





Case history
In 1994 a 44-yr-old male was admitted for surgical resection of a hard, not painful, nodule which was believed to originate from the isthmus of the thyroid gland. He was known to have mild asthma, treated with inhaled corticosteroids and short-acting β2-agonists. His medical record revealed a smoking history of 20 pack-yrs. The patient denied any other symptoms, except the presence of the nodule.
On physical examination a hard nodule was felt anteriorly to the trachea. A clear separation with the thyroid gland could not be made.
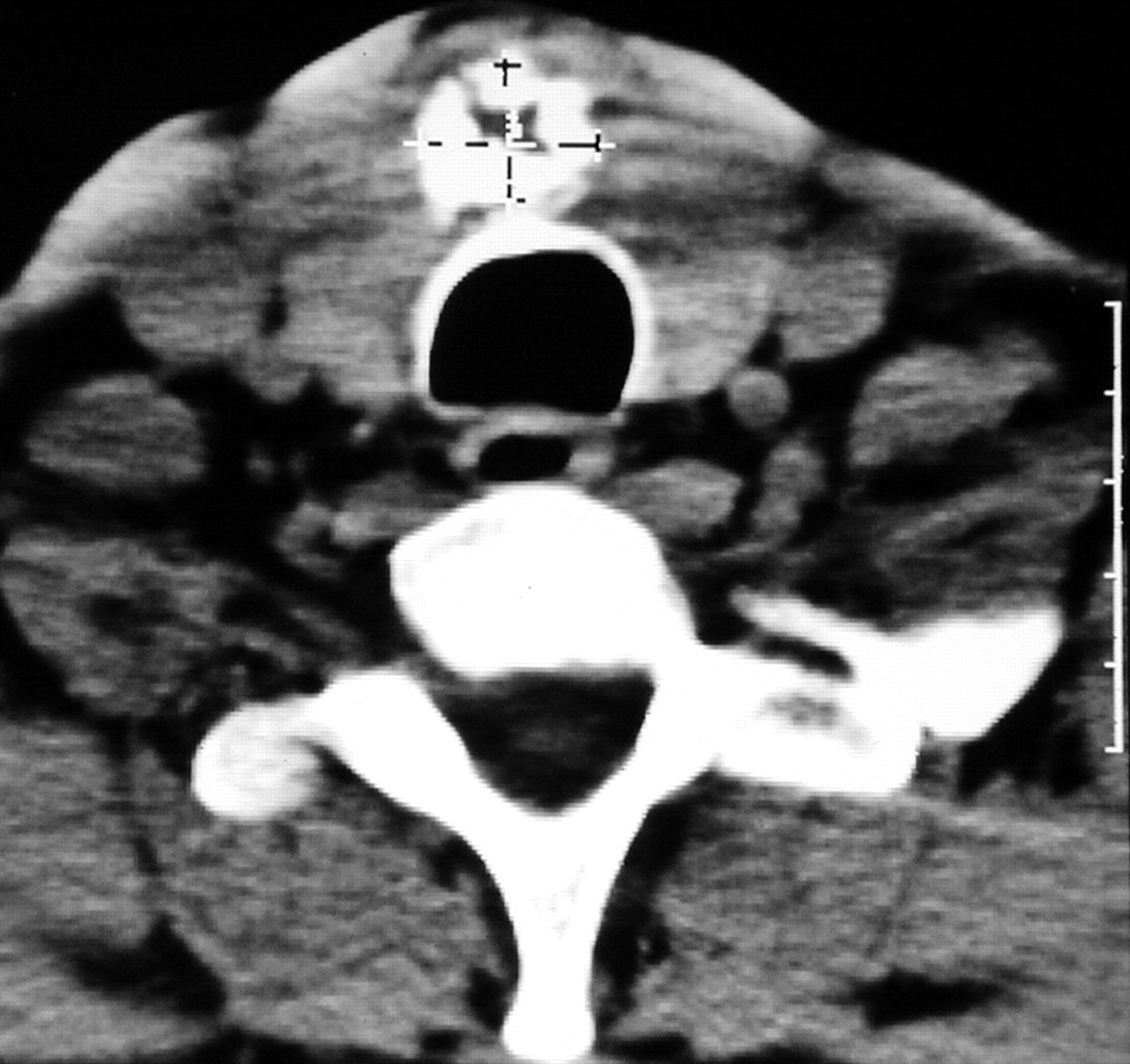
A preoperative computed tomography (CT) scan of the neck revealed a calcified nodule on the midline, adjacent to the trachea (fig. 1⇓). Laboratory studies demonstrated a euthyroid status.

