alveolar ELF 5. β‐Lactams reach this compartment by passive concentration-dependant diffusion from blood, across the alveolocapillary barrier 5. The presence of active inflammation increases the permeability of the alveolocapillary barrier and facilitates thepenetration of drugs from blood to ELF. However, the significance of this phenomenon has rarely been assessed quantitatively. Cefepime, a “fourth-generation” cephalosporin, has an extended spectrum of activity that encompasses both Gram-positive organisms, such as Staphylococcus aureus and Streptococcus pneumoniae, and Gram-negative pathogens, including Pseudomonas aeruginosa, Enterobacter spp. and other members of the Enterobacteriaceae family 6. Cefepime is, therefore, one of the preferred agents for empirical monotherapy of nosocomial pneumonia 7.
The first aim of the present study was to measure the concentration of cefepime in ELF (CELF,cefepime) following continuous intravenous administration, at steady state. The second goal of the study was to assess alveolocapillary permeability to cefepime in normal lung, as well as in acute lung inflammation. An oleic acid injection model, which is known to induce acute lung inflammation, increased alveolocapillary permeability and oedema, was used 8. The third goal of the study, since urea is widely used as an endogenous marker of ELF dilution, was to compare the VELF and CELF,cefepime/plasma cefepime concentration ratios based on 99mTc-DTPA versus urea. The error due to urea diffusion into BALF during lavage was evaluated with reference to 99mTc-DTPA. Finally, a correction method accounting for urea diffusion into BALF during lavage was also tested. The present study provided a good opportunity to compare these three methods for the estimation of the ELF concentration ofa low-molecular-weight solute, cefepime, in control and acutely injured lung.
Materials and methods
Animal preparation
Animal care and procedures were performed in accordance with the guidelines for the Care and Use of Animals provided by the American Physiological Society, and approved by the local institutional authorities. The experiments were performed on nine anaesthetised beagles weighing 13.6±0.2 kg (mean±sem). A 20‐G catheter (Venflon®, Viggo, Helsingborg, Sweden) was placed in a forelimb vein. The dogs were anaesthetised with 100–150 mg intravenous propofol (Diprivan; Zenecca Laboratories, Cergy Pontoise, France), intubated and mechanically ventilated. Anaesthesia was maintained with continuous intravenous propofol infusion at 30–40 mg·kg body weight−1·h−1. The inspiratory oxygen fraction was adjusted to maintain arterial blood gas levels within the normal range in injury experiments. A second 20‐G catheter was placed in a contralateral forelimb vein for blood sampling. A 7.5‐F Swan-Ganz catheter (Baxter, Maurepas, France) was placed in a pulmonary artery via a femoral vein by the Seldinger technique, for pulmonary artery wedge pressure and cardiac output monitoring in injury experiments, and for intracardiac injection of oleic acid. In addition, a polyethylene carotid artery catheter was placed in these experiments for blood pressure monitoring.
Saturation bronchoalveolar lavage procedure
The saturation BAL technique has been reported in detail previously 9. Briefly, prior to each experiment, a batch BAL solution of 500 mL was prepared by adding 50 mg fluorescein isothiocyanate-labelled dextran (2,000 kDa) (FITC-D2000; Sigma, Saint-Quentin-Fallavier, France) to 500 mL sterile physiological saline to give a final concentration of 100 mg·L−1. An inflatable latex balloon was adapted to the extremity of a paediatric fibreoptic bronchoscope (Fujinon, Tokyo, Japan; distal tip diameter 4.8 mm). Prior to each BAL, the bronchoscope was inserted into the endotracheal tube through an airtight adapter, and its distal end randomly placed in a segmental bronchus. A pressure transducer was connected to the bronchoscope lumen. The balloon was inflated and the seal provided by the balloon tested by serial injections of 10‐mL boluses of air into the bronchoscope lumen. In order to estimate the volume of BALF to be instilled, pressure increments induced by successive 10‐mL air injections were recorded over a few seconds. When the initial pressure in the lung segment was >10 cmH2O for a total injected air volume of 60 mL, the bronchoscope was repositioned in another segment, or the instilled BALF volume was reduced to equal the air volume producing a pressure increment of ≤10 cmH2O. The lavage fluid was contained in a closed-circuit at all times and lavage fluid pressure was monitored continuously to prevent overinflation or excessive suction of the lavaged lung segment; 20–50 mL lavage fluid were initially instilled in ∼15 s, and 2–3 mL air was injected to clear the operating channel dead space, followed by rapid aspiration. Fluid retrieval was visually monitored through the bronchoscope, and suction was stopped as soon as the bronchus tended to narrow. A 3‐mL sample was taken from the retrieved lavage fluid. Fresh lavage fluid was added to the retrieved fluid so that the total volume was equal to the volume of fluid initially instilled. This fluid was then reinstilled, and the lavage cycle repeated six times. The volume of instilled fluid was, therefore, identical from one lavage cycle to the next.
