





Abstract
Within the framework of the APHEA2 (Air Pollution on Health: a European Approach) project, the effects of ambient particles on mortality among persons ≥65 yrs were investigated.
Daily measurements for particles with a 50% cut-off aerodynamic diameter of 10 µm (PM10) and black smoke (BS), as well as the daily number of deaths among persons ≥65 yrs of age, from 29 European cities, have been collected. Data on other pollutants and meteorological variables, to adjust for confounding effects and data on city characteristics, to investigate potential effect modification, were also recorded. For individual city analysis, generalised additive models extending Poisson regression, using a locally weighted regression (LOESS) smoother to control for seasonal effects, were applied. To combine individual city results and explore effect modification, second stage regression models were applied.
The per cent increase (95% confidence intervals), associated with a 10 µg·m−3 increase in PM10, in the elderly daily number of deaths was 0.8% (0.7–0.9%) and the corresponding number for BS was 0.6% (0.5–0.8%). The effect size was modified by the long-term average levels of nitrogen dioxide (higher levels were associated with larger effects), temperature (larger effects were observed in warmer countries), and by the proportion of the elderly in each city (a larger proportion was associated with higher effects).
These results indicate that ambient particles have effects on mortality among the elderly, with relative risks comparable or slightly higher than those observed for total mortality and similar effect modification patterns. The effects among the older persons are of particular importance, since the attributable number of events will be much larger, compared to the number of deaths among the younger population.
The APHEA (Air Pollution on Health: a European Approach) project 1–3 started as an attempt to provide quantitative estimates of the short-term health effects of air pollution, using an extensive database from 10 different European countries (15 cities with >25 million people), through time series data and meta-analysis.
Daily measurements of black smoke (BS), sulphur dioxide (SO2), suspended particles (as total or particles with an aerodynamic diameter smaller than a certain cut off), nitrogen dioxide (NO2) and ozone (O3) were derived from existing monitoring networks. The outcome data were daily counts of total and cause-specific deaths and hospital emergency admissions. Data on potential confounders (e.g. seasonal and long term patterns, meteorological factors, day of the week, holidays, influenza epidemics, unusual events such as strikes of medical staff) were also used.
Poisson regression allowing for autocorrelation and over-dispersion was used in the analysis, controlling for all potential confounding factors, choosing the “best” air pollution models, and applying diagnostic tools to check the adequacy of the models.
The results of APHEA were firstly reported in a series of articles describing the individual contributions to the collaborative effort: Bratislava, Slovak Republic 4; Amsterdam and Rotterdam, the Netherlands 5; Lyon, France 6; Cracow, Lodz, Poznan, and Wroclaw, Poland 7; Paris, France 8; Athens, Greece 9; Koln, Germany 10; Helsinki, Finland 11; Milan, Italy 12.
Subsequently, the APHEA results were reported in a series of articles describing the pooled findings of the health outcomes for a 50 µg·m−3 increase in daily mean level of a single pollutant.
Anderson et al. 13 found increased probabilities of hospital admissions for chronic obstructive pulmonary disease (COPD) ranging 2–4%; Katsouyanni et al. 14, investigated particles and SO2, and found increases in daily mortality ranging 2–3% in Western European cities and from 0.6–0.8% in Central Eastern European cities (with stronger effects during the summer); Touloumi et al. 15, who investigated NO2 and O3, found a 1.3–2.9% increase of daily number of deaths, respectively; Sunyer et al. 16 described daily admissions for asthma that increased as follows: significantly by 2.9% with increasing ambient levels of NO2, nonsignificantly by 2.1% with BS in adults (15–64 yr); significantly by 7.5% with SO2 and by 8% in cold seasons with NO2, and nonsignificantly by 3% with BS in children <15 yrs.
Spix et al. 17, from the quantitative pooling of local analyses on five West European cities, found a significant increase of daily admissions for respiratory diseases (adults of 15–64 yrs and elderly of ≥65 yrs) with elevated levels of O3. This finding was stronger in the elderly, had a rather immediate effect, and was homogeneous over cities. The elderly were affected more during the warm season. The effect of BS was significantly stronger with high NO2 levels on the same day. O3 results were in good agreement with the results of similar USA studies.
