





Abstract
Scandinavian human leukocyte antigen-DR17-positive (DR17+) sarcoidosis patients are characterised by a good prognosis. They also reveal an accumulation in bronchoalveolar lavage fluid of T‐lymphocytes expressing the T‐cell receptor V gene segment AV2S3 at disease onset. The authors of this study wished to establish whether AV2S3 T‐lymphocyte accumulation changes from disease onset to clinically resolved disease and how this relates to other activity parameters.
Bronchoalveolar lavage fluid and serum from nine DR17+ sarcoidosis patients were examined at disease onset and after spontaneous resolution of clinical and radiographical signs of disease.
Nine DR17+ patients with lung accumulated CD4+ AV2S3+ T‐cells were investigated after clinically recovery. At re-examination the percentage of CD4+ AV2S3+ lymphocytes in bronchoalveolar lavage fluid was normalised (29 versus 5.4%). A significant reduction in lymphocyte percentage (14 versus 4.4%) and a decrease in cellular concentration (179×106·L−1 versus 111×106·L−1) and CD4/CD8 ratio (5.2 versus 2.4) were also seen. In serum, the activity of angiotensin-converting enzyme (24.9 versus 14.0 U·mL−1) as well as the levels of neopterin (7.8 versus 5.3 nmol·L−1) decreased significantly after recovery.
These results indicate that the locally accumulated AV2S3 positive T‐lymphocytes in bronchoalveolar lavage are involved in the pathogenic process of sarcoidosis in this patient group.
This study was supported by the Swedish Medical Research Council (K2002-74X-14182-01A), the Swedish Heart-Lung Foundation, the King Oscar II Jubilee Foundation and the Karolinska Institutet.
Sarcoidosis is characterised by the accumulation of lymphocytes, preferentially CD4+ cells, at the site of inflammation. Since CD4+ lymphocytes are suggested to direct immune reactions these cells have gained special interest. Although the disease may affect almost any organ, lung involvement occurs in >90% of patients 1. Therefore, the study of bronchoalveolar lavage (BAL) fluid (BALF) cells and soluble components is a widespread method to increase knowledge of pathological processes involved in this disease. Several parameters in BALF, such as the cellular profile and lymphocyte subsets, are also reported to reveal diagnostic, prognostic or disease activity information 2–4. However, most of these data are based on comparisons between sarcoidosis patients and controls, and not on follow-up in individual patients over a longer period. Disease activity may also be judged from serum markers, such as angiotensin-converting enzyme (ACE), although this has limitations with respect to sensitivity and specificity.
Previously, the current authors have reported that the human leukocyte antigen (HLA) class II allele DR17 (DRB1*0301) is over-represented in Scandinavian sarcoidosis patients, 33% compared to 17% in the normal population 5. DR17-positive (DR17+) patients share several clinical features, such as an acute disease onset, often with Löfgren's syndrome, and a favourable prognosis with an increased rate of spontaneously resolving disease within 2 yrs from disease onset. Interestingly, at disease onset these patients reveal a restricted expansion in BALF of CD4+ lymphocytes expressing the T‐cell receptor (TCR) V gene segment AV2S3 6. This restricted TCR usage in Scandinavian DR17+ subjects seems to be limited to sarcoidosis and supposedly reflects a reaction towards a specific antigen.
The main purpose of this study was to investigate if a former CD4+ AV2S3+ lymphocyte expansion in BALF from HLA-DR17+ sarcoidosis patients diminishes with clinical normalisation, i.e. disappearance of clinical symptoms and normalised chest radiography and pulmonary function.
The authors also wished to study, from disease onset to clinical normalisation, the natural course of some previously suggested activity markers in BALF and serum in this distinct sarcoidosis group.
Methods
Study subjects
Nine Scandinavian HLA-DR17+ patients presenting a typical clinical picture for sarcoidosis, with bilateral hilar lymphadenopathy without (n=7) or with (n=2) parenchymal infiltrates on chest radiography 1, were included in the study. All presented with Löfgren's syndrome, i.e. bilateral hilar lymphadenopathy (BHL), fever, erythema nodosum and/or ankle arthritis 7. Three of the patients had a positive transbronchial biopsy and one had a positive Kveims test. BALF and peripheral blood (PBL) samples from the included patients were examined at disease onset (BAL1) and after clinical resolution of disease at least 2 yrs later (BAL2). Clinical resolution was defined as disappearance of symptoms (dry cough, fever, fatigue, arthralgia), normalisation of chest radiography and a normal spirometry. None was prescribed systemic or topical corticosteroid therapy within 3 months before BAL examinations. In all subjects clinical and radiographical signs of disease spontaneously resolved without any pharmacological therapy within 2 yrs of onset. The characteristics of the patients are presented in table 1⇓.