Experimental protocol
After 30 min of recording at baseline, a 1.3 mL bolus of 0.5 mCi·mL−1 99mTc-DTPA in saline (Pentacis; Cis Bio International, Paris, France) was injected intravenously, followed immediately by infusion at 2 mL·h −1 for the entire duration of the experiment. At the same time, a 10 mg·kg body weight−1 bolus of cefepime was administered intravenously, followed by continuous infusion at 7.7 mg·kg body weight−1·h−1 for the duration of the experiment. The total administered dose of cefepime in the whole experiment was 48.5 mg·kg body weight−1. This infusion protocol was used in order to obtain steady-state plasma concentrations as early as possible. Preliminary experiments were performed to determine adequate bolus dose and infusion rate for cefepime, in order to obtain steady-state plasma concentrations. A 10 mg·kg body weight−1 intravenous bolus of cefepime was administered in one dog. Cefepime concentrations were described by a two-compartment pharmacokinetic model with an estimated elimination half-life of 54 min. This value was close to those previously reported in dogs 10. In a second animal, the bolus dose and perfusion rates were tested in order to verify that steady-state plasma concentrations were obtained. In control experiments, 5 h after the start of 99mTc-DTPA and cefepime infusion, six serial BALs were performed. After 7–15 days, the same animals underwent a second experiment. In these experiments, serial BALs were also performed 5 h after the beginning of 99mTc-DTPA and cefepime infusion. Acute lung injury was induced 3 h prior to lavage by gradual injection of 0.05 mg·kg body weight−1 oleic acid (Sigma) diluted in 5 mL ethanol, through the proximal port of the Swan-Ganz catheter, over 1 min. The reason injury was induced at this point in time was based on previous observation that a 3‐h interval after oleic acid injection is helpful in obtaining a stable and significant increase in extravascular lung water and microvascular permeability 4.
Sample processing
99mTc-DTPA activity was measured in 0.5‐mL samples of retrieved lavage fluid immediately after the end of the experiment using a Packard Cobra II gamma counter (Global Medical Instrumentation, Clearwater, MN, USA). Corrections were made for background noise and the decay of 99mTc-DTPA. FITC-D2000 concentrations were measured in plasma and BALF using a fluorescence spectrophotometer (Perkin-Elmer® LS50; Perkin Elmer, Norwalk, CT, USA). The excitation and emission wavelengths were 485 and 520 nm respectively. Cefepime concentrations in plasma and BALF were measured by ion-pair liquid chromatography with ultraviolet absorption detection at 280 nm after solid-phase extraction. The lower quantification limit was 0.1 mg·L−1, and the between-day coefficient of variation was <10% over the calibration range. The urea concentration in plasma and BALF was determined by a urease assay (Roche Diagnostics, Meylan, France) using a Hitachi 917 automatic analyser (Hitachi, Tokyo, Japan). For BALF, additional sample volume was added to the reaction mixture in order to enhance sensitivity. Calculation methods are detailed in the Appendix.
Statistics
Group data are presented as mean±sem. A paired t‐test was used to compare data between groups. The single-factor analysis of variance (ANOVA) test was used to assess the significance of changes in lavage data as a function of time. Differences with a p‐value of <0.05 were considered significant.
