





Abstract
Peripheral muscle weakness is common in chronic obstructive pulmonary disease (COPD) but it is still under debate whether weakness is due to atrophy or contractile dysfunction.
In vitro and in vivo contractile properties of the vastus lateralis muscle were studied in 16 patients with stable COPD (forced expiratory volume in one second 39±16% of predicted, age 67±4 yrs (mean±sd)) and nine sedentary control subjects. Isometric knee extensor strength was measured while mid-thigh muscle cross-sectional area (MTMCSA) was obtained using computed tomography. Muscle strips from the vastus lateralis obtained through open biopsy were rapidly suspended in an oxygenated Krebs-Ringer solution that was maintained at 35°C with a pH of 7.40 to study their contractile properties.
The isometric knee extensors strength/MTMCSA ratio was 0.50±0.08 versus 0.58±0.06 kg·cm−2 for COPD and control subjects, respectively. The muscle bundle cross-sectional area (CSA) was 4.6±2.1 and 4.4±3.1 mm−2, the length at which active tension was maximum was 15±4 and 15±3 mm, and maximal isometric peak forces normalised for CSA were 4.3±2.7 and 4.8±2.6 N·cm−2 for COPD and control subjects, respectively. The force/frequency relationship tended to be shifted to the right in patients with COPD, meaning that a higher stimulation frequency was necessary to produce the same relative force. Patients with COPD had a lower proportion of type I fibre than controls (26±12% versus 39±11%) with reciprocal significant increase in type IIb fibre proportion (20±16% versus 8±4%). The proportion of type IIa fibres was similar between the two groups.
These results suggest that the contractile properties of the vastus lateralis are preserved in patients with chronic obstructive pulmonary disease. Therefore, the reduction in the quadriceps strength in patients with chronic obstructive pulmonary disease cannot be explained on the basis of an alteration of the contractile apparatus.
- atrophy
- chronic obstructive pulmonary disease
- human skeletal muscle contractility
- muscle biopsy
- peripheral muscle dysfunction
- weakness
R. Debigaré was the recipient of a PhD training award of the Fonds de la Recherche en Santé du Québec. F. Maltais is a Research Scholar of the Fonds de la Recherche en Santé du Québec. This study was supported by CIHR grant no 36331.
Muscle atrophy and weakness are common in chronic obstructive pulmonary disease (COPD) 1, 2. While several studies have investigated peripheral muscle function in COPD, it is still unclear whether the loss in strength can be solely attributed to muscle atrophy or whether a pathological process impairing the contractile function or the excitation:contraction coupling is involved 1–3. If muscle atrophy is the sole factor involved, it could be hypothesised that loss of strength would be proportional to decrease in muscle cross-sectional area. Otherwise, if a muscle dysfunction and/or pathological process are involved then the degree of weakness would not be linearly related to the loss in muscle cross-sectional area (reduced strength/muscle surface ratio). This question is difficult to resolve clinically for two reasons: 1) it is difficult to ascertain whether a maximal muscle contraction has been performed during a voluntary strength measurement manoeuvre; and 2) the actual muscle surface involved during the manoeuvre cannot be accurately quantified.
These difficulties can be overcome by assessing the in vitro contractile properties of muscle bundles obtained through a small open biopsy using electrical field stimulation 4–6. Under such conditions, the maximum force produced is totally independent from motivational factors and the muscle cross-section involved can be estimated with great precision. In the present study, this methodology was used to test the hypothesis that the decreased peripheral muscle strength observed in COPD patients can be entirely explained by atrophy. Thus, this study compared the in vitro contractile properties of isolated bundles of the vastus lateralis muscle in patients with COPD and healthy control subjects in whom in vivo contractile properties of the same muscle were also evaluated.
Methods
Subjects
Sixteen males with COPD were recruited for the study. Diagnosis of COPD was based on smoking history and pulmonary function testing, which confirmed the presence of moderate-to-severe irreversible airflow limitation 7. At the time of evaluation, patients with COPD were stable with no exacerbation of their disease in the preceding 2 months and had not experienced recent weight loss. Patients with COPD that had used systemic corticosteroids in the last 6 months or were under long-term oxygen therapy were excluded. Nine healthy sedentary males of a similar age served as control subjects. In both groups, subjects were excluded if they had prolonged bed rest or presented previous muscle disease. No subjects were involved in any form of exercise training. Only males were included in this study in order to reduce measurement variability. The Ethics Committee of Hôpital Laval, Sainte-Foy approved the study protocol and each patient signed a written informed consent form.
