





Abstract
The prevalence of asthma has been on the increase in the USA and worldwide. To understand the worsening epidemiological trends of asthma, this study analysed the data from the third National Health and Nutrition Examination Survey (NHANES III) to determine the prevalence and risk factors for asthma and wheezing among US adults.
This analysis used data from 18,825 US adults aged ≥20 yrs who had participated in the NHANES III project. After excluding subjects with physiciandiagnosed emphysema, a total of 18,393 subjects were included in the final analysis.
The prevalence of current asthma (asthma) was 4.5% and the prevalence of wheezing in the previous 12 months (wheezing) was 16.4%. MexicanAmericans exhibited the lowest prevalence of asthma when compared with other race/ethnic groups. Multiple logistic regression analysis showed that MexicanAmericans were less likely to report asthma when compared to nonHispanic whites. Low education level, female sex, current and past smoking status, pet ownership, lifetime diagnosis of physiciandiagnosed hay fever and obesity were all significantly associated with asthma and/or wheezing. No significant effect of indoor air pollutants, as derived from the use of household heating/cooking appliances, on asthma and wheezing was observed in this study.
In conclusion, this study observed racial/ethnic differences in the prevalence of asthma and wheezing and identified several important risk factors that may contribute to development and/or exacerbation of asthma and wheezing. Contrary to earlier reports, the proxy measures of indoor air pollution used in this study were not found to be associated with increased risk of asthma and wheezing.
The incidence, prevalence and severity of asthma have been increasing in the general population, both worldwide and in the USA, for the past two decades 1. There are ∼14 million people in the USA suffering from asthma. The prevalence of selfreported asthma increased by 75% in the USA from 1980–1994 and the states with the highest prevalence of selfreported asthma were California (7.1%) New York (6.8%) and Texas (6%) 2. In the largest asthma prevalence survey conducted to date, the European Community Respiratory Health Survey (ECRHS), an overall prevalence of 4.5% in adults aged 20–44 yrs was found. However, there was considerable variation among the 22 countries studied 3.
In the absence of any gold standard, and because of the variable nature of the disease, accurate case findings of asthma, outside of the clinical setting, is very challenging. A variety of methods have been used in epidemiological surveys to define asthma: self reports of physiciandiagnosed asthma 4, 5, presence of asthma symptoms, such as wheezing 5, combination of asthma symptoms, e.g. discriminate function predictors 5, or objective measurements like spirometry 6 or use of methacholine or histamine for testing bronchial responsiveness 5, 7. Each approach may lead to selection of different study groups with asthma, thereby reporting results that may not be comparable. Although, largescale epidemiological surveys, such as the ECRHS, have been conducted using nonspecific bronchial challenge 3, the cost and technical skills involved remain a limiting factor in their widespread use. Hence, questionnairebased selfreports of asthma remain the most commonly used approach for defining asthma in epidemiological surveys.
The National Health and Nutrition Examination Survey (NHANES) provided a rich populationbased dataset to identify determinants of asthma and wheezing. This study analysed the data gathered from the third, and most recent, round of the NHANES, to estimate the prevalence and determine the risk factors for adult asthma and wheezing in this population.
Materials and methods
The National Center for Health Statistics (NCHS) conducts several largescale surveys to assess the general health status of the USA's general population. Data from the NHANES III, which was conducted by NCHS from 1988–1994, was used. Detailed descriptions of the stratified cluster sampling strategy have been described elsewhere 8. This survey gathered information regarding the health status of ∼40,000 American individuals, aged ≥2 months old with no preset upper age limit. In order to obtain reliable estimates of the health status of different population subgroups, younger children, older persons, MexicanAmericans and AfricanAmericans were sampled in large numbers. The overall response rate in the NHANES III was 82% (80% for Whites, 86% for Blacks, and 87% for MexicanAmericans) 9.