Results
Fluid retrieval
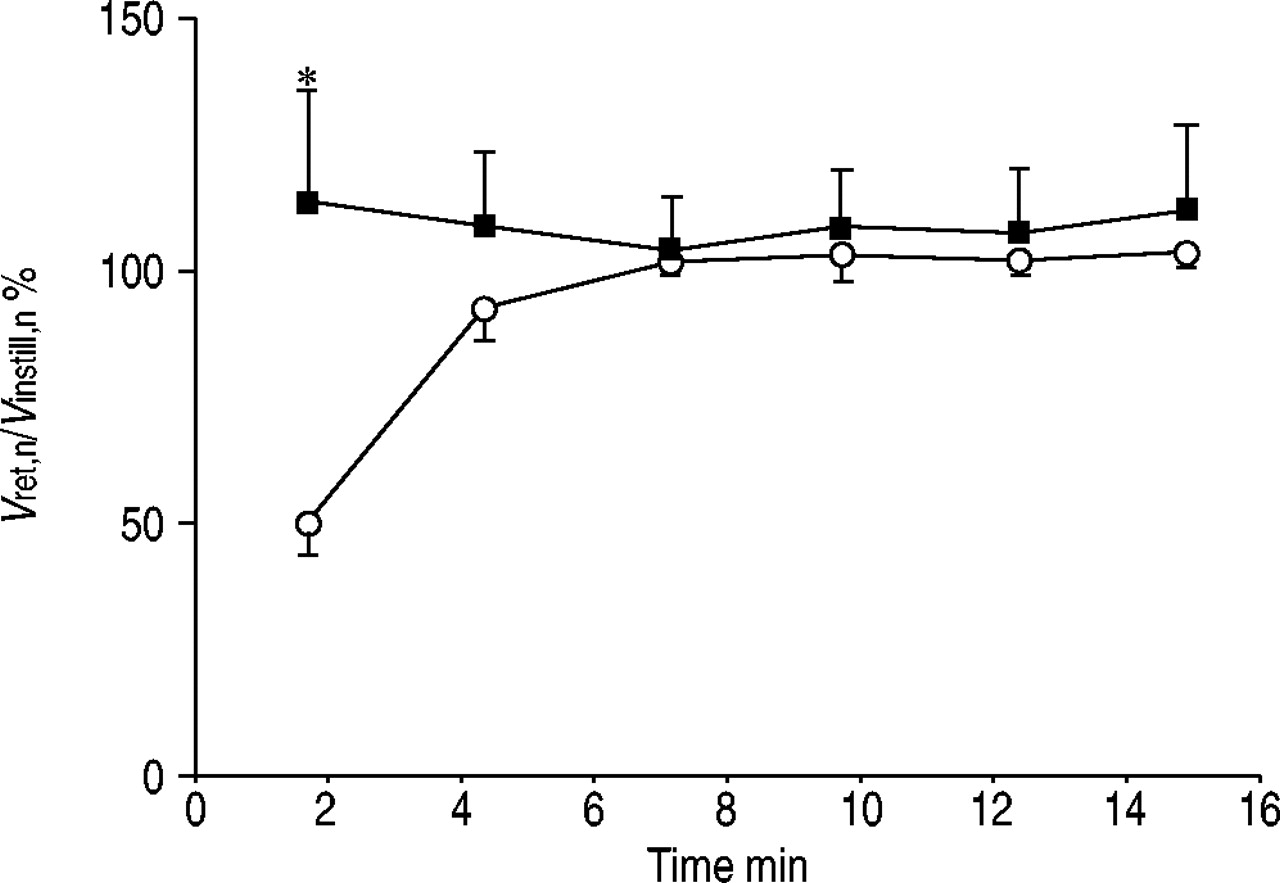
The instilled volumes were 36.1±3.1 and 26.1±2.3 mL in control and injury experiments respectively. The smaller instilled volume in injury experiments was due to the lower compliance of injured lung during the inflation manoeuvres preceding lavage, since the instilled volume was defined as that equal to the same volume of air producing a pressure increment of ≤10 cmH2O. Fluid recovery was total beyond the third lavage in normal lung (fig. 1⇓). In injured lung, more fluid was recovered than instilled in early lavages, due to the abundant presence of oedema fluid.
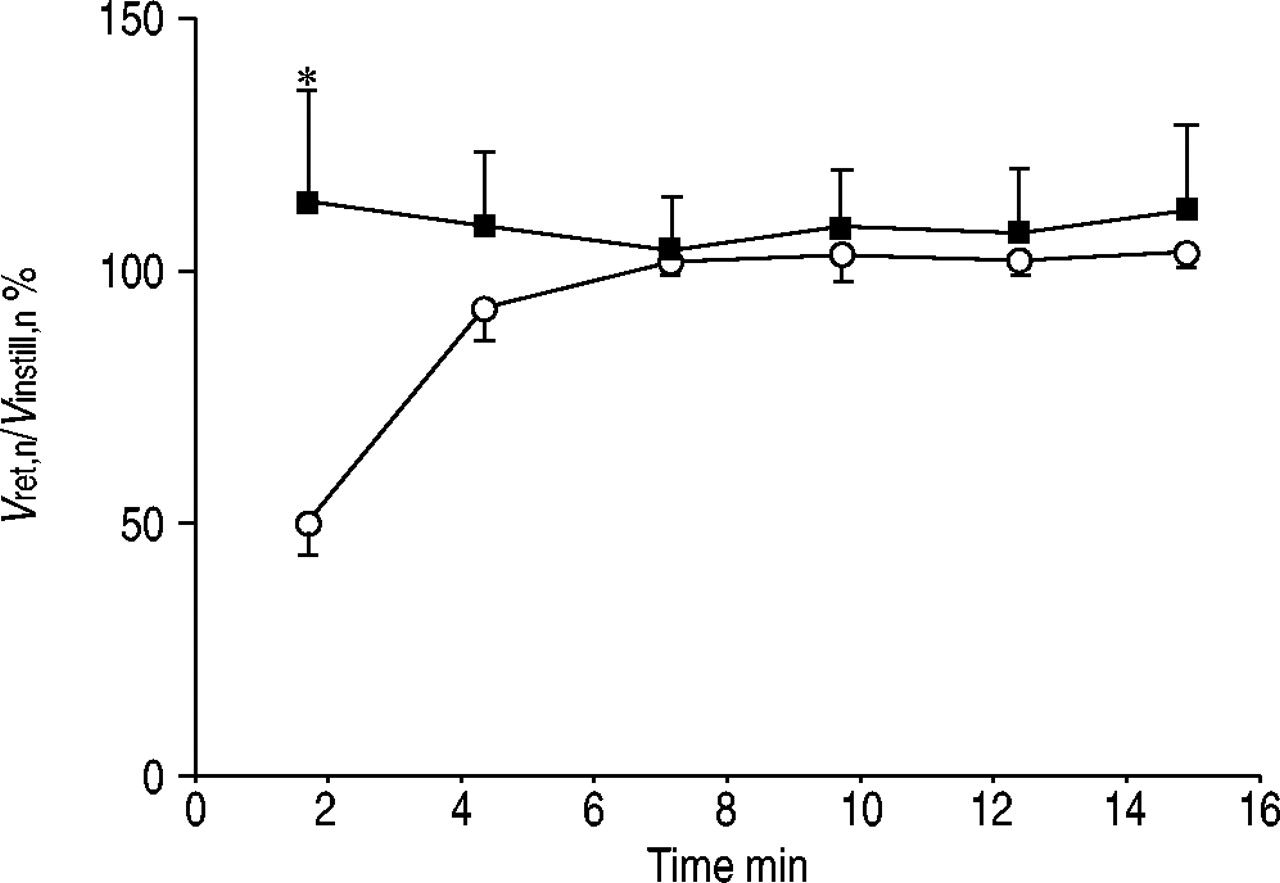
Ratio of retrieved (Vret,n) to instilled (Vinstill,n) broncholaveolar lavage fluid volume in lavage cycle n in control (○) and injured (▪) lung. Data are presented as mean±sem. *: p<0.05 versus control.
99mTc‐DTPA activity and urea concentration in the retrieved bronchoalveolar lavage fluid
In normal lung, 99mTc-DTPA activity in the retrieved BALF increased progressively with time, from 11.6×103±2.3×103 counts per minute (cpm)·mL−1 in the first lavage cycle to 16.7×103±3.2×103 cpm·mL−1 in the sixth lavage cycle (fig. 2a⇓). The change in 99mTc-DTPA activity