





Abstract
Based on recent guidelines for the management of community-acquired pneumonia, this study was designed to evaluate the effectiveness of a new fluoroquinolone compared with standard antimicrobial regimens, in conditions relating as closely as possible to the real world setting.
In this study, 564 patients were randomised to either oral moxifloxacin (400 mg o.d.) or to standard oral therapy (amoxicillin 1 g t.i.d. or clarithromycin 500 mg b.i.d. alone or in combination) for up to 14 days using a double-blind procedure. The choice between the three standard regimens was made by the clinician prior to randomisation. Clinical response, quality of life, symptoms, healthcare resources and safety were assessed.
In the per-protocol population, clinical success was reported for 201 of 215 (93.5%) and 217 of 231 (93.9%) in the moxifloxacin and standard groups, respectively, at 7–10 days post-therapy. At 28–35 days follow-up, continued clinical cure was observed in 183 of 192 (95.3%) moxifloxacin and 207 of 221 (93.7%) standard groups. Drug-related adverse events were reported in 55 of 274 (20%) moxifloxacin and 86 of 279 (31%) standard patients with diarrhoea >5%.
Oral moxifloxacin monotherapy was as effective as, and better tolerated than, optimal antibiotic strategy represented either by mono- or combination therapy (amoxicillin and/or clarithromycin) in community-acquired pneumonia management.
This study was funded by Bayer AG, Wuppertal, Germany.
Community-acquired pneumonia (CAP) is a frequent cause of morbidity and mortality in Europe. Incidences range from >800,000 per year in Spain to >1 million per year in Italy. Incidence rates in Germany, France and the UK have also been reported between these estimates 1, 2. Overall, there are >3 million cases of CAP annually in Europe compared with an estimated 2–3 million seen in the USA each year 3. In the USA, CAP is the sixth leading cause of death and the fifth cause in those >65 yrs of age, accounting for ∼90,000 deaths in 1997 4, 5. Of these, up to 20% will be hospitalised 6, resulting in major financial impact 7. Hospitalisation is the prime driver of CAP-associated costs, as shown by Fine and co-workers 8, 9, who developed criteria to predict either mortality or increased morbidity, the Pneumonia Severity Index (PSI) 8. Clearly, both patients and the healthcare system would benefit if patients could be appropriately treated out of hospital or discharged earlier 9.
Several new approaches to the management of CAP have been published, including those of the Infectious Diseases Society of America 10, the Canadian Infectious Disease Society-Canadian Thoracic Society 11, the European Respiratory Society 12, the Drug-Resistant Streptococcus pneumoniae Therapeutic Working Group 13 and the American Thoracic Society (ATS) 14.
In this context, the CAP 2000 study was developed to compare the main current antimicrobial treatments and their outcomes in CAP, in situations as closely related as possible to the general practice setting. The study compared a third-generation fluoroquinolone, moxifloxacin, given as a single first-line with a comparative arm, where the choice was given to investigators between a β‐lactam, a macrolide or the combination of both. The selected products and their dosages were fixed and chosen according to guideline recommendations.
Material and methods
Study design
This phase IIIb study was designed to compare the effectiveness of moxifloxacin with standard recommended therapy. The choice of the standard regimen was made by the investigator prior to randomisation based on clinical presentation. Patients were then randomly allocated to either moxifloxacin 400 mg o.d. orally or to one of three possible treatment options in the standard group, amoxicillin 1 g t.i.d., clarithromycin 500 mg b.i.d., or the association of both regimens, according to a double-blind procedure, where both the patient and clinician did not know which treatment was administered. In both arms, patients received between 5–15 days of treatment.
Patients eligible for inclusion in the study were ≥18 yrs of age with CAP clinically documented by the presence of fever, an elevated white blood cell count (>100,000 µL−1), signs or symptoms of pneumonia and a new or progressive infiltrate on a chest radiograph. Patients were excluded for the following reasons: allergy to fluoroquinolones, pregnancy or lactating, hospitalisation for >48 h, rapid fatal underlying disease, history of fluoroquinolone tendinopathy, severe liver or renal impairment, administration of another investigational drug within 90 days of enrolment in the study, previous enrolment in this study, drugs treatment known to affect cardiac output interval and previous systemic use of antibiotics for >24 h prior to enrolment. The study was approved by the institutional review board and all patients gave written, informed consent prior to enrolment.
Patients were examined at days 3–5 of treatment, days 7–10 (test of cure visit) and days 28–35 after the end of treatment. Clinical assessment included physical examination, blood pressure, cardiac frequency, respiration rate and mental state (on entry only). Temperature was recorded every 12 h for the first 5 days. Positive chest radiology was needed for inclusions, subsequent radiographs were at the discretion of the investigator. Similarly, bacteriological examinations were optional. Routine laboratory examinations of blood parameters were taken at the start of the study and followed in cases of abnormality or if deemed necessary by the investigator.