Zmirou et al. 18, from a meta-analysis on 10 large European cities, found that daily deaths from cardiovascular conditions increased 2% with BS, 2% with O3 and 4% with SO2; the analogous figures for respiratory diseases were 4, 6 and 5%, respectively. This occurred in Western but not in Central European cities.
Some papers 19–21 summarised and commented on the APHEA findings and considered the theoretical and practical aspects of a monitoring system and made recommendations concerning the minimum data-set required, the methods of statistical analysis and presentation, and Europe-wide coordination of monitoring.
One intriguing finding was that the effects were lower in Central-Eastern European cities. Samoli et al. 22 reanalysed through generalised additive models the original data by restricting to days with pollutant concentration <150 µg·m−3. The new estimates for increase in mortality, only in Central-Eastern European cities, were larger than the ones published previously: by 69% for BS and 55% for SO2. Thus, part of the heterogeneity in the estimates of air pollution effects had been caused by the statistical approach and lack of threshold for pollutant levels.
Overall, through the APHEA study, the existence of an association between daily variations in the levels of urban air pollution and adverse health effects was confirmed in Europe. This association is weak, but it involves the whole resident population, so it is a major cause of concern from the public health point of view.
APHEA methodology has been discussed and utilised by other investigators, as well 23–33.
The APHEA (Air Pollution on Health: a European Approach) project
During the last decade consistent results from several epidemiological studies have indicated that current concentrations of ambient particulate matter (PM) have adverse health effects including increases in daily mortality 34, 14. Important evidence was added to these results by multicentre studies such as the APHEA project in Europe 1–22 and the National Mortality Morbidity and Air Pollution Study (NMMAPS) in the USA 35, which included data from several cities collected and analysed using a standardised protocol. The above results influenced the revisions of air quality standards in the USA and in Europe 36, 37.
Recently, attention has shifted to understanding, among other issues, which particular population groups are more sensitive to these effects 38. The elderly, which are proportionally increasing in Europe, are a group of special interest.
The APHEA2 project was implemented, as a continuation of the APHEA project, based on a more extended database, with objectives to address the consistency of associations, to identify sensitive subpopulations and specific particle characteristics, and to explore confounding and effect modification 39, 40.
The estimated increase in the daily number of deaths for all ages for a 10 µg·m−3 increase in daily particles with a 50% cut-off aerodynamic diameter of 10 µm (PM10) or BS concentrations was 0.6%, whereas for the elderly it was slightly higher 39. There were important effect modifications for several variables: e.g. in a city with low versus one with high average NO2, the estimated increase was 0.19 versus 0.80%; in a relatively cold versus one with warm climate 0.29 versus 0.82%; in a city with low versus one with high standardised mortality rate 0.80 versus 0.43%. For the same pollutants increase, Atkinson et al. 40 found increase in daily hospital admission for: asthma (0–14 yrs) of 1.2%, asthma (15–64 yrs) of 1.1%, and COPD plus asthma and all-respiratory (≥65 yrs) of 1.0 and 0.9%. In the ≥65 groups PM10 estimates were positively associated with annual mean concentrations of O3. Zanobetti et al. 41 analysed the mortality displacement issue, i.e. if it is due solely to the deaths of frail individuals, which are brought forward by only a brief period of time. They fit a Poisson regression model and a polynomial distributed lag model with up to 40 days of delay in each city. They found that the overall effect of PM10 per 10 µg·m−3 for the fourth-degree distributed lag model is a 1.61% increase in daily deaths (95% confidence interval (CI): 1.02–2.20), whereas the mean of PM10 on the same day and the previous day is associated with only a 0.70% increase in deaths (95% CI: 0.43–0.97). Thus, the effect size estimate for airborne particles more than doubles when longer-term effects are considered, which has important implications for risk assessment.
This paper reports the results of the APHEA2 project on the effects of daily PM on mortality among persons ≥65 yrs, in 28 European cities.