was not significant by single-factor ANOVA. A larger relative increase was observed in the urea concentration in the retrieved BAL fluid from 0.3±0.2 mM in the first lavage cycle to 0.9±0.2 mM in the sixth lavage cycle (p<0.001, single-factor ANOVA) (fig. 2b⇓).

a) Technetium-99m diethylenetriaminepenta-acetic acid activity (Cret,n,99mTc-DTPA) and b) urea concentration (Cret,n,urea) in retrieved bronchoalveolar lavage fluid as a function of time from the beginning of n serial lavages in control (○) and injured (▪) lung. Data are presented as mean±sem.
In injured lung, 99mTc-DTPA activity in the retrieved BAL fluid was 159×103±21×103 cpm·mL−1 in the first lavage cycle, and 154×103±30×103 cpm·mL−1 in the sixth lavage cycle (fig. 2a⇑), which did not significantly change by ANOVA. Similarly, urea concentration was 1.6±0.4 mM in the first lavage cycle and 2.0±0.6 mM in the sixth lavage cycle, the difference being nonsignificant (fig. 2b⇑).
Epithelial lining fluid volume
Since VELF depends on the size of the lavaged compartment, it was also expressed as a percentage of Vtot,n. In injured lung, VELF represents the volume of oedema fluid in the lung segment prior to lavage, which is very large compared to control VELF.