Study population and outcome variables
The analyses involved using data from the 18,825 adults aged ≥20 yrs and who were interviewed in the NHANES III project. In this analysis two outcome variables, asthma and wheezing, were used. Current asthma (asthma) was defined as an affirmative response to the question “Has a doctor ever told you that you had asthma?” and “Do you still have asthma?” Wheezing was defined as an affirmative response to the question “Have you had wheezing or whistling in your chest at any time in the past 12 months?” Subjects who responded in the affirmative to the following question “Has a doctor ever told you that you had emphysema?” (item HAC1G in NHANES III, n=432) were excluded from the analysis.
Independent variable selection
Independent variables included in the analysis were selected based on risk factors reported in the literature, and classified into five broad conceptual categories: 1) demographic i.e. age, sex, race/ethnicity, urban/rural, and census region; 2) socioeconomic i.e. education and poverty income ratio; 3) indoor air quality based on the response to a limited number of questions on the use of a space heater, furnace, or oven to heat the home; 4) allergy, hay fever; and 5) other characteristics i.e. smoking history, body mass index (BMI), and family and household size.
Statistical analysis
Since the NHANES III uses a complex survey design, a statistical package (STATA statistical software; Stata Inc., College Station, TX), which allows users to incorporate sampling weights and compute sampling variances, was used for the analysis. Simple descriptive statistics were used to describe the study population, followed by univariate and multivariate analyses using logistic regression to explore the association between independent variables and the outcome variable. Separate univariate and multivariate models were built using asthma and wheezing as the outcome variable. All variables significant at p<0.1 were considered for inclusion in the final model. Multiple logistic regression analysis was used to simultaneously adjust for the various independent variables. Estimated crude odds ratios (ORs), and adjusted ORs with their corresponding 95% confidence intervals (CI) were calculated.
Results
Based on the study inclusion and exclusion criteria, a total of 18,393 study subjects aged ≥20 yrs were included in the analysis. Table 1⇓ describes the weighted percentage of the respondents by selected demographic and housingrelated variables. The prevalence of asthma was 4.5%, while wheezing was reported as 16.4%. The prevalence of asthma and wheezing did not differ significantly across different age groups (table 2⇓). When restricted to age group 20–44 yrs (as used in the ECRHS), the prevalence of asthma was 4.7 % (95% CI 4.0–5.5) and the prevalence of wheezing was 17.5% (95% CI 16.3–18.6).
Demographic and housing characteristics of study subjects aged ≥20 yrs from the National Health and Nutrition Examination Survey III 1988–1994
Prevalence of current asthma and wheezing by age group
An estimated 11.4% of the USA population were living below poverty level and an estimated 24.7% had <12 yrs of education (table 3⇓). Approximately 28% of adults were current smokers. The estimated prevalence of obesity (defined as BMI ≥30) among adults was 30%. MexicanAmericans formed the largest ethnic group living below the poverty level. More than onehalf also reported receiving <12 yrs of education (table 3⇓).
Health and social characteristics by race/ethnicity in the National Health and Nutrition Examination Survey III adult study population 1988–1994
MexicanAmericans exhibited the lowest prevalence of asthma (2.9%) when compared with other race/ethnic groups. The prevalence of wheezing was highest among nonHispanic Whites when compared with MexicanAmericans and AfricanAmericans (table 3⇑). The estimated prevalences of other respiratory conditions and symptoms were significantly lower among nonHispanic Blacks and MexicanAmericans than nonHispanic Whites (table 3⇑).