Pulmonary function tests and anthropometric measurements
Standard pulmonary function tests, including spirometry and phlethysmographic lung volumes, were obtained in patients with COPD, according to previously described guidelines 7, and related to normal values of Knudson et al. 8 and Goldman and Becklake 9, respectively. Only spirometry was obtained for control subjects. Height and weight were measured in both groups according to standardised methods 10.
Computed tomography
In order to quantify the mid-thigh muscle cross-sectional area (MTMCSA), a computed tomography of the right thigh halfway between the pubic symphisis and the inferior condyle of the femur was performed before the muscle biopsy, as described previously 2.
In vivo muscle strength measurements
The maximal isometric torque of right knee extensors was measured with the knee flexed at 90° during a static voluntary contraction against an isometric strain gauge (UTC2; Gould-Statham, Cleveland, OH, USA) coupled to a digitised analysing system (MP100; BIOPAC Systems, Santa Barbara, CA, USA). Measurements were performed while subjects were comfortably seated. Both extremities of the strain gauge were firmly fixed under the seat using the frame and the extensor pads as fasteners. To ensure that the best possible efforts were obtained, subjects were carefully instructed to perform maximal effort during exhalation while verbal encouragements were given. Three trials separated by 2 min of rest were performed and the best attempt was kept for analysis.
Muscle biopsy
Muscle biopsies were performed by a general surgeon (F-S. Hould) during a subsequent visit. After shaving and disinfection of the external part of the right thigh, a biopsy of the right vastus lateralis was performed ∼10 cm above the superior border of the patella. Local subcutaneous anaesthesia was achieved using 4 mL of lidocaine (2%) with special attention to ensure that no lidocaine was injected in the muscle. Thus, injection of lidocaine was done superficially and obliquely. After a small cutaneous incision, the vastus lateralis fascia was visualised and cut. Muscle fibres were carefully dissected in their longitudinal axis to obtain a bundle of ∼2.5×0.5×0.5 cm. Both ends were immediately clipped and the bundle was fixed on a cork support at its apparent resting length. The bundle was immediately placed in cold oxygenated Krebs-Ringer bicarbonate solution (NaCl 137, KCl 5, CaCl2 2, MgSO4 1, NaH2PO4 1, NaHCO3 24 and glucose 11 mM) and quickly transported to the laboratory for contractile property evaluation.
In vitro contractile protocol
Muscle bundles were placed in a dissecting bath containing oxygenated Krebs-Ringer bicarbonate solution at room temperature for additional dissection. Silks were tied 5–6 mm proximal to each extremity and further dissection was pursued in such a way that the remaining bundle segment available for contractility assessment was ∼1.5×0.2×0.2 cm, as recommended previously 11. These muscle segments were expected to be viable based on the study of Faulkner et al. 5 showing normal action potential at a distance of ≥5 mm of the cut extremity of a muscle bundle. The dissected bundle was then vertically attached between platinum electrodes to a glass hook and an isometric strain gauge (Grass S48 Stimulator; Grass, Quincy, MS, USA) at its inferior and superior end, respectively, and immediately immerged in a 50 ml organ bath containing Krebs-Ringer bicarbonate solution maintained at 35°C, pH 7.40. The solution was bubbled with a gas mixture comprising 95% oxygen and 5% carbon dioxide in order to oxygenate tissue and maintain pH at 7.40. Following bundle immersion, the optimal muscle length (Lo), i.e. the length at which the peak twitch tension was achieved, was determined using a micrometric screw. After a resting period of 15 min, a twitch contraction was obtained using supramaximal stimulation parameters (2 ms pulse duration; ∼25 V intensity). Peak twitch tension (Pt), time to peak twitch tension (TPT), and half relaxation time (RT1/2) were obtained. After a further 5 min of rest, a force/frequency relationship was constructed using 10, 15, 20, 30, 50, 80, 100, 120 and 150 Hz stimulation to obtain maximal isometric tetanic tension (Po). The contractile protocol, including transportation time to the laboratory, was completed within 60 min. At the end of the contractile protocol, Lo was measured and the bundle was weighed dry and then perpendicularly mounted on a cork piece and frozen in isopentane cooled to freezing point with liquid nitrogen and stored at −70°C until processing for fibre typing. Muscle bundle cross-sectional area (CSA) was estimated from the previously measured bundle weight and Lo, assuming a muscle density of 1.06 g·cm−3 and a uniform section 11.