Using the 99mTc-DTPA method (method A), a single VELF can be calculated from each experiment. This is also the case using method C, i.e. using urea as indicator with a correction for urea diffusion. The situation is quite different using method B, the urea method as proposed by Rennard et al. 11 and its single-cycle variant, which is the method used in clinical studies. In the latter case, absolute VELF cannot be calculated; however, the concentration of a solute such as CELF,cefepime can be estimated for each volume of retrieved lavage fluid using the dilution factor Čp,urea/Cret,n,urea (see Appendix). When VELF was estimated using endogenous urea as an indicator along with a correction to account for urea diffusion during lavage (VELF,urea; method C), VELF,urea represented overestimation of VELF by >238% in normal lung (2.0±0.6 versus 0.84±0.14 mL). In injured lung, VELF,urea by method C was 183% of the VELF estimated by method A (table 1⇓).
Epithelial lining fluid volume (VELF) calculated using methods A# and C¶
Cefepime concentrations in plasma and retrieved bronchoalveolar lavage fluid
Cefepime concentrations in plasma and retrieved BALF are summarised in table 2⇓. Cefepime concentrations in plasma were stable over time. Generally, plasma cefepime concentrations were significantly higher in injury experiments versus controls, although the difference did not reach significance. The BAL fluid to plasma cefepime concentration ratio (mean value for all six lavages) was much higher (43.4±4.6%) in injured lung than in controls (2.5±0.5%) (p<0.05).
Cefepime concentrations in plasma (Čp,cefepime)¶, bronchoalveolar lavage fluid (CBAL,cefepime)+ and epithelial lining fluid (CELF,cefepime)
Cefepime concentrations in epithelial lining fluid
Using method A, the calculated CELF,cefepime were slightly higher in injured lung than in control; however, this was in proportion to the difference in plasma concentrations. Consequently, CELF,cefepime expressed as a percentage of plasma cefepime concentration were 95±17 and 100±14.5% in normal and injured lung respectively, and were not significantly different (table 2⇑). Using urea as an endogenous indicator, CELF,cefepime can be estimated for each of the six individual lavages in the sequence as shown in figure 3⇓. From the beginning of the sequential lavages, the concentration of urea in the retrieved BALF in lavage cycle n is increasingly overestimated in normal lung, and, consequently, the calculated CELF,cefepime are increasingly underestimated. When CELF,cefepime estimation was based on mean BAL concentrations of Cefepime and urea by method B, simulating the situation in which fluid from all six lavage cycles is pooled, CELF,cefepime was underestimated compared to method A in both normal and injured lung. However, this underestimation was much greater in normal lung (table 2⇑). Using the single-cycle urea variant (method B, single cycle), a higher estimate of CELF,cefepime was obtained in normal lung, but this made no difference in injured lung (table 2⇑). Using method C, which includes a correction for urea exchange during the lavage process, significantly higher CELF,cefepime were obtained in control lung, but no difference was observed in injured lung compared to method B (table 2⇑). Overall, CELF,cefepime calculated by method C were still lower than those calculated by method A, which uses 99mTc-DTPA as indicator. A graphic comparison of the estimated CELF,cefepime by the three methods is presented in figure 4⇓.

Estimated cefepime concentrations in epithelial lining fluid based on urea concentrations in plasma and bronchoalveolar lavage fluid (CELF,cefepime; method B (Appendix)) as a function of time from beginning of lavage in control (○) and injured (▪) lung. Data are presented as mean±sem. *: p<0.05 versus control.

Epithelial lining fluid cefepime concentrations (CELF,cefepime) relative to plasma concentration (Čp,cefepime), estimated by methods A (□), B (└), single-cycle B (┘) and C ( ) (see Appendix). Data are presented as mean±sem. No significant difference was found in injured versus control lung by method A. *: p<0.05 versus method A; #: p<0.05 versus method B, single cycle.
) (see Appendix). Data are presented as mean±sem. No significant difference was found in injured versus control lung by method A. *: p<0.05 versus method A; #: p<0.05 versus method B, single cycle.
Cefepime blood/airspace clearance
99mTc-DTPA blood/airspace clearance increased from 6.2±1.2 µL·min−1 in control, to 63.6±30.6 µL·min−1 in injured lung. Similarly, Cefepime clearance increased ∼10‐fold from 3.6±0.6 in normal lung to 59.5±24.3 µL·min−1 following oleic acid-induced acute lung injury (fig. 5⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cefepime blood/airspace clearance (CLcefepime) in normal and injured lung. *: p<0.05 versus control.