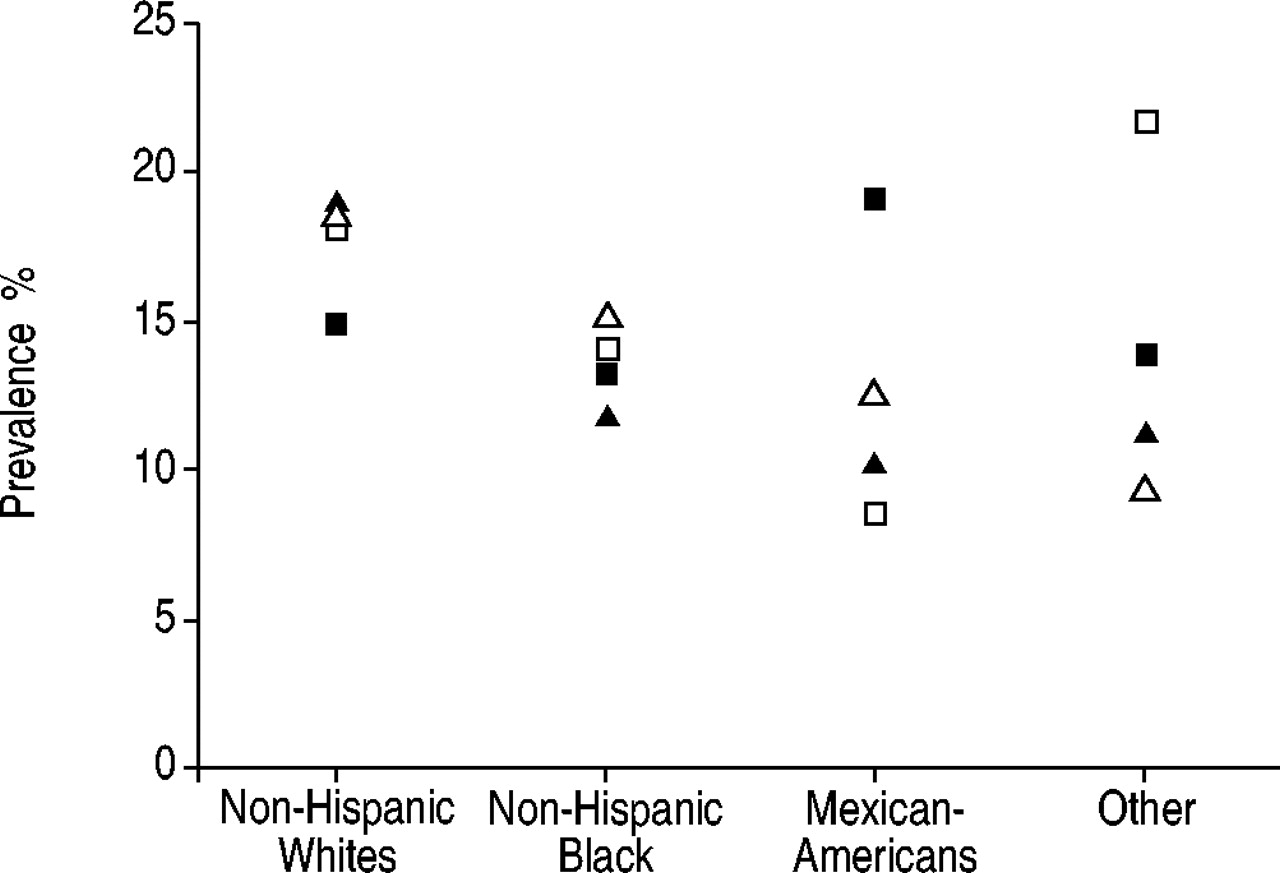
The prevalence of asthma was significantly higher among females (5.4%, 95% CI 4.6–6.2) than males (3.6%, 95% CI 2.8–4.4). No differences, however, were observed for wheezing. The prevalence of asthma and wheezing did not vary significantly by region. However, when the data were stratified by race/ethnicity, an interesting pattern was observed. MexicanAmericans living in the south region of the USA had the lowest prevalence of asthma (1.5%, 95% CI 1.0–2.1) while the other race/ethnicity group (which included other Hispanics and Asian populations) had the highest prevalence in the Northeast (6.5%, 95% CI 1.1–1.9) and Midwest regions (8.8%, 95% CI 3.2–14.4). MexicanAmericans in the Northeast had the highest prevalence of wheezing (19.0%, 95% CI 9.2–28.8), and those in the Midwest exhibited the lowest prevalence (8.6%, 95% CI 4.7–12.4). The other race/ethnic group had the highest prevalence of wheezing in the Midwest region (21.7%, 95% CI 6.2–37.1) (figs 1 and 2⇓⇓).

