





Abstract
People spend about ≥80–90% of their daily time indoors, elderly people especially at home. Thus, it is important to investigate possible health effects of indoor air pollutants and to consider their contributions to the total human exposure.
This report summarises current knowledge on health effects of three common indoor air pollutants, respirable suspended particles, nitrogen dioxide and environmental tobacco smoke, with focus on the adults and the elderly. Preliminary findings on exposure distributions and health effects of these pollutants in older subjects of two panel studies carried out in Italian general populations will also be reported.
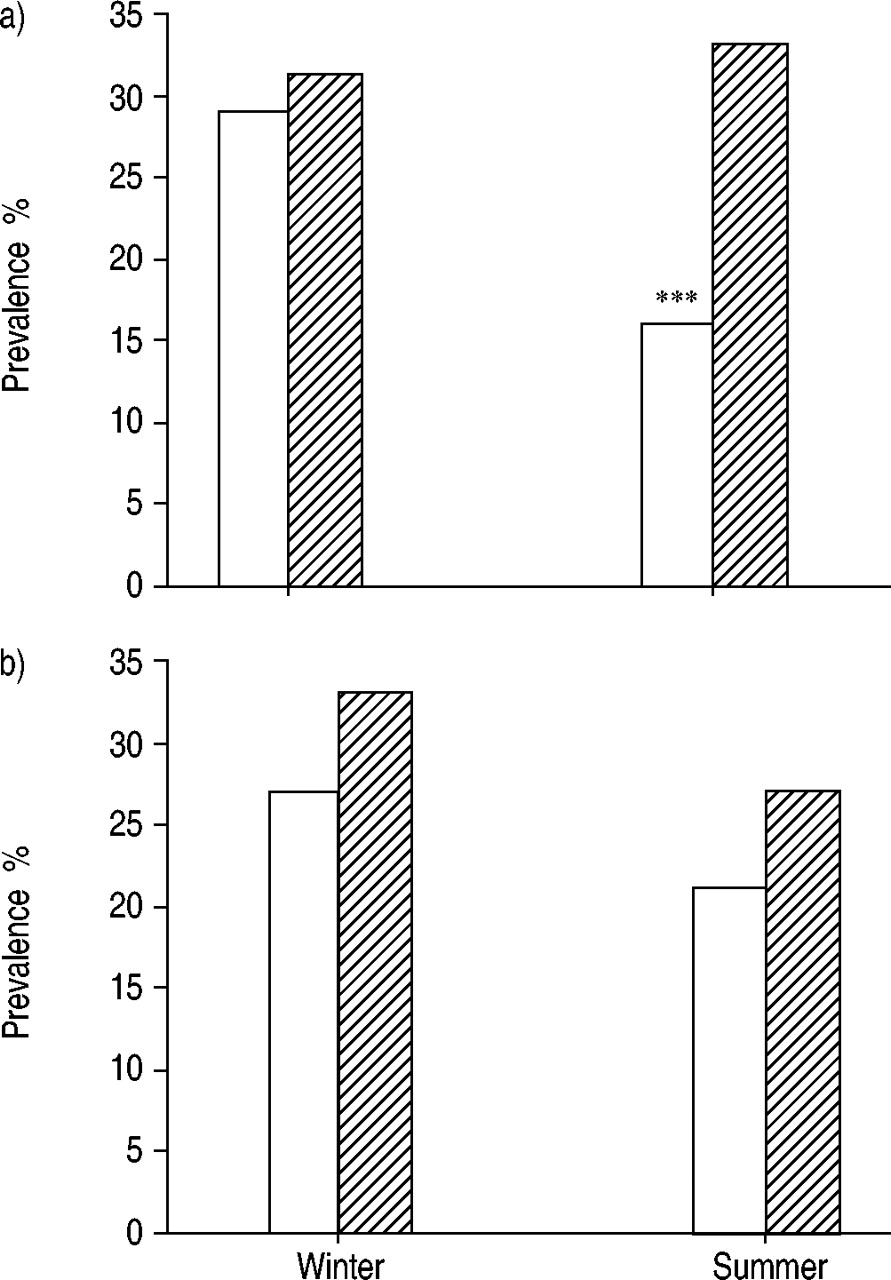
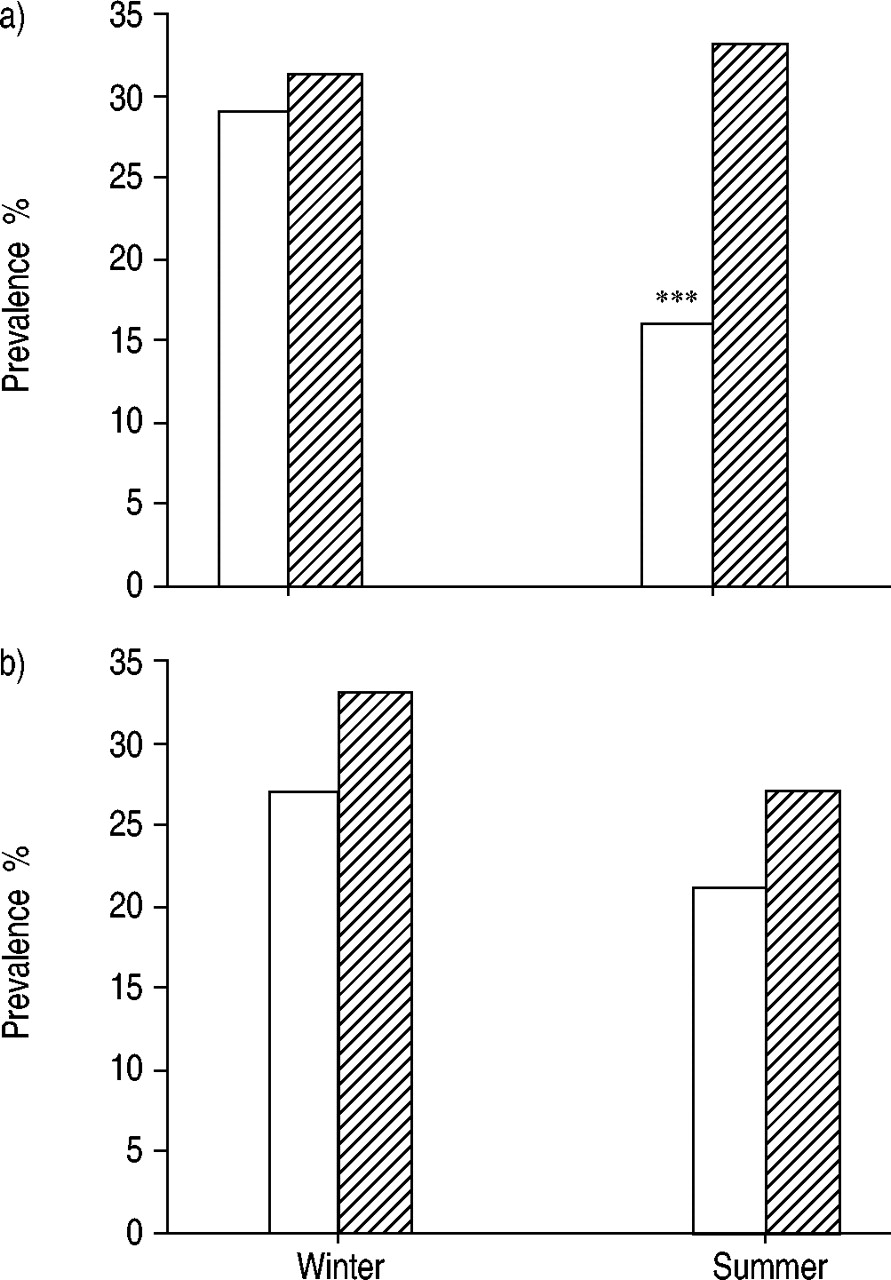
The two indoor pollution studies were performed in the Po Delta area in North Italy (428 subjects and 140 houses investigated) and in Pisa in Central Italy (761 subjects and 282 houses investigated). Individuals aged ≥65 yrs spent a significantly larger number of hours at home than the other age groups both in winter and in summer. A trend of higher occurrence of acute respiratory symptoms in the presence of environmental tobacco smoke was shown in comparison to the unexposed elderly both in winter (31 versus 29%) and summer (33 versus 16%). The occurrence of acute respiratory symptoms was consistently higher in relation to the high respirable suspended particles-index exposure compared to low exposure (33 versus 27% in winter, 27 versus 21% in summer). Both the presence of environmental tobacco smoke at home and exposure to the high respirable suspended particles-index were associated with a decrease in the mean daily peak expiratory flow.