Symptoms were recorded with a specific 18-item questionnaire, the CAP-symptom, developed and validated within this study 15. Quality of life was measured using a generic questionnaire the Acute MOS 36-Item Short-Form Health Survey (acute SF-36), at the beginning and end of the patient's inclusion in the study, with calculation of the SF-36 Physical Component Summary score (PCS), SF-36 Mental Component Summary score (MCS) and the eight SF-36 dimension scores 16. In addition, the vitality subscale of the acute SF-36 was also used at days 3–5 and at test of cure. Healthcare resource utilisation, such as concomitant medications, diagnostic and therapeutic procedures, hospitalisation and visits to medical staff, were recorded. The parameters to calculate the PSI 8 for analysis were also collected at baseline. The consumption of main healthcare resources were described in the two treatment arms.
The clinical response at days 3–5, at test of cure and at days 28–35 after the end of the drug treatment was graded in three stages: 1) continued clinical cure (disappearance of acute signs and symptoms related to the infection maintained throughout the follow-up period); 2) clinical relapse (clinical cure at test of cure, with subsequent reappearance of signs and symptoms of CAP requiring antibacterial therapy within the 28–35 days after the drug treatment period); and 3) indeterminable (it was not possible to determine clinical assessment).
Statistical analysis
All patients who received at least one dose of moxifloxacin were evaluated for safety. The intention-to-treat (ITT) population included all the patients in the study who had received at least one dose of the study drug and whose essential data was complete (e.g. clinical evaluation at test of cure). The per-protocol (PP) population included patients matching the ITT criteria, who had a confirmed diagnosis of CAP and who had received study medication for a minimum of 48 h (in case of clinical failure) or 5 full days (in case of clinical cure).
Since the study aimed to compare moxifloxacin with standard treatment, reflecting the clinician's choice in the real world practice, it was powered as a two-arm comparison. The standard treatment arm offered three possible prerandomisation options but represented only a single arm for the purpose of randomisation and statistical analyses. The primary analysis was the clinical response at test of cure on the PP population. The two study groups were compared by using a one-sided 95% confidence interval (CI) for the difference in clinical success rates. If, and only if, the upper limit of this CI was <10%, moxifloxacin was proven to be at least as effective as the standard therapy.
The sample size was based on a conservative failure rate of 10% in the two arms, equivalence clinically relevant delta of 10%, and power of 90%. Taking into account a 15% increase in sample size to account for the multicentre design of the study, and assuming a validity rate of 80%, 269 patients were enrolled in each group resulting in a total of 538 patients.