Data and methods
Data was collected from 28 cities across Europe: Athens, Barcelona, Basel, Bilbao, Birmingham, Budapest, Cracow, Dublin, Geneva, Helsinki, Ljubljana, Lodz, London, Lyon, Madrid, Marseille, Milano, Paris, Poznan, Prague, Rome, Stockholm, Tel-Aviv, Teplice, Torino, Valencia, Wroclaw, Zurich with a total population exceeding 43 million. The study period was ∼5 yrs for most cities, within the nineties. The health outcome in the present analysis was the daily number of deaths (excluding deaths from external causes, International Classification of Diseases (ICD)9 ≥800) among persons ≥65-yrs-old, which ranged, in the different cities, from 4–139 on average per day. PM10 concentrations were contributed for the whole or part of the period (or could be estimated based on other studies) from 21 cities: the 24 hr concentrations ranged from 15 µg·m−3 to 66 µg·m−3 on average. Fourteen cities contributed daily BS measurements; these ranged 10–64 µg·m−3 (24 h concentrations). Measurements of air pollutants were provided by monitoring networks established in each town. The selection criteria for monitors to be included in the study (based on completeness of measurements) and the methods for replacing the few remaining missing values are described elsewhere 39. Data was also collected on potential confounders: other pollutants (specifically SO2, NO2, O3, carbon monoxide), meteorological variables (daily temperature and relative humidity), influenza epidemics. Day of the week, national and school holidays, seasonality and long-term trends were also adjusted for. Since significant heterogeneity between individual city estimates had been observed before 14, the present authors collected information on potential effect modifiers characterising the city with respect to the pollutant mix, the status of health of the population, climate and geography 39.
A two-stage analysis was applied. In the first stage, city-specific regression models were fitted and their results were used in a second stage analysis to provide overall estimates and to investigate effect modification. Days with PM10 or BS levels >150 µg·m−3 were excluded. These days did not exceed 5% of the total number of days. Generalised additive models, extending Poisson regression were applied allowing for overdispersion. Local nonparametric locally weighted regression (LOESS) smoothers were used to control for seasonal patterns and long-term trends. Temperature, humidity, day of the week, holidays, unusual events and influenza epidemics were also appropriately controlled for 39. For PM10 and BS, the average concentrations of lags 0 and 1 was a priori chosen as exposure measure. For the second stage analysis, i.e. the combination of results across cities, meta-regression models were used. These allowed the estimation of combined effects and the investigation of the role of potential effect modifiers in explaining observed heterogeneity. Fixed and random effects models were used as appropriate. More details on the data and methods have been reported elsewhere 39.
Results
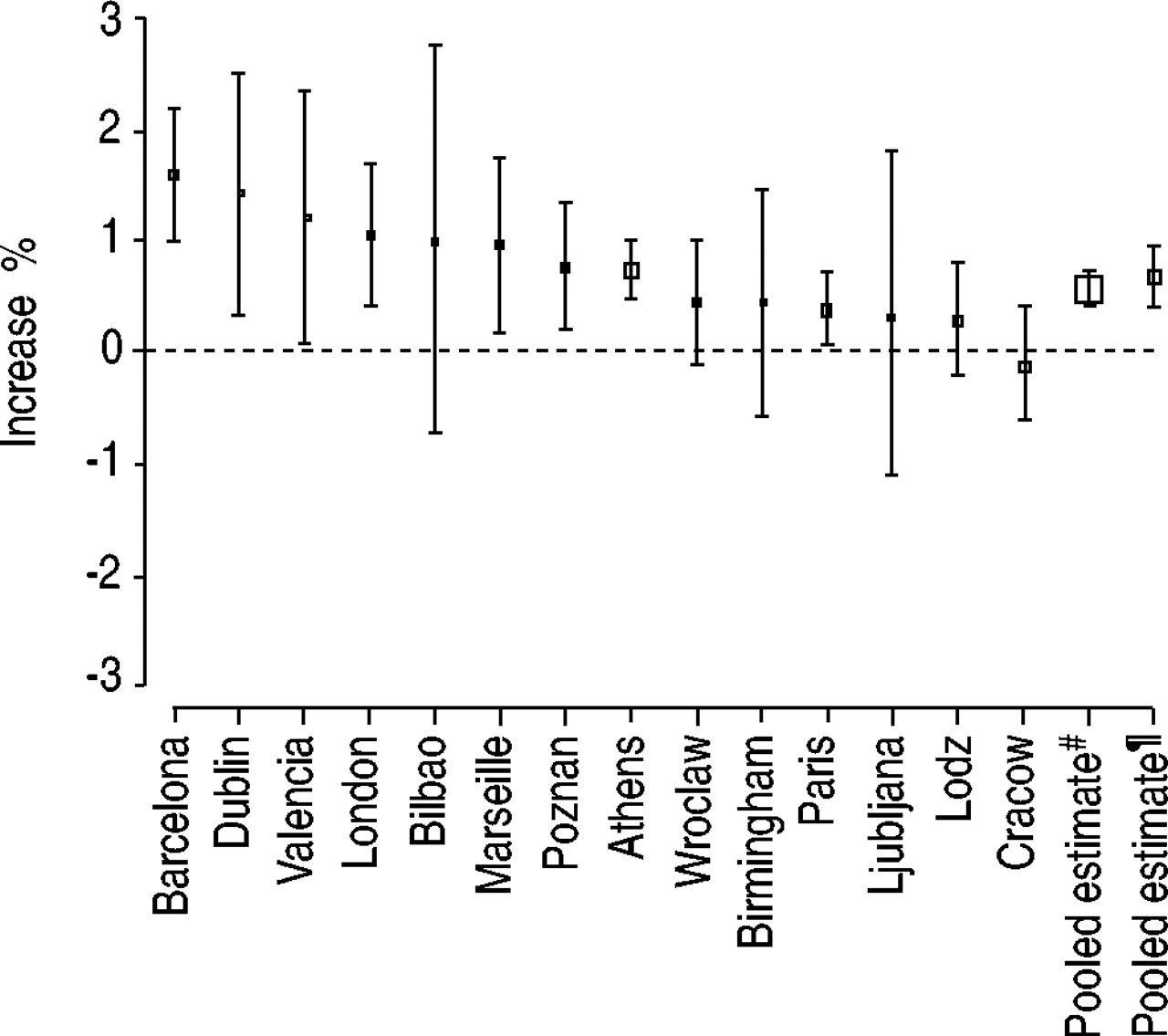
