





Case history
A 37‐yr‐old male complained of a dry cough, fever, nocturnal sudation and dyspnoea. On lung auscultation, his general practitioner noticed right-sided expiratory wheezing and the diagnosis of tracheitis was withheld. Clarithromycin and a cough syrup were given and a slight amelioration was noticed, except for the persistence of dry cough. Bronchial hyperreactivity was suspected and a combination of budesonide and formoterol was added to the treatment.
During the following 2 months, symptomatology varied; cough and dyspnoea were intermittently present until the patient started complaining of right thoracic pain and important fatigue. Fever re-appeared reaching 39°C, and, after consulting his general practitioner, cefuroxime and paracetamol were prescribed.
Once again the fever disappeared, but a very invalidating cough with mucopurulent sputum, fatigue and chest pain persisted. After the antibiotic was stopped, fever reappeared and the patient was hospitalised.
In his past history the patient was treated at the age of 12 yrs by immunotherapy for an allergic rhinitis caused by dust allergy. There was no particular familial history. He had never smoked and worked in an office.
On clinical examination, the patient was pale, sweaty and thin. His blood pressure was 125/65, pulse 100·min−1 and temperature 38.7°C. On lung auscultation, breath sounds were diminished at the right lung base. Otherwise, physical examination was normal.
Laboratory studies demonstrated a white blood cell count of 16×109·L−1, with 83% neutrophils, haemoglobin 131 g·L−1, platelets 130 1×109·L−1 and CRP 120 mg·L−1. Liver tests, renal and serum chemistry were normal.
A chest radiography and a CT scan of the lungs and mediastinum were performed (figs 1 and 2⇓⇓).

Chest radiography.

CT scan.
Flexible bronchoscopy showed a polypoid, necrotic, highly vascularised tumour occluding the right bronchus intermedius. No biopsies were taken, but instead a diagnostic and therapeutic rigid bronchoscopy was performed. The endobronchial tumour is shown in figure 3⇓. The biopsy is shown in figures 4 and 5⇓⇓.

Rigid bronchoscopy showing an endobronchial tumour in the right bronchus intermedius.