The secondary effectiveness variables were analysed on ITT population. These included the clinical response at days 3–5 (on treatment) and days 28–35 (after the end of the treatment), the CAP symptom score (derived from the validation statistical analysis) 15, the SF-36 scores (calculated according to the recommended algorithms) 17, and healthcare utilisation data reported in units consumed without direct economic valuation.
As well as the two-arm comparisons of clinical and nonclinical outcomes, regimen-specific clinical outcomes within standard treatment were also described.
Results
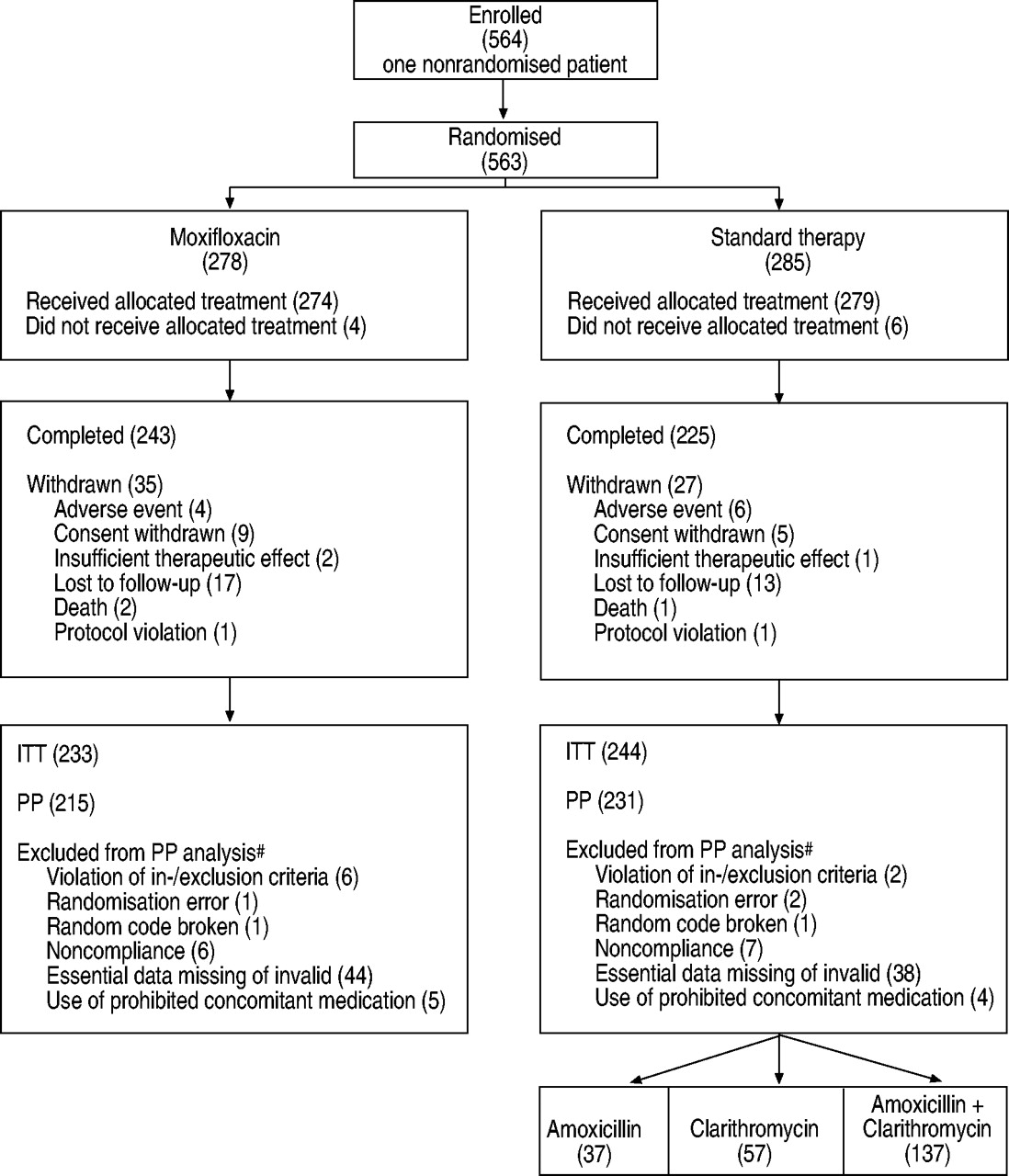
A total of 553 patients were randomised from 64 participating centres. A further 10 patients were invited to participate but declined before any drug was administered. Four-hundred and seventy-seven patients and 446 patients were included in the ITT and the PP analyses, respectively. The populations are depicted in figure 1⇓. In total, 13 countries were involved in this study (table 1⇓).

{kind=link}
Study population. Number of patients in parentheses. ITT: intention-to-treat; PP: per-protocol. #: patient may have more than one reason.
Country details (intention-to-treat population)
No between-group differences were found in the demographic characteristics, the medical history, the presenting signs and symptoms or the PSI (table 2⇓). Globally, the PSI was distributed into class I (178 patients, 37%), class II (108 patients, 23%) and class III (109 patients, 23%). Class IV and V, representing the most severe patients, comprised 75 (16%) and seven patients, respectively.
Patient demographics and medical history (intention-to-treat population)
Treatment compliance was similar in both groups, with 10 days as the mean length of study treatment duration. In the standard treatment arm, 143 of 244 patients received a combination of amoxicillin and clarithromycin. Monotherapy was received by 60 (24%) and 41 (17%) patients for clarithromycin and amoxicillin, respectively. Clinical presentation (88%), radiological findings (65%) and/or local susceptibility patterns (26%) were described as the principal reasons for antibiotic choice.
In the PP population, clinical cure at test of cure was achieved by 201 of 215 (93.5%) and 217 of 231 (93.9%) of the moxifloxacin and standard group patients, respectively (table 3⇓). This yielded a difference of -0.4% (95% CI −4.2–3.3%), demonstrating that moxifloxacin was as effective as the standard treatment. Follow-up at 28–35 days post-therapy showed a continued clinical cure of 95.3% (183 of 192) and 93.7% (207 of 221) for moxifloxacin and standard group patients, respectively (difference of -1.5%, 95% CI −2.2–5.2%). In the ITT population the results shown earlier were confirmed at all assessment points (table 3⇓). The rate of clinical cure was similar between the different regimens within the standard therapy arm, both in monotherapy (amoxicillin or clarithromycin), 94.1% (95 of 101) at test of cure and 91.8% (89 of 97) at 28–35 days follow-up, and in combination (amoxicillin+clarithromycin), 93.7% (134 of 143) at test of cure and 94.2% (129 of 137) at 28–35 days follow-up, respectively. Descriptive results were also expressed according to the PSI classification at study entry. These levels of clinical success rate were mainly consistent across the classes of PSI and within the different dosage regimen in the standard group (table 4⇓).