Clinical data of the study group
All included subjects gave their informed consent for participation. The study was approved by the local ethics committee at the Karolinska Hospital, Stockholm, Sweden.
Bronchoalveolar lavage and bronchoalveolar lavage fluid cell preparation
BAL was performed under local anaesthesia with a flexible fibreoptic bronchoscope (Olympus Optical Co. ltd, Tokyo, Japan) wedged in a subsegment of the middle lobe. Sterile, 37°C 0.9% saline solution was instilled and gently aspirated in five aliquots of 50 mL. The recovered fluid was kept on ice in a siliconised plastic bottle until analysis 8. After filtration of BALF through a Dacron net (Millipore, Cork, Ireland), BAL cells were separated by centrifugation in 4°C at 400×g for 10 min. Total and viable cells were counted in a Bürker chamber after staining with trypan blue.
The cells underwent cytocentrifugation at 500 rates·min−1 for 3 min (Cytospin2; Shandon, Runcorn, UK). The cellular differentiation was counted after staining with May-Grünwald and Giemsa solutions.
Immunostaining and flow cytometry
Cells obtained from BALF and PBL were labelled and analysed as previously described 9. Cells were labelled with RPE-Cy5-conjugated monoclonal antibodies (mAb) against CD4, RPE-conjugated mAb against CD8 (Dako, Glostrup, Denmark) and flourescein isothiocyanate (FITC)-conjugated mAb against CD3 (Dako) and AV2S3 (Serotec, Oxford, UK). As a negative control an FITC-conjugated anti-immunoglobulin G mAb (Dako) was used in all cell experiments, staining <1% of the cells. The cellular antigen expression was analysed in a flow cytometer (FACScalibur; Becton Dickinson, Mountain View, CA, USA). Lymphocytes from BALF and PBL were gated by light scattering properties. Dot plots were made for analysing the expression of respective FITC-conjugated mAb for CD4+ and CD8+ cells.
Preparation of cells from peripheral blood and serum analysis
Gradient centrifugation with Ficoll-Hypaque (Pharmacia, Uppsala, Sweden) was used for the separation of mononuclear cells from PBL. Serum was separated from venous blood samples taken at the time of BAL and centrifuged at 800×g for 10 min (Labofuge 200; Heraeus, Sepatech GmbH, Osterode, Germany) and was immediately sent for analysis (ACE) or frozen at −70°C until analysis (neopterin). Serum activity of ACE (SACE) was analysed with a colorimetric kit (Fujirebio, Tokyo, Japan) at the routine chemistry laboratory at Karolinska Hospital. The upper normal value was set at 32 U·mL−1. Enzyme-linked immunosorbent assay was used for the determination of neopterin (ELItest Neopterin; Brahms Diagnostica GmbH, Berlin, Germany) in serum.
Pulmonary function tests
Forced expiratory volume at one second (FEV1) and vital capacity (VC) were measured using a Sensor-Medics 2400 spirometer (Sensor-Medics, Waldbüttelbrunn, Germany). FEV % was calculated as the ratio between FEV1 and VC. The carbon monoxide diffusing capacity of the lung (DL,CO) was analysed by the single-breath technique. The results of VC and FEV1 are presented as % of predicted 10.
Analysis
The nonparametric Wilcoxon test and Mann-Whitney U‐test were used for comparisons of paired and nonpaired data, respectively. Results are presented as medians. A p‐value of <0.05 was considered significant.
Results
Cellular composition and CD4+ AV2S3 expression in bronchoalveolar lavage T‐cells
The percentage of CD4+ lymphocytes in BALF expressing AV2S3 decreased markedly in every patient from BAL1 to BAL2 (29 versus 5.4%, p<0.01) (fig. 1⇓).

Percentage of CD4+ bronchoalveolar lavage (BAL) fluid cells in patients (n=9) expressing AV2S3 at BAL1 and BAL2. Median values are presented as horizontal bars. ○: patient no. 1; □: patient no. 2; ⋄: patient no. 3; ▵: patient no. 4; •: patient no. 5; ▪: patient no. 6; ♦: patient no. 7; ▴: patient no. 8; ▾: patient no. 9. **: p<0.01.