Skeletal muscle and data analysis
Fibre typing
Histochemical fibre typing of muscle biopsy specimens was carried out as described previously 12. Briefly, muscle samples were cut into 10-μm thick transverse sections in a cryostat at −20°C and stained for myofibrillar adenosine trisphosphatase activity, according to the single-step ethanol-modified technique 13. Staining intensity designated fibre types as type I (nonstained), type IIa (lightly stained) and type IIb (darkly stained). Muscle sections were magnified and transmitted to an image analysing system (Image Pro Plus 4.1 for Windows; MediaCybernetics, Silver Springs, MD, USA) to count and classify fibres and measure their cross-sectional area. This last measurement was calculated based on 40 randomly selected fibres of each type 12, 14.
Statistical analysis
Results of representative measures are expressed as mean±sd. Descriptive variables were analysed using unpaired t-tests. Comparisons between both groups for fibre types were performed using a multivariate one-way analysis of variance. To compare the force/frequency relationships of both groups, a repeated measure design was performed. The normality assumption was verified with the Shapiro-Wilkinson test and the Bartlett's statistic was used to verify the homogeneity of variances. All assumptions were fulfilled. Regression analyses were performed using the least-squared method. The level of statistical significance was set at a p-value of ≤0.05.
Results
Subjects' characteristics
Anthropometric characteristics and pulmonary function data are depicted in table 1⇓. Patients with COPD had a lower body mass index (p<0.05) compared to control subjects. On average, patients with COPD had severe airflow limitations, hyperinflation and a slightly reduced resting oxygen tension in arterial blood.