Indoor air pollution is a major global public health problem requiring increasing efforts in research and policy-making 1. The concentrations of several pollutants can be many times higher indoors than outdoors 2. In addition, the presence of indoor pollutants, even at low concentrations, may have important biological impact because of long exposure periods. People spend ≥80–90% of their day indoors, and elderly people are likely to spend even more time at home 2, 3. Thus, indoor air pollutants may have special significance for this age group. Since the length of life expectancy is increasing in all developed countries, more efforts to study the effects of air pollution on the health of the elderly are needed, including studies on indoor air quality. Several studies have investigated the effects of indoor air pollution on health of infants and children 1, 4–10. Some studies have shown evidence that indoor air pollution increases the risk of respiratory and atopic diseases even in adult populations 11–14, but information on health effects of such pollutants in the elderly is sparse.
The aim of this report is to summarise current knowledge on health effects of three common indoor air pollutants, namely respirable suspended particles (RSP), nitrogen dioxide (NO2), and environmental tobacco smoke (ETS), focusing on the adults and the elderly. In addition, the home exposure distributions and health effects of these pollutants in older subjects in two Italian studies carried out in general adult populations will be presented 3, 15. Finally, methodological issues and questions for future research will be discussed.
Health effects of respirable suspended particles, nitrogen dioxide and environmental tobacco smoke
Suspended particulate matter, which is produced by ETS, cooking, cleaning and renovation activities, unvented gas and kerosene heaters indoors, and by penetration from outdoors, is a common measurable indoor pollutant. Particles >10 µm are usually removed at the upper airways, whereas those <10 µm (i.e. RSP) may be deposited in the smaller airways and alveoli 16. Recently, several studies have found strong associations between outdoor RSP levels and mortality and morbidity, especially in the elderly 17–18. Some studies 19–20 have indicated a strong correlation between indoor and outdoor particulate matter (PM) concentrations, suggesting that outdoor concentrations may be considered as a proxy for indoor concentrations. On the other hand, other studies 21, 22 utilising personal monitoring have found only a small correlation between total personal PM exposure and outdoor concentrations, suggesting that indoor concentrations provide a major contribution to the total exposure and, thus, to the health effects.
Only a few studies have evaluated the effects of indoor RSP on respiratory health in adults (table 1⇓) 14, 23, 24. The study on indoor pollutants in the Po Delta area in North Italy 23 showed an association of relatively low levels of RSP with increased occurrence of acute respiratory symptoms. There was a significant positive association between RSP exposure and bronchitic and asthmatic symptoms in winter. In nonsmokers, a similar association was observed also in summer. Moreover, the symptom duration was greater in the presence of high RSP exposure. With regard to peak expiratory flow (PEF) and its variability, an increase in RSP exposure was associated with an increase in both max amplitude and diurnal variation of PEF. A study on the effects of indoor particulate levels on respiratory health in Chinese neversmokers, aged 40–69 yrs, showed an association between increasing level of particulates and the risk of chronic respiratory symptoms 14. Consistently with these results, a trend of increasing risks for respiratory symptoms with increasing indoor particles with a 50% cut-off aerodynamic diameter of 10 µm (PM10) levels was shown in a more recent study on Chinese adults 24.
Effects of indoor particulate matter level/coal smoke on respiratory health in selected earlier studies on adults
Another common and easily measurable indoor pollutant is NO2 produced by unvented gas cooking, kerosene and propane space heaters, ETS, and wood heating indoors, and by penetration from outdoors. NO2 has been shown to cause lung damage at high concentrations 25. NO2 may penetrate the conducting airways also at moderate levels and produce respiratory symptoms and irritative symptoms of the nose and eyes 25.
Few studies on the relationship between indoor NO2 and health in adults or the elderly have been reported (table 2⇓) 25, 26–28. The Po Delta study 23 showed an association of relatively low levels of indoor NO2 with increased occurrence of acute respiratory symptoms and reduced PEF in adults. Bronchitic and asthmatic symptoms were significantly more prevalent in the presence of high NO2 exposure. High NO2 exposure was associated with greater symptom duration. Increase in NO2 exposure was also associated with an increase in both max amplitude and diurnal variation of PEF, the associations being significant only in subjects with chronic respiratory diseases (i.e. asthma and bronchitis).
Indoor nitrogen dioxide (NO2) levels and lung function and respiratory symptoms/diseases in selected studies of adults
A study of British adults 26 showed a significantly reduced forced expiratory volume in one second (FEV1) in subjects who currently used gas for cooking compared to those who used electricity. In an Australian study 27 the presence of gas heaters at home was significantly associated with increased prevalence of asthma in males. Gas cooking was also associated with increased risk of respiratory symptoms and impaired lung function in nonsmoking women in Singapore 28.