This reduction was paralleled by a significant decrease in the ratio between the percentage of CD4+ lymphocytes expressing AV2S3 in BALF and PBL from BAL1 to BAL2 (6.9 versus 1.2, p<0.05).
With individual exceptions, the cellular concentration in BALF in general decreased from BAL1 to BAL2 (179×106·L−1 versus 111×106·L−1, p=0.05) (fig. 2a⇓).

Bronchoalveolar lavage (BAL) fluid parameters in patients at BAL1 and BAL2 (n=9). Median values are presented as horizontal bars. a) Cell concentration. b) Percentage of lymphocytes. c) CD4/CD8 ratio. ○: patient no. 1; □: patient no. 2; ⋄: patient no. 3; ▵: patient no. 4; •: patient no. 5; ▪: patient no. 6; ♦: patient no. 7; ▴: patient no. 8; ▾: patient no. 9. **: p<0.01; #: p=0.05; ¶: p=0.07.
The same trend was seen for relative numbers of lymphocytes (14 versus 4.4%, p<0.01) (fig. 2b⇑), while a corresponding increase in the percentage of alveolar macrophages was found (84 versus 94%, p<0.05). No significant difference was found in relative numbers of neutrophils, eosinophils or basophils between BAL1 and BAL2. A strong tendency towards a decrease in BALF CD4/CD8 ratio was seen between BAL1 and BAL2, although not statistically significant (5.2 versus 2.4, p=0.07) (fig. 2c⇑).
Serum activity of angiotensin-converting enzyme and neopterin
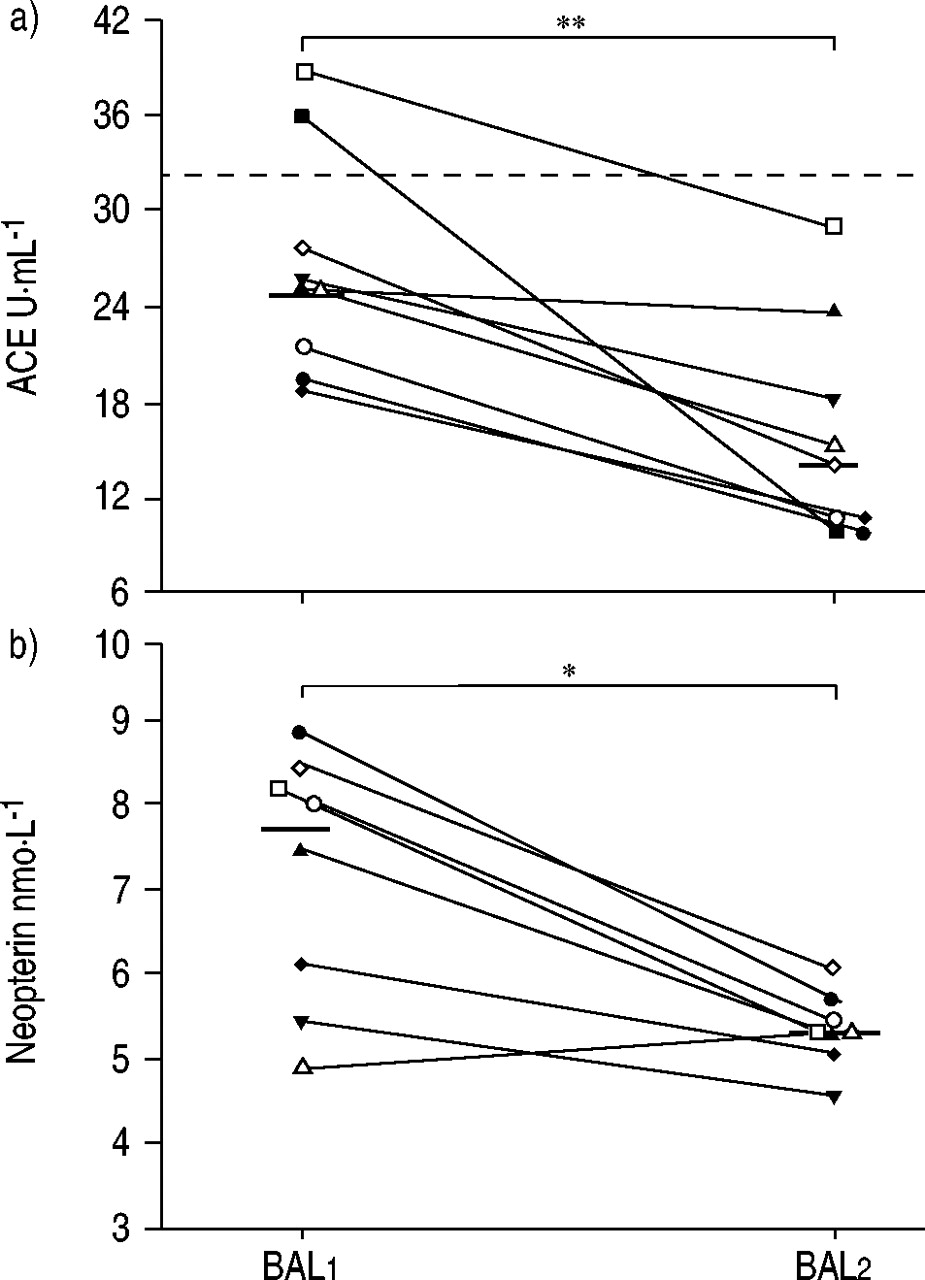
SACE activity was higher at BAL1 than at BAL2 (24.9 U·mL−1 versus 14.0 U·mL−1, p<0.01). The decrease led to normalisation in SACE in the two patients who presented with SACE above the upper reference value at disease onset (fig. 3a⇓). A similar decrease in S‐neopterin was found (7.8 versus 5.3 nmol·L−1, p<0.05) (fig. 3b⇓).