Patients' characteristics
The in vivo characteristics of the vastus lateralis muscle are shown in table 2⇓. Patients with COPD had significant reductions in isometric strength and MTMCSA (p<0.05) compared to control subjects. The isometric strength/MTMCSA ratio was significantly lower in patients compared to healthy subjects. In both groups, there was no statistically significant difference in isometric strength between the three repetitions, the difference between repetition one and three averaging 3%.
In vivo peripheral muscle characteristics
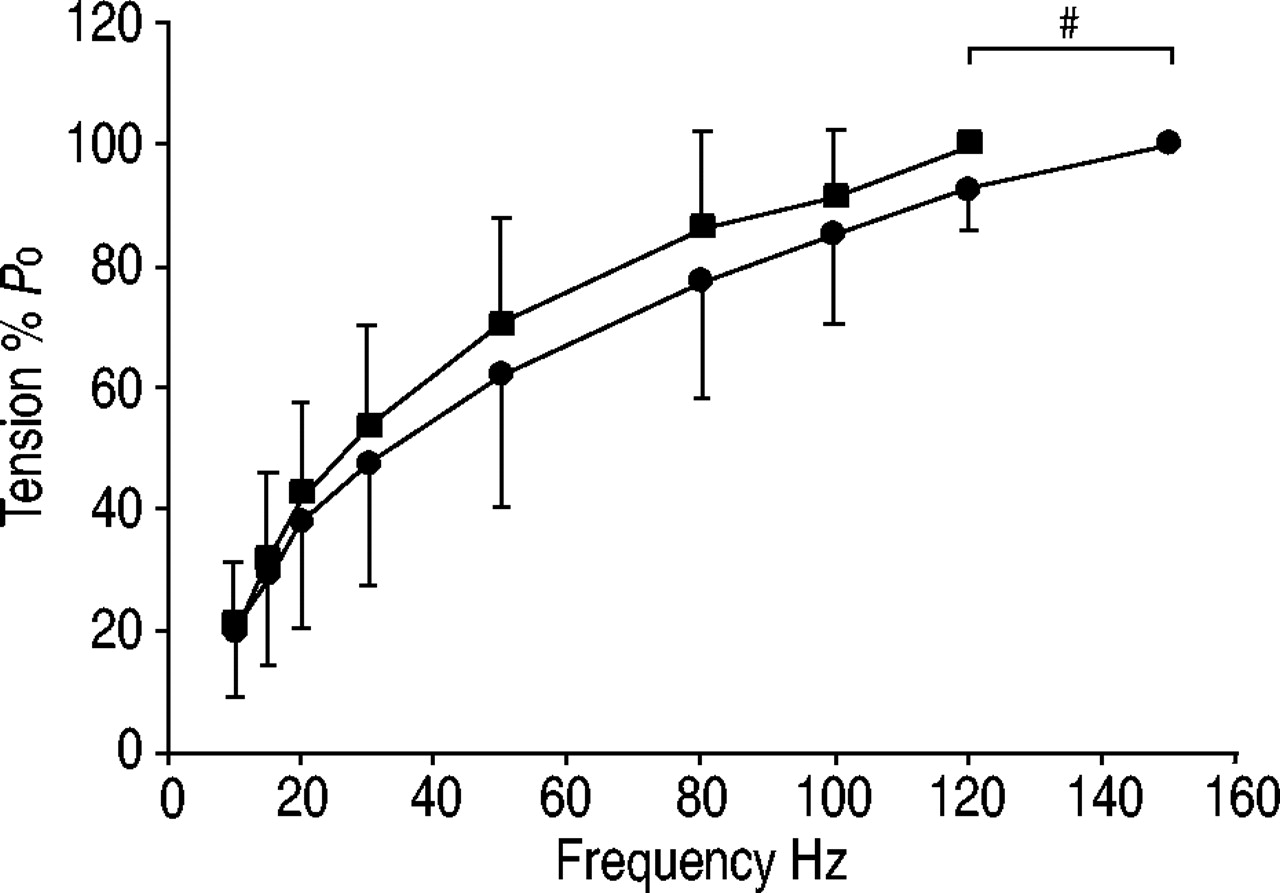
The in vitro contractile properties of muscle bundles are provided in table 3⇓. Lo and muscle bundle CSA were not significantly different between both groups. Group mean values for Po, Po corrected for muscle bundle CSA and Pt/Po are shown in figure 1⇓. All contractile parameters measured, including Po corrected for muscle bundle CSA, were similar in both groups. There was a significant correlation between isometric strength/MTMCSA ratio and Po corrected for muscle bundle CSA (r=0.56, p=0.015). There was no correlation between in vitro muscle force and disease severity. The force/frequency relationships for the two groups are shown in figure 2⇓. This relationship tended to be shifted to the right in COPD as a higher stimulation frequency was necessary to produce the same relative force. Also, the stimulation frequency required to elicit Po tended to be higher in patients with COPD compared to control subjects (150±36 versus 122±42 Hz; p=0.09).
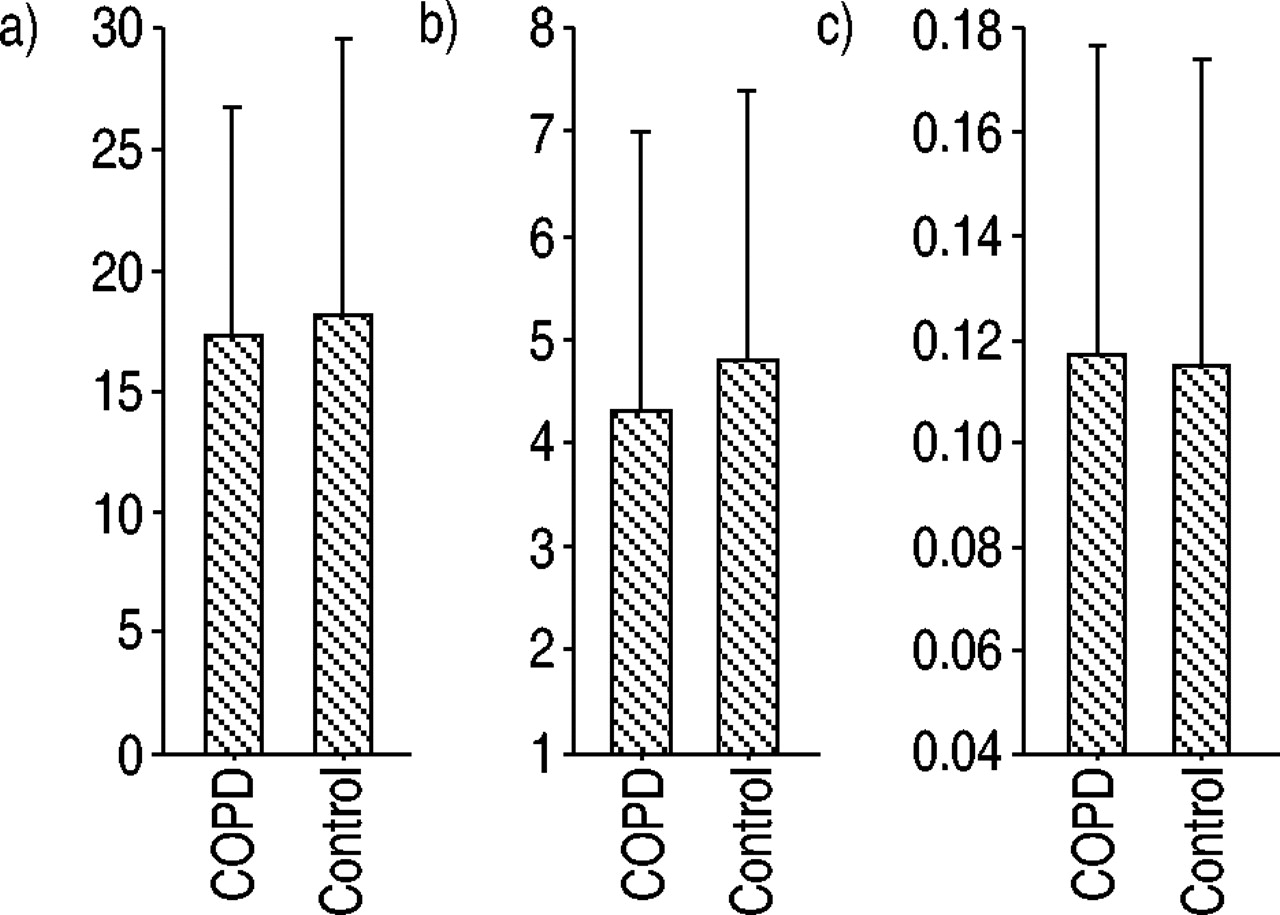