Chest computed tomography scan. Internal scale bar=5 cm.
During surgery, the nodule could not be separated from the tracheal cartilaginous ring and a left hemithyroidectomy, with resection of part of the affected cartilaginous ring, was carried out (histology of the nodule in fig. 2a⇓). The tracheal defect was closed with a muscle flap. The patient continued to do well on follow-up examinations ≤5 yrs postoperatively, without complaints. Repeated bronchoscopy examinations confirmed the tracheal integrity. After 5 yrs the patient was lost to follow-up.

Histology of the first resection. a) haemotoxylin-eosin stain and the recurrence. b) immunohistochemistry for Ki 67. Internal scale bar=10 µm.
Seven years after his first operation the patient reported cough, blood-speckled sputum and dyspnoea on exertion.
Physical examination revealed inspiratory wheezes (stridor) over the cervical trachea.
Spirometry with flow/volume loop analysis (fig. 3⇓), bronchoscopy (fig. 4⇓) and a CT scan of the neck (fig. 5⇓) were performed. The histology of the resection specimen is shown in figure 2b⇑.

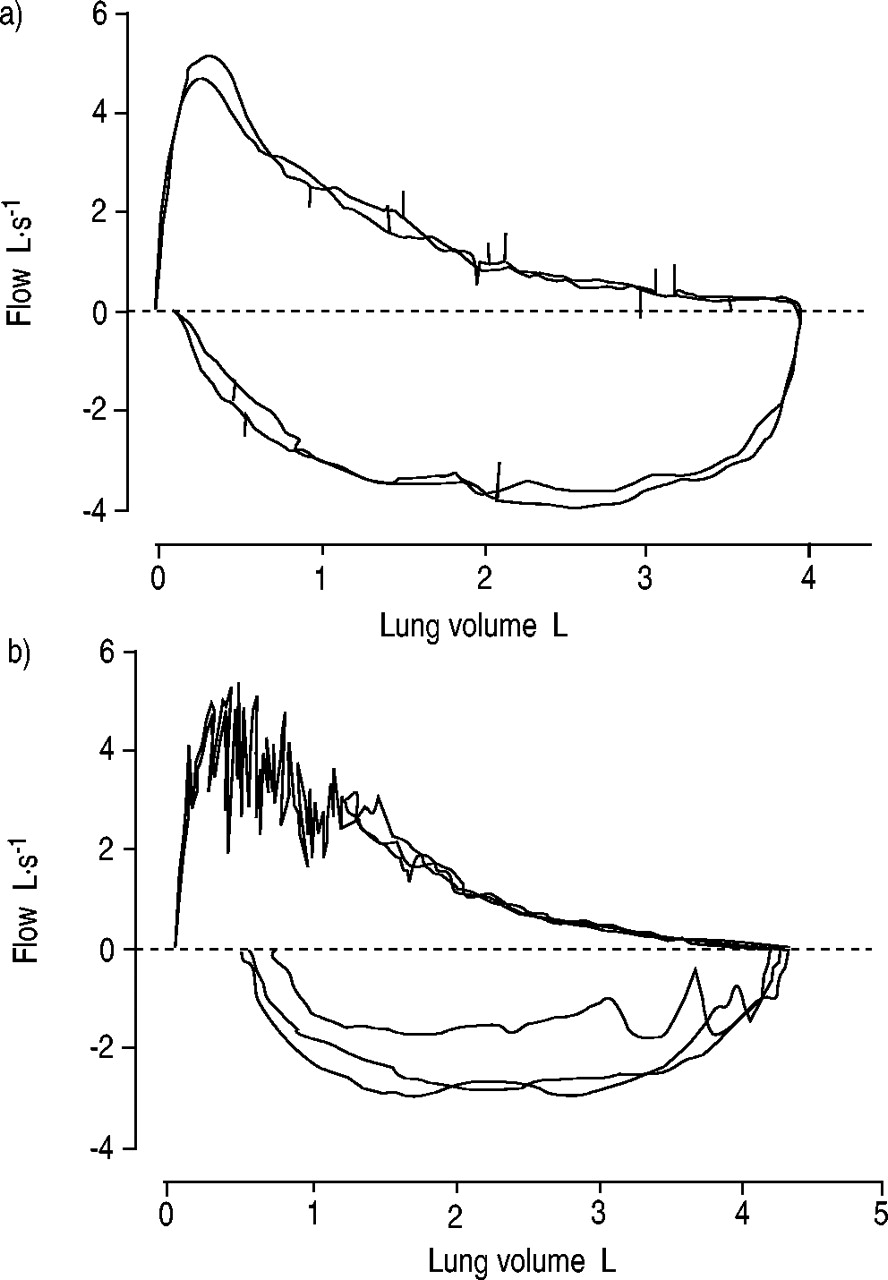
Flow/volume loops performed a) a few years before the admission and b) during the last admission. The loop with positive values is the expiratory flow/volume loop and the loop with negative values is the inspiratory flow/volume loop.