{kind=link}
{kind=link}
{kind=link}
Serum parameters in patients at bronchoalveolar lavage (BAL1) and (BAL2). Median values are presented as horizontal bars. a) Angiotensin-converting enzyme (ACE) (n=9). ----: upper reference value. b) Neopterin (n=8). ○: patient no. 1; □: patient no. 2; ⋄: patient no. 3; ▵: patient no. 4; •: patient no. 5; ▪: patient no. 6; ♦: patient no. 7; ▴: patient no. 8; ▾: patient no. 9. *: p<0.05; **: p<0.01.
Pulmonary function tests
Although results were within the normal range for all examined patients (n=8) at BAL1, a minor increase could be seen in both FEV1 (98 versus 101%, p<0.05) and VC (104 versus 110%, p<0.05) at BAL2, although no difference in FEV % was revealed during the same period (data not shown). No significant change could be seen in DL,CO between onset and follow-up, however, this test was unfortunately only performed in five patients initially (data not shown).
Discussion
In this study, several clinical and inflammatory parameters have been compared in a distinct group of sarcoidosis patients at disease onset and after ≥2 yrs when the disorder clinically had resolved, i.e. following disappearance of symptoms and normalisation of chest radiography and improvement of pulmonary function. This patient group, HLA-DR17+, make up one third of all Scandinavian sarcoidosis patients 5.
The alveolitis in sarcoidosis is characterised by an accumulation of lymphocytes, preferentially of the CD4 subset 1. Several attempts have been made to use the percentage of lymphocytes and the ratio between CD4+ and CD8+ BAL lymphocytes for diagnostic and prognostic purposes. An increased CD4/CD8 ratio, >3.5–4.0, has been reported to be highly specific for sarcoidosis 4, 11, 12, while a decrease has been suggested to be prognostically unfavourable 13, 14. In a previous study, the current authors reported an increased CD4/CD8 ratio in the BALF of HLA-DR17+ sarcoidosis patients compared to HLA-DR17- patients, although there were exceptions 15. Also in the present study, it was found that although most patients clearly had elevated CD4/CD8 ratios, there were notable exceptions without any obvious relation to prognosis. A normalisation in cell concentration, percentage of lymphocytes and CD4/CD8 ratio could be seen in the BALF from most patients between BAL1 and BAL2, indicating that the alveolitis resolved. When comparing the BALF CD4/CD8 ratio between patients from this study and 25 healthy subjects from an ongoing study, an initial significant increase at BAL1 (5.2 versus 2.1, p<0.01) was normalised at BAL2 (2.4 versus 2.1, p>0.05) (personal observations).
However, exceptions in BAL2 existed; one patient had a persistent BAL-lymphocytosis and two others had a CD4/CD8 ratio >3.5. Although no signs of clinical disease remained, these findings may reflect a subclinical alveolitis in these patients. This assumption is further strengthened by the fact that these deviations were seen in three of the patients with a relatively short interval between the two examinations, ∼2 yrs.