Group mean values for a) maximal isometric tetanic tension (Po), b) Po corrected for muscle bundle cross-sectional area and c) maximal isometric twitch tension (Pt)/Po ratio of vastus lateralis muscle bundles for chronic obstructive pulmonary disease (COPD) (n=16) and controls (n=9). There was no significant difference between both groups for these values. Data are presented as mean±SD.
{kind=link}
{kind=link}
The force/frequency relationship of vastus lateralis muscle bundles for chronic obstructive pulmonary disease (COPD) (n=16) and controls (n=9). The force/frequency relationship tended to be shifted to the right in patients with COPD; a higher stimulation frequency was necessary to produce the same relative force. The stimulation frequency needed to elicit the maximal isometric tetanic tension (Po) tended to be greater in patients with COPD compared to control subjects. Data are presented as mean±SD.
Muscle bundle characteristics and in vitro twitch contractile properties of vastus lateralis in both groups
Muscle fibre-typing could be obtained in 11 patients with COPD and eight control subjects. The mean total number of fibres counted was similar in both groups and averaged 604±273 and 543±342 for COPD and control subjects, respectively. Patients with COPD had a lower proportion of type I fibre than controls (26±12% versus 39±11%, p=0.02) with reciprocal significant increase in type IIb fibre proportion (20±16% versus 8±4%, p=0.04). The proportion of type IIa fibres was similar between the two groups. Compared to controls, the CSA of type I (4,802±1,723 µm−2 versus 5,793±2,118 µm−2, p<0.05) and type IIa fibres (4,782±1,762 µm−2 versus 5,273±2,139 µm−2, p<0.05) were significantly reduced in COPD. There was no significant difference in the CSA of type IIb fibres between both groups (3,593±1,683 µm−2 versus 3,721±1,713 µm−2, p>0.05).