ETS is a common indoor exposure in many countries and it is a major contributor to indoor RSP concentrations. It constitutes >4000 compounds, many of them known carcinogens and irritants 8, 29. Issues on ETS exposure assessment have been discussed before 30–31. The research on health effects of ETS has expanded since the 1980's, focusing on children and lung cancer in adults 8. Table 3⇓ summarises the aetiological studies of ETS and respiratory health in the elderly 32. It also presents a judgment on causality of the relationships, based on the amount of studies, their validity, evidence of dose-response relationships, and biological plausibility.
Summary of aetiological studies on environmental tobacco smoke and respiratory diseases and conditions in the elderly 32
There is convincing evidence that ETS causes lung cancer and coronary heart disease, both of which are diseases of the elderly 8, 32–35. Several cross-sectional studies have shown increased occurrence of chronic respiratory symptoms and deficits in ventilatory lung function in relation to ETS exposure at home and/or at work 8, 13, 28, 32, 36–40. A limited number of studies have investigated the relationship between ETS exposure and asthma, chronic obstructive pulmonary disease (COPD) and pneumococcal infections in the elderly, but all of them indicate an increased risk among those exposed to ETS 13, 32, 41–44.
More longitudinal studies are needed on ETS and respiratory diseases among the elderly, since even small changes in respiratory function may have a critical impact on the quality of life of the elderly. Moreover, it is important to assess the effects of ETS exposure on elderly people with a pre-existing disease that may restrict them to indoor environments with possible very high levels of ETS exposure 32. Surprisingly few studies 32, 44–48 have evaluated the role of ETS in determining the prognosis of an established disease, such as asthma or COPD, although this may be critical for the ability of the elderly to function in everyday life 32.
Methods of indoor surveys
To investigate the exposure distributions and respiratory effects of NO2, RSP, and ETS, two panel studies were performed in 1991–1994 in subsamples of two randomised stratified samples of Italian general populations, studied previously in cross-sectional surveys 11, 12, 49.
Subsamples were selected to include subjects fulfilling the following criteria: 1) subjects with current asthma and/or asthmatic symptoms; 2) subjects with bronchial hyper-reactivity (defined as provocative dose causing a 10% fall in FEV1 (PD10)<2.4 mg in methacholine challenge); 3) current smokers without asthmatic symptoms or bronchial hyper-reactivity; 4) “healthy” subjects, who were neither active or passive smokers nor had asthmatic symptoms or bronchial hyper-reactivity; 5) some other subjects not included in the previous groups 23, 50. One study took place in the Po Delta area in Northern Italy (n=428, 140 houses investigated) 3 and the other in Pisa in Central Italy (n=761, 282 houses investigated) 15.
Information on home characteristics and smoking and other habits of the family were inquired with a modified version of the new EPA standardised environmental inventory questionnaire 3.
Study subjects filled in a daily diary on daily activity pattern (the number of hours spent at home, cooking or doing other activities, the number of hours spent at work or in the school, in other indoor locations, in transit, and outdoors) and on the occurrence of acute respiratory symptoms (allergic symptoms and acute respiratory illnesses and irritative symptoms) during the study weeks. The following were considered acute symptoms: runny nose, sore throat, sputum production from the chest, chest cold, shortness of breath, attack of shortness of breath, wheeze, and red, itchy, watery or burning eyes. Occurrence of chronic symptoms and diseases, such as asthma and bronchitis, were inquired in the previous cross-sectional studies 11, 12. To assess lung function, each subject performed PEF measurements four times daily using a mini-Wright peak flow meter.
To assess exposure, each house was monitored for 1 week in winter and 1 week in summer to measure RSP (i.e. particles with an aerodynamic diameter <2.5 µm, in µg·m−3) and NO2 (in parts per billion (ppb)). RSP sampling was performed by active sampling (two 48 h samples) using a Dorr Oliver-type preselector 3. The mean of the two 48‐h values during the study week was used in the analyses. NO2 sampling was carried out with passive samplers (Palmes tubes) during each week and analysed with spectrophotometric techniques (Saltzman reaction) 3. Indices of exposure to NO2 (NO2-IndEx) and to RSP (RSP-IndEx) were computed as the product of the weekly mean concentration and the daily duration of exposure (i.e. the time spent at home). The indices were considered “low” or “high” based on values below or above the median value.
The Chi-squared test was used to test the differences in occurrence of respiratory symptoms between the exposure groups and nonparametric Mann-Whitney U‐test for comparing exposure and time distributions. Multiple linear regression analysis, adjusting for the season, sex, height and weight, was applied to study the relationship between exposures and the mean daily PEF levels. A p‐value <0.05 was considered as statistically significant. Analyses on the effects of indoor pollutants on respiratory symptoms in the elderly were performed on subjects ≥65 yrs (n=59 and 61 in winter and summer, respectively).