In figure 1⇓ the individual city as well as the pooled effect estimates for the daily number of deaths among the elderly, associated with a PM10 increase of 10 µg·m−3 are shown. The individual city effect estimates are positive for all cities except one. They range from an increase in the daily number of deaths of 0–1.7%, associated with 10 µg·m−3 increase in daily PM10 concentrations. In figure 2⇓ the corresponding effect estimates for a similar increase in BS are shown. BS effects in individual cities range from 0–1.6% increase in the daily number of deaths associated with a daily increase of 10 µg·m−3 in BS concentrations. In table 1⇓ the pooled estimated effect from fixed and random effects models for the elderly and those for all ages (for comparison) are shown. It should be noted that published estimates for all ages mortality included one more city, Erfurt in Germany, in which the daily number of deaths for the elderly was not available 39. For reasons of comparability, the present authors calculated here the combined estimates without Erfurt. The pooled effects remain practically the same since Erfurt had little weight in the combined analysis, due to its small population. The effect estimates for the elderly are consistently higher compared to those for all ages. In tables 2 and 3⇓⇓ the results on effect modification are shown for PM10 and BS estimates respectively. Only effect modifiers which are statistically significant (p<0.05) and explain >10% of the heterogeneity are presented. To illustrate the magnitude of the effect modification, the effect estimated for a city with “low” level in the effect modifier (i.e. at the 25th percentile of the corresponding effect modifying variable distribution) and that estimated for a city with “high” level in the effect modifier (i.e. at the 75th percentile of its distribution) are presented. Thus, it can be seen that, for the most important effect modifier identified, long term NO2 concentration, the effect of PM10 on the daily number of deaths among the elderly, ranges from 0.30% in cities with low long-term average NO2 (about 40 µg·m−3) to 0.97% in cities with high long-term average NO2 (about 70 µg·m−3). Other important effect modifying variables are the temperature and relative humidity levels (PM10 effects are higher in warmer and drier cities), the age-standardised annual mortality rate (higher mortality is associated with lower PM10 effects), the proportion of the elderly (a higher proportion of elderly is associated with higher PM10 effects) and geographical region (effects are highest in Southern and lowest in the Central-Eastern cities). It should be noted that these effect modifying variables were included in the models alternatively and the effects reported may be partly due to their intercorrelations. The effect modification pattern for BS effects is similar to that for PM10. When three effect modifiers were included in one model (the most important ones from each category, i.e. NO2, temperature and age-standardised mortality rate or the proportion of the elderly) the p-value for the remaining heterogeneity was >0.20.