Estimated prevalence of asthma across four regions of the USA by race/ethnicity in the National Health and Nutrition Examination Survey III adult study population, 1988–1994. ▪: northeast; □: Midwest; ▴: south; ▵: west.
{kind=link}
{kind=link}
Estimated prevalence of wheezing across four regions of the USA by race/ethnicity in the the National Health and Nutrition Examination Survey III adult study population,1988–1994. ▪: northeast; □: Midwest; ▴: south; ▵: west.
The estimated crude and adjusted ORs with 95% CIs for associations between independent risk factors and asthma and selfreported wheezing in the previous 12 months are presented in table 4⇓. MexicanAmericans were 0.61times less likely to report asthma when compared with nonHispanic Whites. Female sex, living below poverty, loweducation level, living in an older house, pet ownership, lifetime diagnosis of physiciandiagnosed hay fever (hay fever) and obesity were all significantly associated with asthma. Current and past smoking history did not show any significant associations with asthma.
Estimated crude and adjusted odds ratios (OR) and 95% confidence intervals (CI) using current asthma and wheezing in the previous12 months as an outcome in the National Health and Nutrition Examination Survey 1988–1994
Race/ethnicity was an important risk factor for wheezing. MexicanAmericans (adjusted OR=0.55) and nonHispanic blacks (adjusted OR=0.58) showed a significantly lower risk for wheezing. Living in the west census region of the USA did not show a significant association in the univariate analysis. However, when adjusted for other variables in the model a statistically significant association was observed (adjusted OR=1.24). Use of a stove/oven for heating by the residence in the previous 12 months showed a 45% increased odds of wheezing in the univariate analysis. This point estimate decreased when adjusted for other variables in the final model, but was retained due to its strong univariate effect. There were no significant differences in the prevalence of asthma and wheezing for the use of stove/ovens between male and females. Owning a pet was also significant in the univariate analysis, however, the effect was diluted and became nonsignificant when adjusted for other variables in the model. A moderate association of BMI with wheezing was observed for both underweight and obese individuals in the univariate analysis. However, the OR increased significantly from 1.30 to 1.52 for obese individuals only. When stratified by sex, no significant differences in the prevalence of asthma and wheezing for obesity were observed. A strong association of wheezing with past and current smoking history was observed in this analysis. Living below the poverty level, and lifetime history of hay fever were also significantly associated with wheezing.
Discussion
The major strength of the present analysis is that it is based on a large representative national sample of the USA population. Few populationbased studies have addressed the prevalence of asthma among adults in the USA.
The results show that the prevalence of current asthma was 4.5% and the prevalence of wheezing was 16.5%. Previously reported prevalence rates of asthma in adults have ranged from below 3% to over 20% 2, 3, 10, 11. In the NHANES II, Turkeltaub and Gergen 11 reported a prevalence of 6.9% and 9.2% among Whites and Blacks, respectively, based on selfreported physician diagnosis of asthma. Janson et al. 3 in a recent review of ECRHS data compared geographical variation in the prevalence of asthma and asthma symptoms in 22 countries. The median prevalence of current asthma was 4.5% (range 2.0–11.9) similar to the results found in this study. In the ECRHS, asthma prevalence was generally higher in Englishspeaking countries. The median prevalence of wheezing was 20.7% (range 4.1–32.0), i.e. slightly higher than what was found in the present study. However, it is difficult to directly compare prevalence rates observed in this study with other reports due to the use of different populations and case definitions.
There was a significantly higher prevalence of asthma, but not wheezing, among females in this study. Asthma and wheeze are generally reported to be higher among male children, but the trend usually reverses around puberty 3, 12–14. It has been suggested that the higher prevalence rates observed among females could partly be due to their smaller airway calibre size 13. Alternately, it may also reflect the tendency among physicians to diagnose a respiratory condition as asthma in females and chronic obstructive pulmonary disorder (COPD) in males 10.