Results
Subjects living in the Po Delta and Pisa areas spent most of their day indoors. Older subjects spent a significantly (p<0.001) higher number of hours at home daily compared to subjects of the other age groups (table 4⇓). Home concentrations of NO2 and RSP were significantly higher in winter than in summer (21 versus 15 ppb for NO2; 77 versus 49 mg·m−3 for RSP). The highest values of NO2 were found in the kitchens (33 and 20 ppb in winter and summer, respectively).
Daily activity pattern (in hours) by age group in winter and in summer in the Po Delta and Pisa areas
Analyses in older subjects (≥65 yrs) of the Po Delta 3, 23 and Pisa 15 showed a trend of higher occurrence of acute respiratory symptoms in relation to ETS exposure both in winter (31% in ETS exposed versus 29% in unexposed) and in summer (33% versus 16%, p<0.001) (fig. 1⇓). The occurrence of acute respiratory symptoms was consistently higher in relation to high RSP exposure compared to low exposure (33 versus 27% in winter, 27 versus 21% in summer), although the differences were not statistically significant (fig. 1⇓). Presence of ETS at home was associated with a decrease in the mean daily PEF (effect estimate: −19.2 L·min−1, p<0.01). In these analyses, NO2 exposure did not affect the occurrence of acute respiratory symptoms or lung function.
{kind=link}
Discussion
People have been shown to spend ∼80–90% of their day indoors, and this percentage increases in the elderly. The Po Delta and Pisa studies confirmed that people ≥65 yrs spend a significantly larger number of hours at home compared to people of the younger age groups. This finding underlines the importance of indoor air quality studies in the elderly, who may be especially susceptible to effects of low concentrations of pollutants because of underlying chronic diseases. It also confirms that, in epidemiological studies, it is important to assess exposures from outdoor and indoor sources separately, as suggested by the U.S. Environmental Protection Agency 29.
Health effects of indoor air pollutants have been addressed in studies of infants and children 1, 4–10, but only a few studies have investigated such effects in adults and in older people 14, 23, 24, 26–28. Previous results of the Po Delta study 23 showed an association of relatively low levels of indoor pollutants (e.g. RSP 77 µg·m−3 in winter and 49 µg·m−3 in summer, NO2 21 ppb in winter and 15 ppb in summer) with acute respiratory symptoms and reduced PEF in adults. The results in older subjects living in the Po Delta and Pisa areas showed consistently higher occurrence of acute respiratory symptoms in relation to high RSP exposure as compared to low exposure. In addition, the high RSP-index was significantly associated with a decrease in the mean daily PEF. This finding is consistent with the negative association between RSP and PEF found in earlier studies of indoor 14 and outdoor 51 pollutants.
The present authors' finding of a trend of increased acute respiratory symptoms in relation to ETS exposure is in accordance with an earlier study of acute symptoms in nurses 37 and with several studies on ETS and chronic respiratory symptoms in adults 8, 13, 28, 32, 36, 38. ETS exposure was also significantly associated with a decrease in the mean daily PEF, which points out that there are small effects of ETS on lung function impairment (table 3⇑) 8, 32, 39.
There is a clear need for more studies on indoor pollution and health in adults, and especially in the elderly. Further development of exposure assessment methodology is a major challenge for the future. Future studies should address both short-term and long-term health effects related to indoor air pollutants. Identification of subgroups among the elderly who are susceptible to the adverse effects of air pollutants would also be an important step to support preventive measures. Few studies have evaluated the role of indoor pollutants in determining the prognosis of pre-existing diseases. Such studies may become an important new area for research, especially among the elderly, who often have chronic diseases restricting them to indoor environments with possible high levels of exposure to indoor pollutants.
In conclusion, the current results in people of ≥65 yrs confirm that older people spend more time at home than younger subjects, emphasising the importance of good indoor air quality for the maintenance of the health of the elderly. In older people, exposure to RSP and ETS is related to increased occurrence of acute respiratory symptoms and reduced lung function.
There is a clear need for more studies on indoor pollutants and health in the elderly, with focus on improved exposure assessment, various types of short-term and long-term health outcomes, and identification of characteristics associated with susceptibility to the adverse effects.
The potential role of indoor pollutants as a prognostic factor determining the development of a pre-existing disease may be an important new area for research.
- Received April 12, 2002.
- © ERS Journals Ltd
References