Estimated per cent increase and 95% confidence intervals in the daily number of deaths of persons ≥65-yrs-old associated with an increase of 10 µg·m−3 in the levels of particles with a 50% cut-off aerodynamic diameter of 10 µm (PM10) for individual cities and overall. The size of the data point is inversely proportional to its variance. #: fixed effect; ¶: random effect.
{kind=link}
{kind=link}
Estimated per cent increase and 95% confidence intervals in the daily number of deaths of persons ≥65-yrs-old associated with an increase of 10 µg·m−3 in the levels of black smoke for individual cities and overall. The size of the data point is inversely proportional to its variance. #: fixed effect; ¶: random effect.
Pooled estimates for the increase in the total daily number of deaths and deaths among the elderly associated with a 10 µg·m−3 increase in particles with a 50% cut-off aerodynamic diameter of 10 µm (PM10) and black smoke (BS) (average concentrations of lags 0 and 1)
Results of the second stage regression models investigating the role of potential effect modifiers# of the estimated effects of particles with a 50% cut-off aerodynamic diameter of 10 µm (PM10) on the daily number of natural deaths among persons ≥65 yrs old
Results of the second stage regression models investigating the role of potential effect modifiers# of the estimated effects of black smoke (BS) on the daily number of natural deaths among persons ≥65 yrs old
Discussion
The present study estimated the effect of daily ambient particulate matter concentrations on the number of deaths among the elderly (persons ≥65-yrs-old) in 28 European cities, using the database compiled within the APHEA2 project 39. The effect estimates were consistently larger, by 10–20%, than those estimated for all age mortality from an identical database. The effects of two different ambient particle measures, PM10 and BS, were comparable.
In the studied cities elderly mortality comprised 67–88% of the total number of deaths, thus playing a predominant role in determining the magnitude of all age mortality. In other studies in which the effect of particles on mortality has been investigated, the age distribution of those who died on any given day was different. Thus, in a study in Sao Paolo, Brazil 42, the percentage of deaths among those >65 yrs was only 49%. In that study, the effect of a daily change of 10 µg·m−3 in PM10 on the daily number of deaths from all causes among the elderly was found to be a 0.5% increase, which is comparable to the one reported from the present analysis, but slightly smaller. The difference in size may be due to the use of a one day PM measurement in the Brazilian study, whilst in APHEA2 the average of lags 0 and 1 was used. It has been shown that longer time averages result in higher estimates 43. This difference may also be attributable to a higher mean age of death in the APHEA2 populations compared to Sao Paolo. If older age groups are consistently at higher risk of death from air pollution, then it will be expected that, in a population where the mean age is higher, larger PM effects will be observed. In studies conducted in places where the age-distribution of the population is similar to that in Europe, the results were close to those reported here. Thus, in a study in Canada 44 the increase in mortality among the elderly associated with a 10 µg·m−3 increase in PM10 was found to be 0.69% for lag0 and 0.79% for lag1 whilst that for all ages was 0.67% for lag0 and 0.36% for lag1. In the USA NMMAPS 35 the increase in the daily number of deaths for all ages associated with a 10 µg·m−3 change in PM10 was 0.5%.