Contrary to earlier reports 10, 15 nonHispanic Blacks did not have a higher risk of asthma in this study. Moreover, nonHispanic Blacks showed less wheezing compared with nonHispanic Whites, and MexicanAmericans showed the lowest risk of asthma and wheezing compared with the other groups. Previous studies from California, New Mexico and Arizona have found a lower risk of asthma and other respiratory diseases among MexicanAmerican adults 6, 16. Results from the Hispanic Health and Nutrition Examination Survey suggested that Puerto Rican children have the highest prevalence of asthma (20.1%) compared with MexicanAmericans (4.5%), nonHispanic Whites (6.4%) and nonHispanic Blacks (9.1%) 15. It has been argued that the lower risk among MexicanAmericans can be explained by differences in socioeconomic status (SES) and access to healthcare. However, in the present study, rates remained significantly lower among MexicanAmericans, even after controlling for SES and other confounding factors.
There were no overall differences in prevalence of asthma and wheezing across regions, although a variation across different race/ethnic groups by region was observed. Earlier reports indicated that the morbidity and mortality of asthma among Puerto Rican Hispanics is highest in the northeastern USA 17. The 1988 National Health Interview Survey also found the highest prevalence of asthma among children younger than 18 yrs of age in the northeastern region of the USA 18. This study found the highest prevalence of asthma was among the other race/ethnic groups and the highest prevalence of wheezing among MexicanAmericans to be in the northeastern USA. In the NHANES III, Hispanics who were not selfreported as MexicanAmerican were included in the other race/ethnic groups category and these should have included Puerto Ricans. Therefore, the possibility of misclassification of Puerto Ricans as MexicanAmericans is not likely to explain the high prevalence of wheezing observed in this region. A variety of factors could explain the decreased risk of asthma among MexicanAmericans. These include genetic/biological factors, differences in health beliefs and behaviours among Hispanic subgroups, protective psychosocial effects, consumption of a diet rich in fruit and vegetables, and differences in migration pattern, favouring a “healthy migrant effect” 17, 19.
The majority of the relatively few studies that have looked at the relationship between asthma and poverty in adults have found an association between low SES and asthma, as was the case in this study. This was also true in the two previous rounds of the NHANES survey 4, 10, 11. Persistent wheeze was also found to be associated with poverty among children, based on parental social class 20. In contrast, Mielck et al. 21 in a review of 24 studies found either no association or negative association of SES with asthma. However, in their own study, the authors found a strong association between poverty and severe asthma (OR 2.37, 95% CI 1.28–4.41). Differences in the measurement of SES and definitions of poverty may be partly responsible for the inconsistent findings.
In this present study, the prevalence of asthma and/or wheezing was affected by various environmental factors. Both current and past smoking, were strong predictors of wheezing, but not of asthma, compared with neversmokers, this was most marked in current smokers. These results did not change when the analysis was restricted to subjects aged 20–44 yrs; this finding is consistent with that of the ECRHS 3. The relationship between smoking and asthma has been a subject of interest and conflicting findings. Thus, several studies have reported an association between smoking and asthma and/or wheezing 3, 22, 23, but others have not 10, 24, 25. Although the harmful effects of maternal smoking on the respiratory system of developing foetuses and children have been well documented 26, no clear cause and effect relationship between smoking and asthma in adults has been established. Cigarette smoke is likely to induce increased permeability of respiratory epithelium, which may result in increased “trafficking” of allergens and other inflammatory cells to submucosal cells resulting in allergic inflammation of the airways 27.
The use of space heaters, furnaces or gas stoves may affect indoor humidity levels, which might indirectly contribute to the growth of house dust mite, especially when malfunctioning. They can also generate oxides of nitrogen, which are oxidant gases and indoor air pollutants. Studies performed in some European countries 28, 29, but not in the USA 30, have reported increased risk of wheezing among females using gas cookers. In the ECRHS, although a positive association was found with gas cooking, this was limited to females and there was considerable variation among countries 3. The results from this study are consistent with those of earlier USAbased studies; a moderate associations between the use of a gas stove and wheezing was observed only in the univariate analysis. No quantitative measurements of indoor pollutants or allergens were made in NHANES III, and the questions relating to indoor air were narrow in their scope; these are important limitations to the study's findings. The relationship of these findings to housing characteristics and home heating, ventilation and air conditioning should be further explored.