Bronchoscopic view of the trachea.

Chest computed tomography scan.
BEFORE TURNING THE PAGE, INTERPRET THE COMPUTED TOMOGRAPHY SCANS (FIGS. 1 AND 5⇑⇑), THE FLOW/VOLUME LOOPS (FIG. 3⇑), THE BRONCHOSCOPIC IMAGE (FIG. 4⇑) AND THE RESECTION SPECIMENS (FIG. 2⇑), AND SUGGEST A DIAGNOSIS.
Interpretations
Computed tomography
The initial neck CT scan shows a calcified mass, adherent to the tracheal wall, exterior to the tracheal lumen (fig. 1⇑). A multilobulated mass, with foci of calcification in the tracheal lumen, was seen 7‐yrs later (fig. 4⇑). There is no lymph-node enlargement.
Flow/volume loops
The flow/volume loop taken 4 yrs before readmission is normal, except for a slight loss of the end-expiratory flows (asthma). The flow/volume loops, taken before endoscopic laser resection, show upper airway instability (fluttering on the expiratory flow/volume loop) and a flattened inspiratory flow/volume loop, suggestive of upper-airway obstruction.
Bronchoscopic image
Figure 3⇑ shows a multilobulated mass with capillary distension and normal looking overlying mucosa, extending in the tracheal lumen for ∼3 cm.
Pathology
Both histological images (fig. 5⇑) show a similar morphology. The tumour is composed of mature chondrocytes. Enlarged or binucleated cells are absent. There are no foci of proliferation. The latter is confirmed by the negative immunohistochemistry for the Ki 67 antigen.
Diagnosis: Primary tracheal chondroma
Clinical course
An endoscopic-laser resection of the pedunculated mass was performed. The patient received a self-expandable covered metallic stent. Unfortunately, the stent dislodged a few weeks later, provoking respiratory distress with vocal-cord oedema. Under general anaesthesia the stent was removed and a silicon stent was inserted. The postoperative outcome was complicated by a transient ischaemic attack with left-sided hemiplegia, but the patient recovered completely. A follow-up bronchoscopy showed a fully opened tracheal lumen (fig. 6⇓).

Bronchoscopic view of the trachea after therapeutic intervention.
Discussion
Primary tracheal chondroma is a rare benign disease, originating from the hyalineous cartilaginous rings of the trachea. These rare tracheal tumours have been distributed evenly among the upper, middle and lower thirds of the trachea. In reported cases, age ranged 50–70 yrs and all patients were male. No definite causes have been related to the development of these tumours. Tracheal chondromas will present most commonly with dyspnoea or chronic cough and stridor in the case of substantial narrowing of the tracheal lumen 1, 2. The patient presented the first time with an indolent pretracheal nodule. The recurrence episode was characterised by dyspnoea and cough, as well as stridor.
Endoscopic exploration is essential for diagnosis and biopsy of the intratracheal proliferation. A CT scan is of help to determine the extent of the tumour into the surrounding structures. The presence of the amorphous calcifications, which are present in 75% of the reported cases, may indicate the cartilagenous nature of the tumour 3. Differential diagnosis includes other benign causes of an endotracheal mass. With decreasing frequency, fibroma, haematoma, angioma and osteoma are noted. Squamous-cell carcinoma of the trachea and adenoid-cystic carcinoma are the most frequent malignant tracheal tumours. Recurrent and malignant (sarcomatous) transformation of these chondromas are the most feared complications 4, 5.
Surgical resection is regarded as the mainstay of treatment. Bronchoscopic resection is another option. The best indications for bronchoscopic treatment of benign tumours of the tracheobronchial tree are: strictly intraluminal location of the tumour, limited extent within the lumen of the trachea, low probability of recurrence and poor surgical candidates. In addition, patients reluctant to undergo further surgery, as in the patient in the current study. Cavalieri et al. 6 reported no recurrence in 103 endoscopically controlled cases of a total of 151 cases of benign endobronchial tumours (nine chondromas) selected for laser resection with curative intent (mean follow-up 24 months, range 6–192 months).
- © ERS Journals Ltd










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}