Discussion
ELF is the least permeable extracellular lung compartment. It is separated from the lung interstitium by the alveolar epithelium, which has very low permeability due to the presence of tight junctions, impeding solute and fluid exchange between the lung interstitium and the alveolar lumen 12. BAL is widely used to study ELF composition in both humans and animals; however, a major difficulty with this technique has been estimation of the dilution of the ELF by the instilled saline. Although it is well known that use of urea as an endogenous marker for estimation of ELF dilution results in overestimation of VELF, it is still widely used due to its simplicity. A method was developed recently, based on the equilibration of 99mTc-DTPA between blood and ELF, which accounts for the diffusion of the indicator during lavage 4. In the present study, both indicators were compared in order to evaluate the true error when urea is used as a dilution marker, both with and without a correction method to account for urea exchange during the lavage procedure itself. The 99mTc-DTPA and urea techniques were applied to the evaluation of cefepime penetration into this compartment atsteady-state plasma concentrations, in both normal and acutely injured lung. The relevance of measuring cefepime penetration in normal lung can be questioned, since alveolocapillary barrier permeability can dramatically increase in lung inflammation. Therefore, the impact of acute lung injury on cefepime penetration in ELF was evaluated by measuring blood/airspace clearance rates in both normal and injured lung. The main findings of the present study were that CELF,cefepime reach steady-state plasma concentrations 5 h after the beginning of infusion in both normal and injured lung, in anaesthetised dogs. When urea is used as an endogenous marker of ELF dilution, CELF,cefepime are generally underestimated. This underestimation increases as lavages are repeated in normal lung, due to rapid diffusion of urea into the lavage fluid. Cefepime concentrations are underestimated less in the presence of increased alveolocapillary barrier permeability. In acute lung injury, the large increase in cefepime blood/airspace clearance suggested much faster penetration from blood to ELF.
Five hours after the beginning of administration, the CELF,cefepime was very close to the plasma concentration, based on method A. The present results are similar to those of Breilh et al. 13, who recently reported a cefepime concentration of 101% of steady-state plasma concentrations in lung biopsy specimens from patients undergoing thoracic surgery. More recently, Boselli et al. 14 measured CELF,cefepime at steady state after 48 h of continuous intravenous infusion in patients with severe nosocomial bacterial pneumonia. The authors found a mean cefepime penetration into ELF of 100%, using a microlavage technique with endogenous urea as indicator. To the present authors' knowledge, this is the only study on cefepime penetration in ELF at steady state. Although these results were obtained by identical means to the measurement of ELF penetration by method A in the present study, they are ∼25% higher than the present estimates in injured lung using urea, although direct comparison is difficult due to differences in lavage technique, experimental model and timing. Equilibration of CELF,cefepime with plasma cefepime concentrations is compatible with the limited cefepime serum protein-binding of 17% in rat 15 and 12.5–14.5% in dog 16. In the present study, CELF,cefepime/plasma cefepime concentration ratios were not different in normal versus injured lung, despite different plasma concentrations. The present authors are not aware of any other systematic comparison of the ELF penetration of cefepime in normal versus injured lung. Higher plasma cefepime concentrations in injured versus normal lung may be explained by altered glomerular filtration in these acutely ill animals, prolonging the blood elimination half-life. Conversely, the haemoconcentration that occurs as a consequence of fluid extravasation during oedema formation may contribute to higher blood concentrations in animals with acute lung injury.
When urea was used to calculate CELF,cefepime, lower concentrations and CELF,cefepime/plasma cefepime concentration ratios were found compared to the 99mTc-DTPA method. This includes the CELF,cefepime and ELF/plasma ratios calculated using method C, which accounts for urea exchange during the lavage procedure. An interesting point is that CELF,cefepime using urea as an endogenous indicator was far less underestimated in injured lung than in normal lung. A possible explanation is the fact that, at the end of the first lavage, the urea concentration in BALF was 57.0±12.9% that of plasma in injured versus 7.3±1.5% in control lung. The much shallower urea concentration gradient in injured lung may explain the much slower urea exchange rate into the BALF, if it is assumed that urea exchange across the blood/airspace barrier is mainly diffusive 17, 18. Urea exchange, across the alveolocapillary barrier occurred quite rapidly in uninjured lung (fig. 2b⇑), as shown previously 18. The urea permeability of artificial bilayer membranes is relatively low 19; however, it has been known for some time that urea transport in human red blood cells occurs largely by facilitated diffusion 17, which may also be present in the alveolar and airway epithelium 17. Owing to this fast diffusion across cell membranes, unlike chelates such as DTPA, urea may not be considered an appropriate extracellular indicator. This may explain why the underestimation of cefepime concentrations was only partially corrected by back-extrapolation using method C in normal lung, the urea dilution space being much larger than the ELF compartment alone. The fact that the use of urea as an endogenous indicator leads to underestimation of solute concentrations in ELF has previously been reported 2, 20. Based on this finding, the use of 99mTc-DTPA was initially suggested by Feng et al. 21. Some investigators have used single lavage cycles with a short fluid dwell time (<20 s) in order to limit urea diffusion into the BAL fluid 22. Shortening the lavage fluid dwell time decreases the error in the estimation of ELF dilution by BAL fluid, by reducing urea exchange during lavage. However, it has been shown that the first aliquot of instilled fluid samples only the proximal airways, and that the peripheral airspaces of a lung segment are filled more evenly as lavage cycles are repeated 23. In light of this fact, Baldwin et al. 24 have proposed a “microlavage” technique using a standard bronchial brush tube for rapid lavage of a peripheral lung subsegment. Comparison of this technique with conventional lavage by these authors has shown that microlavage yields lower VELF. This may be an explanation for the differences in cefepime ELF penetration based on urea measurements in the present study versus those reported by Boselli et al. 14.