Discussion
The precise mechanisms leading to peripheral muscle dysfunction in COPD are still poorly understood and several contributing factors, such as hypoxaemia 15, inactivity 16, malnutrition 17, inflammation 18 or even the presence of a myopathy 19, have been proposed. By measuring the in vitro contractile properties of bundles from the vastus lateralis muscle obtained through open biopsy, the intrinsic ability of the muscle to generate tension independently of volitional activation was investigated. Although the in vivo data suggest a disproportionally greater reduction in muscle strength than cross-section, the in vitro contractile properties of the vastus lateralis bundles from patients with COPD and in healthy subjects do not differ significantly. The fact that maximum tetanic tension values corrected for muscle bundle CSA were similar in both groups suggests that the contractile apparatus of the vastus lateralis functions normally in COPD patients not using systemic corticosteroids. This is an important finding since it implies that therapeutic strategies aimed at gaining muscle mass should lead to a direct increase in strength.
In vitro contractility studies can be easily performed in animals in which intact muscle-tendon units can be obtained. Apart from intercostal preparation, intact muscle cannot be harvested in live humans. A protocol allowing the study of sectioned human muscle bundles was initially developed to compare the contracture responses of human muscles to different drugs in order to determine the susceptibility to developing malignant hyperthermia 20. Subsequently, Moulds et al. 4 succeeded in measuring in vitro contractile properties of human muscle bundles with cut ends that were harvested during general anaesthesia. To the best of the authors' knowledge, this study is the first showing that human muscle bundles allowing measurement of in vitro contractile properties can be obtained under local anaesthesia.
The validity of the in vitro contractile property measurements of sectioned muscle bundles in comparison to intact muscles has been evaluated by Faulkner et al. 5. It was found that speed of contraction and relaxation and Pt/Po was not affected by cutting muscle fibres. However, absolute and normalised values for Pt and Po of sectioned fibres are expectedly lower than in intact fibres, which results from fibre damage and reduced membrane potentials at the extremities of a sectioned muscle bundle 5 contributing to impaired fibre depolarisation. In the present investigation, it was ensured that all muscle bundles were harvested and prepared in an identical fashion. As such, the underestimation in Po and Pt made from the study of sectioned muscle bundles was likely to be of similar magnitude in all samples and, consequently, in both groups of subjects. This statement is further supported by the fact that Po/Pt, a marker of muscle bundle quality and viability, was similar in both groups. Based on this, the authors believe that the comparison of these variables in healthy subjects and patients with COPD in this study is entirely justified.
As in other studies 4, 5, the in vitro contractile parameters had relatively large standard sds. Such a variation is expected considering that, despite close attention to technical details (all biopsies were performed by the same surgeon and all the contractile studies were carried out by the same investigator), subtle differences in tissue harvesting and preparation from one individual to another may influence the viability of the tissue. In spite of this, the validity of the in vitro measurements is supported by several observations. As previously recommended, measurements were confined to muscle segments located 5–6 mm from each extremity in order to ensure electrophysiological viability 5 and to minimise sarcomere damages. In addition, the ranges and mean values for Po were similar to those previously reported in bundles with both extremities sectioned either in humans 4 or animals 5. Lastly, the existing correlation between isometric strength/MTMCSA ratio and Po corrected for muscle bundle CSA, gives credence to the measurements in this study.
In the present study, in vitro measurement of contractile properties of muscle bundles allowed the study of muscle function independently of voluntary motor unit recruitment. The similarity of Po·cm−2 observed in healthy subjects and patients with COPD does not support the hypothesis that a myopathic process exists in the latter group, since the decrease in strength in this condition would be disproportionately greater than loss in muscle CSA, indicating an impairment of the contractile apparatus 21, 22. At first sight, this result may appear surprising given the common belief that type II fibres, whose proportion is increased in COPD, are stronger than type I fibres. In contrast, the body of literature on force production in mammalian skeletal muscle made it quite clear that specific Po does not vary significantly among the different fibre types 23. Thus, the conclusion of a similar Po·cm−2 between COPD and healthy subjects is independent of the difference in the fibre-type distribution present in the two groups. Another argument supporting the absence of a generalised myopathic process in COPD is the observation that the level of impairment in muscle function is not equally distributed among all muscle groups, as indicated by the relative preservation of the strength of the upper limb muscle 24. Lastly, the fibre-type distribution of the upper limb muscle in COPD is not different to that of healthy individuals 25, while the diaphragm in emphysema shows favourable change in the fibre-type profile consistent with an adaptation to chronically increased work of breathing 26–28. All together, the current knowledge about skeletal muscle function in COPD is not consistent with a generalised myopathy, at least in patients not recently exposed to systemic corticosteroids.