A restricted usage of certain TCR gene products in active sarcoidosis at the site of inflammation has previously been reported 16, 17. The patients in this study were also characterised at BAL1 by such a restricted usage of the TCR gene segment, AV2S3. A significant decrease in the percentage of CD4+ AV2S3+ BALF lymphocytes at BAL2 was seen, with a complete normalisation in every patient investigated. These results confirm the hypothesis, based on preliminary data from a few, incompletely followed patients 6, that the AV2S3 percentage in BALF is associated with clinical signs of disease activity in DR17+ sarcoidosis patients. A recently published case report also supports this correlation 18. Thus, in this selected group of patients, the relative numbers of AV2S3+ BAL T‐cells may be a more sensitive marker of disease activity than the CD4/CD8 ratio, for example.
It may be speculated that changes in the accumulation of AV2S3+ CD4+ lymphocytes precede changes in the CD4/CD8 ratio in BALF. In patient no. 8 the CD4/CD8 ratio increased from BAL1 to BAL2 while the accumulation of AV2S3+ cells decreased to normal levels during the same time. This patient did not differ clinically from the other patients. In addition, patient no. 7 revealed a lasting increase in the CD4/CD8 ratio at BAL2 although a normalisation in AV2S3 expression had occurred. Moreover, at an additional BALF analysis in patient no. 7, 10 months before BAL2 and before complete clinical recovery, the AV2S3 expression of CD4+ cells as well as the CD4/CD8 ratio remained high, 31 and 6.6%, respectively.
Why do T‐cells express this V gene segment in sarcoidosis? The present authors previous finding of a near 100% association between a restricted usage of the TCR V gene segment and HLA-DR17 6, and HLA DRB3*0101 in a recent study 19, in Scandinavian sarcoidosis patients may reflect a reaction towards a specific antigen presented by DR17 (or DRB3*0101) molecules. Such antigen-driven restricted TCR V gene segment usage has been reported in other conditions 20. However, both the origin of a possible antigen, extrinsic or endogenous, and the role of the AV2S3+ lymphocytes are still elusive. The normalisation of the AV2S3 usage in BALF at follow-up may reflect a successful elimination of such a disease-triggering antigen. This speculation is in line with the present authors' previous observation of an association between the percentage of AV2S3+ cells in BALF and disease duration 21.
At disease onset only two patients revealed ACE activity in serum above the normal range. This was expected since the ACE activity in patients with Löfgren's syndrome has been shown to remain normal 6–8 weeks after clinical disease onset 22 and the majority of the patients in the current study were examined within this time. However, interestingly, SACE was reduced in all patients at BAL2 compared to BAL1, suggesting that individual SACE values may be informative with regard to disease activity.
Neopterin is a derivate from activated cells of the monocyte/macrophage lineage. Serum 23 and urine levels are increased in patients with active sarcoidosis and it has been proposed to be an indirect marker for the activity of the T‐helper 1 cytokine interferon‐γ 24. The decrease in S‐neopterin at BAL2 compared to BAL1, found in all but one patient in the current study, probably reflects a reduction in immunological activity. When comparing S‐neopterin levels from patients included in this study and 10 healthy controls previously described 15, an initial difference for patients at BAL1 had disappeared at BAL2 (7.8 versus 5.3 nmol·L−1, p<0.05 and 5.3 nmol·L−1 in both groups, respectively).
The increase in VC from BAL1 to BAL2 seen in all patients might reflect a reversible component in pulmonary compliance 25, and the increase in FEV1 during the same time may be secondary to this increase in VC. Although statistically significant, the differences in pulmonary function tests that were found, seem to be of limited clinical use since the individual change is small and the results are within normal range at both examinations.
In conclusion, this study of a well-characterised patient group reveals a clear association between the disappearance of clinically objective signs of sarcoidosis, including normalised chest radiography, and the reduction of several disease activity markers in bronchoalveolar lavage fluid and serum. This association supports the usefulness of some previously established activity markers in clinical practice. Furthermore, the results suggest that in this particular patient group the relative numbers of AV2S3-positive CD4-positive T‐cells in bronchoalveolar lavage fluid could be used to access disease activity. The complete normalisation of CD4-positive AV2S3-positive lymphocytes in bronchoalveolar lavage fluid at clinical resolution further establishes the involvement of these cells in the pathogenesis of sarcoidosis in Scandinavian human leukocyte-DR17 patients though further studies are needed to understand their exact role.
Acknowledgments
The authors would like to give special thanks to B. Dahlberg, M. Dahl and G. De Forest for technical assistance and O. Olerup for the human leukocyte antigen typing.
- Received July 5, 2002.
- Accepted August 5, 2002.
- © ERS Journals Ltd
References