Biopsy of the tumour (haematoxylin and eosin staining). Scale bar=25 µm.
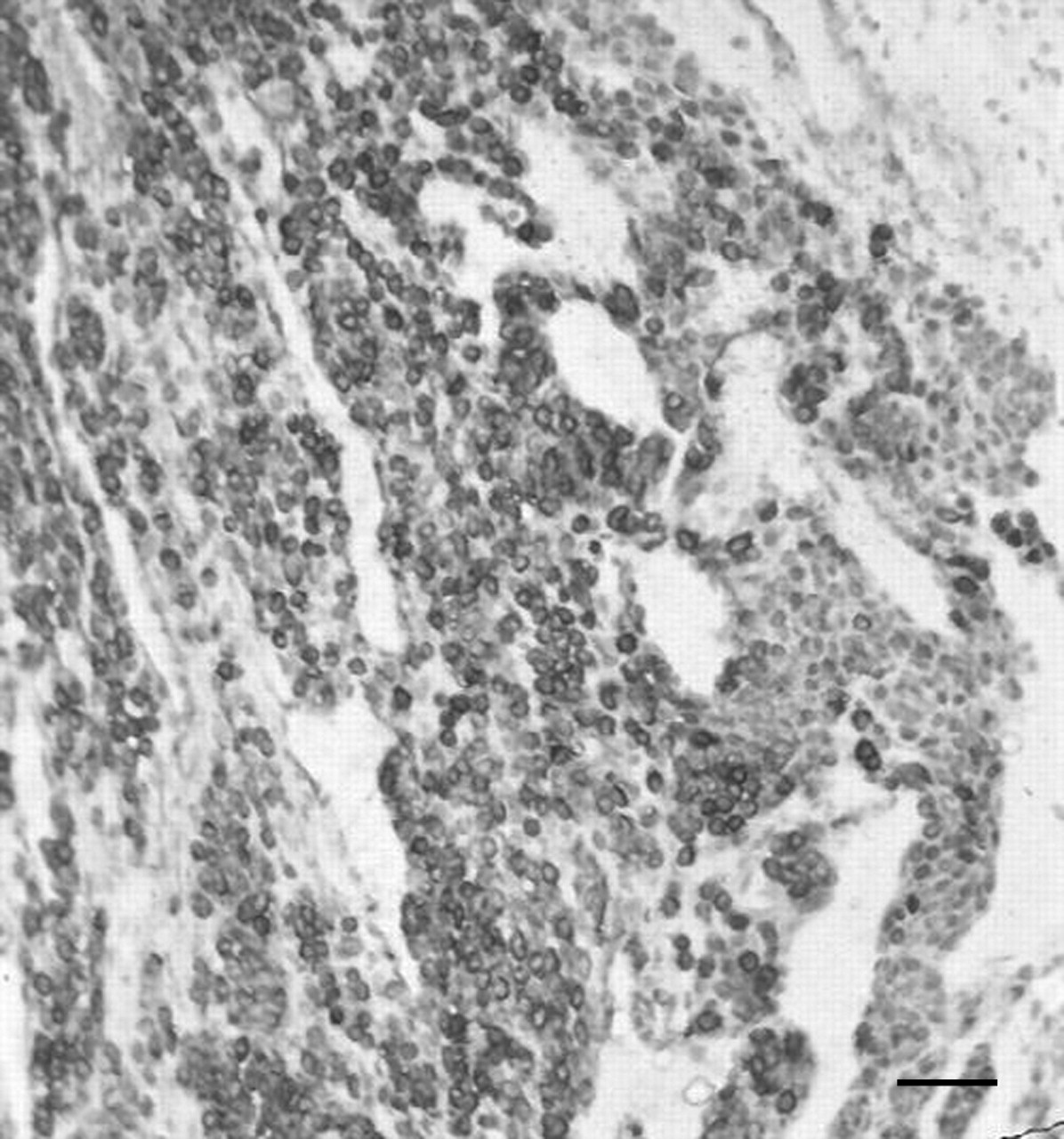
Biopsy of the tumour (cytoplasmatic smooth muscle actin staining). Scale bar=25 µm.
BEFORE TURNING THE PAGE INTERPRET THE CHEST RADIOGRAPHY, THE CT SCAN AND THE PHOTOGRAPHS, AND SUGGEST A DIAGNOSIS.
Interpretation
Chest radiography
Chest radiography of the lungs shows an infiltrate of the basal part of the right lung. This is secondary to the endobronchial tumour seen on the CT (fig. 2⇑).
CT
The chest CT scan (fig. 2⇑) shows an endobronchial tumour of the right bronchus intermedius without infiltration through the bronchial wall. This is not visible on the chest radiograph.
Pathology
Haematoxylin and eosin staining yielded a tumour composed of uniform cells patched together, although there were some areas where the tumour cells were separated by myxoid of fibrinous stroma.
Vascular structures were present. The tumour cells were composed of a pale cytoplasm with well-defined cell borders and regular cores. No mitosis or cellular atypia were seen. In some areas the tumour cells evolved to smooth muscle cells.
The tumour cells stained positive for vimentine and actin, and negative for the neuro-endocrine markers synaptophysine and chromogranine, cytokeratin (used to rule out epithelial tumours), and cD34 and cD31 (markers that highlight the vascular nature of the tumour).
Diagnosis : “Endobronchial glomus tumour with associated postobstructive pneumonia”
Clinical course
After rigid forceps biopsy, ND‐YAG laser was used to coagulate the tumour. Thereafter, the tumour was cored out and removed mechanically with the tip of the bronchoscope. A flow of postobstructive pus was aspirated. The pedicle of the tumour remained in the superior segment of the right lower lobe and was treated with cryotherapy after biopsies were taken. At the end of the procedure, a clean-up bronchoscopy using a flexible scope was performed.
After mechanical resection of the endobronchial glomus tumour, the postobstructive pneumonia healed and the patient recovered. The chest radiography normalised completely.
A flexible bronchoscopy was performed 1 month later. The tumour pedicle was still present at the entrance of the superior segment of the right lower lobe. Biopsies were taken and pathology confirmed the persistence of glomus tumour tissue.
At 3 months follow-up, the chest radiography remains normal and the patient is asymptomatic. He is followed by flexible bronchoscopy on a regular basis.
If the tumour volume increases, a new endoscopic treatment will be proposed to the patient.
Discussion
Glomus tumour is a benign tumour derived from glomus cells. These glomus cells are found in a specialised form of arteriovenous anastomosis called a glomus body and serve in thermal regulation 1. Ultrastucturally, glomocytes have features of smooth muscle 2. They are relatively common cutaneous tumours usually seen in the subungual area of the finger 3. Sometimes they occur deeper in muscles, tendons, ligaments and periosteum 4. Glomus tumours are extremely rare in visceral organs, such as the stomach, rectum, heart, uterus, mediastinum, kidney and lung 1, 3. Within the respiratory tract, the trachea is the most frequent site of involvement. Only a few cases of endobronchial glomus tumours have been described previously 1.
The most common symptoms in glomus tumours of the lung and respiratory tract are cough, haemoptysis, dyspnoea, stridor and hoarseness 1, 5, 6, 8, 11.
The differential diagnosis of a glomus tumour includes carcinoid tumour and haemangiopericytoma. Immunohistochemically, glomus tumours stain positive for musclespecific actin and vimentine 5.
There is no consensus regarding the treatment of bronchial or tracheal glomus tumour. Most tracheal glomus tumours are treated by excision and end-to-end anastomosis of the trachea with good results 6–8. In bronchial glomus tumours, bronchoplasty can be performed but since the development of endobronchial treatment, ND‐YAG coagulation has been performed with good results at 1‐yr follow-up 11, 12. One patient received adjuvant radiotherapy after lasercoagulation 11, also with good results.
In the present case, the initial handling and treatment done by the general practitioner can be questioned, as well as the fact that no chest radiography was performed during the 2 months prior to his hospitalisation.
After treatment of his retro-obstructive pneumonia, the less invasive endobronchial treatment was preferred over open surgery because the tumour was confined within the bronchial lumen and wall. ND‐YAG laser was first used to coagulate the vascularised polypoid part of the tumour, and with the aid of the rigid bronchoscope, almost the entire tumour was removed. Cryotherapy was used on the pedicle of the tumour because of the well-vascularised remaining structure and because there was no critical stenosis of the bronchus.
To the current authors’ knowledge, this is the first time cryotherapy has been used on glomus tumours. However, 1 month later the foot of this tumour was still present and again biopsy confirmed the persistence of glomus tumour, which suggests that cryotherapy may not be efficient therapy for bronchial glomus tumour. Since normal ventilation of the superior segment of the right lower lobe is preserved, this patient was followed-up regularly with bronchoscopy and chest radiography.
- Received September 23, 2003.
- Accepted November 10, 2004.
- © ERS Journals Ltd










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}