Speed-related contractile parameters, such as TPT and RT1/2, are influenced by the myosin heavy chain composition and kinetics of calcium exchange/handling. Values obtained in this study for TPT and RT1/2 in both groups of subjects are similar, suggesting no difference in intramuscular Ca2+ ion kinetics. This observation is consistent with the modest difference in the fibre-type distribution, and presumably in the myosin heavy chain composition 29, observed here between patients with COPD and control subjects. Based on previous studies, where larger samples of patients were studied, a greater difference in the fibre-type distribution of vastus lateralis muscle between COPD and control subjects was expected 12. The proportion of type I fibres in the present control group was somewhat lower than that usually found in individuals of the same age group 30. This could probably be explained by the small sample size of the present study and by the typical variation in the fibre-type profile in the healthy population, since ∼25% of normal males have <50% of type I fibre in their vastus lateralis muscle 31.
One interesting aspect of the present study is that both in vivo and in vitro measurements of peripheral muscle function were obtained in the same individuals. Although subjects were carefully instructed to perform a maximal effort during the strength measurement manoeuvre, it cannot be confirmed whether this goal was achieved in all circumstances. Patients with advanced lung disease may have greater difficulty in fully activating their muscle compared to healthy subjects, leading to a possible underestimation of the force/MTMCSA ratio. Another possible explanation for the low force/MTMCSA ratio in patients with COPD is an overestimation of MTMCSA by the computed tomography analysis due to a greater amount of fat or connective tissue between muscle fibres. This possibility is unlikely for two reasons: 1) the tissue whose density corresponded to fat was specifically removed from the analysis; and 2) although it cannot be ruled out from the computed tomography analysis that a greater proportion of the thigh section was occupied by connective tissue between muscle fibres, this possibility is inconsistent with the similar in vitro Po·cm−2 in both groups. Nevertheless, these potential difficulties with the in vivo muscle function evaluation underscore the significance of the in vitro experiment in the investigation of the origin of weakness in COPD.
Measurement of Po·cm−2 using cut bundles is intrinsically associated with a high variability and it could be questioned whether the lack of a statistically significant difference in Po·cm−2 between healthy subjects and patients with COPD is due to a type II error. Using the present set of data, it was calculated that ∼800 subjects (400 in each group) would be necessary to demonstrate that the observed 10% difference in Po·cm−2 between the two groups reaches statistical significance with a power of 80%. However, if present, such a modest difference in Po·cm−2 cannot account for the 30% reduction in quadricep strength found in patients with COPD in this and other studies 2. Based on these considerations, the conclusion that impairment in the muscle contractile apparatus is not the major cause of muscle weakness in COPD is justified.
In conclusion, the measurements of in vitro contractile properties of the vastus lateralis muscle were similar in patients with chronic obstructive pulmonary disease and healthy sedentary subjects, except for a right shift of the force/frequency relationship of the former group consistent with a modest difference in fibre-type distribution. Therefore, the reduction in the quadriceps strength cannot be explained on the basis of an alteration of the contractile apparatus and the results of this study do not support the presence of a myopathic process in patients with chronic obstructive pulmonary disease.
Acknowledgments
The authors acknowledge the contribution of B. Lapointe, A. Michaud and M. Doucet for their technical assistance, S. Simard for his statistical assistance, and M. Bélanger, M-J. Breton, L. Petitclerc and nurses of the surgical outpatient clinic for their help in accomplishing this study. They also thank J. Frenette and F. Sériès for their helpful suggestions regarding the manuscript.
- Received May 1, 2002.
- Accepted September 2, 2002.
- © ERS Journals Ltd
References