The city specific estimates in the current study were heterogeneous, as were those reported before for all age total and cause-specific mortality 14, 18, 39. One objective of the APHEA2 project was to investigate the reasons for this heterogeneity. In this analysis important effect modifiers have been identified. They are generally consistent to those reported for the all age mortality 39. Thus, higher long-term average NO2 concentrations are associated with larger PM effects. Since NO2 is mainly an indicator of pollution originating from traffic and it is likely that in locations with high NO2 there will be more traffic-related particles, this result may be considered as an indication that these particles are more harmful to human health. Higher PM effects are found in warmer and drier climates. This finding may be due to a higher exposure to outdoor air pollution of populations living in milder climates and should be further investigated using additional data on time-activity patterns, housing and ventilation conditions. It is also found that in cities with higher age-standardised mortality rate, PM effects on the elderly are smaller, in relative terms. This may be a result of competing risks and the health status of the population and is consistent with the results published by Gouveia and Fletcher 42. It is expected that in populations with higher underlying mortality rate the proportional increase in the outcome due to air pollution exposure will be smaller 39, 42.
An interesting finding in the present context, is that the proportion of the elderly appears as modifying the PM effect on elderly mortality. This implies that the PM effect is not constant across different age subgroups among those ≥65 yrs. The average PM effect in an elderly population, thus, probably depends on the mean age of this population. It is plausible to expect that in cities with a larger proportion of elderly, the population group of those ≥65 will also have a higher mean age. In this case, if PM effects increase with age, then higher mean age would result in larger effect estimates. The present authors' result and that reported by Gouveia and Fletcher 42 are in line with this hypothesis.
Acknowledgments
The APHEA2 project was supported by the EC Environment and Climate 1994–98 project, Contract number ENV4-CT97-0534. The Swedish and Teplice groups did not receive E.C. funding.
The Air Pollution and Health: a European Approach (APHEA2) collaborative group consists of: K. Katsouyanni, G. Touloumi, E. Samoli, A. Gryparis, Y. Monopolis, E. Aga, D. Panagiotakos (Greece, Coordinating centre); C. Spix, A. Zanobetti, H.E. Wichmann (Germany); HR Anderson, R. Atkinson, J. Ayres (UK); S. Medina, A. Le Tertre, P. Quenel, L. Pascale, A. Boumghar (Paris, France); J. Sunyer, M. Saez, F. Ballester, S. Perez-Hoyos, J.M. Tenias, E. Alonso, K. Kambra, E. Aranguez, A. Gandarillas, I. Galan, J.M. Ordonez (Spain); M.A. Vigotti, G. Rossi, E. Cadum, G. Costa, L. Albano, D. Mirabelli, P. Natale, L. Bisanti, A. Bellini, M. Baccini, A. Biggeri, P. Michelozzi, V. Fano, A. Barca, F. Forastiere (Italy); D. Zmirou, F. Balducci (Grenoble, France); J. Schouten, J. Vonk (the Netherlands); J. Pekkanen, P. Tittanen (Finland); L. Clancy, P. Goodman (Ireland); A. Goren, R. Braunstein (Israel); C. Schindler (Switzerland); B. Wojtyniak, D. Rabczenko, K. Szafraniec (Poland); B. Kriz, A.M. Celko, J. Danova (Prague, Czech Republic); A. Paldy, J. Bobvos, A. Vamos, G. Nador, I. Vincze, P. Rudnai, A. Pinter (Hungary); E. Niciu, V. Frunza, V. Bunda, (Romania); M. Macarol-Hitti, P. Otorepec (Slovenia); Z. Dörtbudak, F. Erkan (Turkey); B. Forsberg, B. Segerstedt, (Sweden); F. Kotesovec, J. Skorkovski (Teplice, Czech Republic); M. Pavlovic, D. Simic (Croatia).
- Received April 12, 2002.
- © ERS Journals Ltd
References