Previously, pet ownership has been linked to asthma and asthma symptoms in children and adults 31 as found in this study. The magnitude of the association with wheezing, however, was diluted and became nonsignificant after simultaneously adjusting for other confounders in the model. One possible reason for this diminished effect could be that subjects with wheezing avoided pets and this observed association has been underestimated. Hay fever is a wellestablished risk factor for asthma and wheezing, and the current findings are consistent with this.
Until recently, few epidemiological studies have looked at the relationship between obesity and asthma. However, positive associations have been found in studies of nurses 32, children 4, and British adults 33, and the results from the present study are similar. Individuals with asthma tend to be overweight 4 and obese individuals tend to have lower pulmonary function tests 34. Due to the crosssectional nature of the study it may be argued that the higher BMI is a result of asthma, due to weight gain from corticosteroid use or avoidance of physical activity. Obese individuals are generally sedentary, which may result in increased time spent indoors, thereby predisposing them to indoor air allergens, environmental tobacco smoke, and dust mite antigens. Obesity also predisposes to gastrooesophageal reflux disease, which may induce asthmatic symptoms 35. Given the current concern regarding obesity as a public health problem in the USA, a more detailed evaluation of this association is definitely warranted.
The major limitation of this analysis is the crosssectional nature, which precludes establishing temporal relationships or inferring causality. Asthma is frequently misdiagnosed, especially among the elderly and very young. With the absence of any objective measure to test airway hyperresponsiveness (e.g. histamine or methacholine challenge tests) the possibility of misclassification cannot be ruled out. However, any such misclassification would likely be nondifferential. In the present study, all subjects with emphysema in the final analysis were removed but those who had responded affirmatively to the question on ever having been diagnosed as having chronic bronchitis (item HAC1F in the NHANES III) were retained. This decision was made because chronic bronchitis is a symptombased diagnosis and although the authors recognise that the main risk factor for “true” chronic bronchitis is cigarette smoking, it is also true that asthma may present with chronic cough as its only symptom (coughvariant asthma). Consequently, there is a certain degree of overlap between the two conditions in adults. Interestingly, when a subgroup analysis was performed on persons who indicated having a diagnosis of chronic bronchitis (but not emphysema) and these respondents were stratified by smoking status, a higher prevalence of current asthma was observed among nonsmokers (22.3%, 95% CI 15.8–28.8), past smokers (24.0%, 95% CI 14.8–33.1), and current smokers (24.7%, 95% CI 17.5–31.8) with chronic bronchitis. This would support the impression that there is some overlap (possibly misclassification) between chronic bronchitis and asthma, but that smoking status does not significantly impact the prevalence of asthma in these persons. However, when the prevalence of wheezing in the previous 12 months was examined in the same subgroup of chronic bronchitis subjects, by smoking status, the breakdown was as follows: nonsmokers (45.4%, 95% CI 36.8–53.9), past smokers (43.7%, 95% CI 33.4–54.0) and current smokers (62.9%, 95% CI 55.8–69.9). Given the disparity between the findings for asthma and wheezing, it is possible that wheezing in current smokers reflects a condition other than asthma (e.g. undiagnosed COPD, or chronic obstructive bronchitis), leading to some misclassification of asthma status.
In summary, this cross sectional analysis of the National Health and Nutrition Examination III dataset showed that race/ethnicity, female sex, socioeconomic status, smoking, obesity, hay fever and pet ownership are important risk factors for asthma and wheezing. Differences in prevalence of asthma and wheeze were observed for USA regions when stratified by race/ethnicity. MexicanAmericans are less likely to report asthma and wheeze irrespective of their socioeconomic and health insurance status. No significant associations were found with a few surrogate measures of indoor air quality.
- Received June 24, 2002.
- Accepted December 5, 2002.
- © ERS Journals Ltd
References