Following oleic acid-induced acute lung injury, a large increase in 99mTc-DTPA blood/airspace clearance was observed. This is consistent with a previous observation that oleic acid induces a several-fold 99mTc-DTPA blood/airspace clearance elevation along with an increase in extravascular lung water but unchanged pulmonary wedge and capillary pressures 9, due to the increased alveolocapillary permeability known to occur in this model. In the present study, cefepime blood/airspace clearance increased by a similar magnitude to that of 99mTc-DTPA, suggesting that penetration from blood to ELF is greatly enhanced in an acutely inflamed lung. In critically ill patients with high alveolocapillary barrier permeability based on BALF albumin concentrations, vancomycin ELF penetration, as estimated by the urea method and conventional lavage, was nearly twice that of patients with low permeability 25. Further study with repeated BAL sampling should allow better determination of the differences in cefepime blood/ELF kinetics under conditions of normal versus increased alveolocapillary permeability.
Overall, the present study shows the feasibility of saturation bronchoalveolar lavage for quantifying epithelial lining fluid concentrations of pharmacological agents in dog lung, and suggests that the method should be more widely examined as it may provide more accurate measures of epithelial lining fluid volume and solute concentration than current methodology. Comparison with currently used methods shows that using urea as an endogenous indicator is much less erroneous in injured lung, and that single cycle “microlavage” techniques appear the best alternative for bedside application in an acutely inflamed lung.
Appendix: Calculations
A detailed description of all calculation methods can be found elsewhere 4, 9.
Lavage fluid volume
The total volume of fluid in the lavaged segment at end-instillation in lavage cycle n (Vtot,n) was calculated for each of the six bronchoalveolar lavage (BAL) cycles from the concentration in the retrieved BAL fluid (BALF) (Cret,n) of fluorescein isothiocyanate-labelled dextran (2,000 kDa) (FITC-D2000) (Cret,n,FITC-D2000):  where Qn is the quantity present in the lavaged lung segment in lavage cycle n, in this case of FITC-D2000 (Qn,FITC-D2000). Originally, 125I-albumin was used as alveolar indicator 4. In preliminary experiments in three dogs, 125I-albumin and FITC-D2000 were used simultaneously, and the use of FITC-D2000 for measurement of Vtot,n was validated against 125I-albumin. Qn,FITC-D2000 is the sum of the amounts of FITC-D2000 added (Qadd,n,FITC-D2000) at each lavage cycle, minus the amounts removed through sampling of the BALF (Qs,n,FITC-D2000):
where Qn is the quantity present in the lavaged lung segment in lavage cycle n, in this case of FITC-D2000 (Qn,FITC-D2000). Originally, 125I-albumin was used as alveolar indicator 4. In preliminary experiments in three dogs, 125I-albumin and FITC-D2000 were used simultaneously, and the use of FITC-D2000 for measurement of Vtot,n was validated against 125I-albumin. Qn,FITC-D2000 is the sum of the amounts of FITC-D2000 added (Qadd,n,FITC-D2000) at each lavage cycle, minus the amounts removed through sampling of the BALF (Qs,n,FITC-D2000):  In normal lung, after three lavage cycles, Vtot,n reaches a plateau and does not change significantly from the third to the sixth lavage cycle, at which point the lung segment is considered at “saturation” 9.
In normal lung, after three lavage cycles, Vtot,n reaches a plateau and does not change significantly from the third to the sixth lavage cycle, at which point the lung segment is considered at “saturation” 9.
Method A: ELF volume and cefepime concentration using 99mTc-DTPA as indicator
Technetium-99m diethylenetriaminepenta-acetic acid (99mTc-DTPA) was infused at constant blood concentration for 5 h prior to lavage, in order for the activity in epithelial lining fluid (ELF) to equilibrate with that in plasma. The Qn of 99mTc-DTPA (Qn,99mTc-DTPA=Vtot,n·BALF 99mTc-DTPA activity) increases with time due to diffusion from plasma into the alveoli during lavage 9. A best-fit line is adjusted to Qn,99mTc-DTPA expressed as a function of time from beginning of lavage. This best-fit line is extrapolated to time zero (Q0), when 99mTc-DTPA activity (Q0,99mTc-DTPA) was not affected by lavage. ELF volume (VELF) is then calculated from 99mTc-DTPA activity (VELF,99mTc-DTPA) as follows:  where Čp is steady state plasma concentration, in this case of 99mTc-DTPA (Čp,99mTc-DTPA). Q0 of cefepime (Q0,cefepime) is calculated in the same way as for 99mTc-DTPA. Cefepime concentration in ELF (CELF,cefepime) is then calculated as follows:
where Čp is steady state plasma concentration, in this case of 99mTc-DTPA (Čp,99mTc-DTPA). Q0 of cefepime (Q0,cefepime) is calculated in the same way as for 99mTc-DTPA. Cefepime concentration in ELF (CELF,cefepime) is then calculated as follows: 
Method B: ELF cefepime concentration using endogenous urea as indicator
For comparison, endogenous urea was used as an indicator to estimate CELF,cefepime using the method described by Rennard et al. 11. This method is based on the assumption that, since urea diffuses readily through body compartments, urea concentrations in plasma and ELF are identical. CELF,cefepime is then calculated as follows:  where Čp,urea is Čp of urea and Cret,n,cefepime and Cret,n, urea the Cret,n of cefepime and urea respectively. By this method, CELF,cefepime can be estimated for each lavage cycle, or based on the mean urea concentration in the BALF of all six lavage cycles, as is the case when the retrieved lavage fluid from multiple BALs is pooled. Alternatively, CELF,cefepime can be calculated by the same method, but based on the first lavage Cret,n,cefepime alone. This method was subsequently named “single-cycle” lavage.
where Čp,urea is Čp of urea and Cret,n,cefepime and Cret,n, urea the Cret,n of cefepime and urea respectively. By this method, CELF,cefepime can be estimated for each lavage cycle, or based on the mean urea concentration in the BALF of all six lavage cycles, as is the case when the retrieved lavage fluid from multiple BALs is pooled. Alternatively, CELF,cefepime can be calculated by the same method, but based on the first lavage Cret,n,cefepime alone. This method was subsequently named “single-cycle” lavage.
Method C: ELF volume and cefepime concentration using endogenous urea as indicator with correction for urea diffusion
The Qn of urea (Qn,urea=Vtot,n·Cret,n,urea) increases with time due to diffusion from plasma into the alveoli during lavage. Alternatively, a correction method to account for urea diffusion, similar to the above method for 99mTc-DTPA, can be proposed, in which a linear fit of Qn,urea as a function of time from beginning of lavage is back-extrapolated to time 0 to give VELF (VELF,urea):  Q0 of urea (Q0,urea) is calculated by extrapolation to time zero of a linear fit of Qn,urea as a function of time from beginning of lavage. CELF,cefepime can then be calculated using this correction (CELF,cefepime,urea):
Q0 of urea (Q0,urea) is calculated by extrapolation to time zero of a linear fit of Qn,urea as a function of time from beginning of lavage. CELF,cefepime can then be calculated using this correction (CELF,cefepime,urea): 
Blood/airspace clearance
Alveolocapillary solute clearance in lavage cycle n (cln; in microlitres per minute) of cefepime (cln,cefepime) is calculated as follows:  where Qn,cefepime is the Qn of Cefepime (in micrograms), Č p,cefepime is the Čp of cefepime and t is the time (in minutes) from the beginning of cefepime infusion. The cln of 99mTc-DTPA can be calculated in the same way. Blood/airspace clearance at saturation (CL) was defined as the mean alveolocapillary clearance from the third to the sixth lavage cycle:
where Qn,cefepime is the Qn of Cefepime (in micrograms), Č p,cefepime is the Čp of cefepime and t is the time (in minutes) from the beginning of cefepime infusion. The cln of 99mTc-DTPA can be calculated in the same way. Blood/airspace clearance at saturation (CL) was defined as the mean alveolocapillary clearance from the third to the sixth lavage cycle: 
Acknowledgments
Propofol® was generously donated by Astra Zeneca France (Rueil-Malmaison, France).
- Received September 18, 2003.
- Accepted February 5, 2004.
- © ERS Journals Ltd
References