Clinical success rates at test of cure (TOC) and follow-up (per-protocol (PP) and intention-to-treat (ITT) populations)
Descriptive clinical success rates at test of cure (TOC) and follow-up according to the pneumonia severity index (PSI) (intention-to-treat population)
At baseline, 55–58% of enrolled patients had a temperature >38.5°C and no difference was found in the subsequent development of a temperature between the two groups. Likewise, the median of symptom scores regularly improved during the study period with no statistically significant differences between the groups (table 5⇓). The SF-36 questionnaire was completed by 96% of patients. The eight dimension scores as well as the PCS and MCS increased consistently at the end of the study period in comparison with at study entry, with no differences between treatment groups, indicating improvement in patient health status (table 6⇓).
Community-acquired pneumonia symptom questionnaire: completion and scores (intention-to-treat population)
Short-form 36: completion and domain scores (intention-to-treat population)
Likewise, concomitant medications, post-therapy antimicrobial treatments, hospitalisation patterns and requirements for additional therapeutic procedures were distributed similarly between the two groups (table 7⇓).
Consumption of healthcare resources (intention-to-treat population)
A total of 553 patients were included in the safety analysis. The incidence of adverse events was similar between moxifloxacin and standard treatment (48 and 54%, respectively; table 8⇓). The incidence of reported adverse events possibly related to the therapy was statistically lower with moxifloxacin than in the standard arm (20 versus 31% respectively, p=0.004). Possible drug-related adverse events are summarised in table 8⇓. Diarrhoea, the most common adverse event, was reported in 22 (8%) and 13 (5%) patients with standard treatment and moxifloxacin, respectively. Adverse events were reported more frequently among amoxicillin patients (37 of 53 (69.8%)) than with the two other dosage regimens, i.e. clarithromycin alone (38 of 71 (53.5%)) and in combination with amoxicillin (75 of 155 (48.4%)). This trend in adverse events was confirmed as probably drug-related: amoxicillin (22 of 51 (41.5%)), clarithromycin (20 of 71 (28.2%)) and bitherapy (44 of 155 (28.4%)). Diarrhoea and nausea were the most common reported events with amoxicillin, in eight (15.1%) and two (3.8%) patients, respectively. This was also the case for the combination of amoxicillin and clarithromycin: diarrhoea in 11 (7.1%) and nausea in two (1.3%) patients; the incidence rate in clarithromycin-treated patients was 4.2% (three patients) and 1.4% (one patient), respectively.
Safety evaluation: incidence of adverse events (AE) (safety population)
Overall, nine deaths were reported during the study, four in the moxifloxacin group (severe chronic obstructive pulmonary disease and suspected Clostridium difficile diarrhoea, pneumonia, sarcoidosis, heart failure) and five in the standard group (bronchial occlusion, multiorgan failure, cardiac and respiratory arrest, atypical pneumonia and lung cancer). Serious or life-threatening events were noted in 24 (9%) and 33 (12%) patients in the moxifloxacin and standard groups, respectively. Notably, none of the deaths or serious/life-threatening adverse events were attributed to or suggestive of arrhythmia or cardiac arrest. Overall, there were no significant differences in physical findings such as blood pressure or heart or respiration rates between treatment groups.
Discussion
In this study, 400 mg moxifloxacin orally o.d. proved to be as an effective first-line therapy as the standard mono- or combination therapy chosen on a per-patient basis by investigators. The present results suggest, according to recent ATS guidelines 14, that quinolones for nonhospitalised and hospitalised CAP patients may be given at the same level of efficacy as β‐lactams and macrolides. Moxifloxacin was significantly better tolerated than standard treatment with fewer drug-related adverse events.
This innovative outcomes study has several strengths that distinguish it from prior studies in CAP. Typically, phase III clinical trials are designed to achieve regulatory approval. The protocol-driven experimental setting maximises the internal validity of the test of a primary research hypothesis, but in doing so, the extrapolation of study results to conditions of real use is limited. With the rising importance of evidence-based medicine, this trade-off has been recognised and various methodological solutions proposed 18, 19. They range from statistical modelling of efficacy trial results, using epidemiological and economic data from the real world 20–22, to the design of pragmatic trials where protocol-driven constraints are relaxed and statistical analysis schemes modified in order to facilitate decision making rather than hypothesis testing 23, 24. The present study was designed to maintain a high degree of internal validity while maximising the generalisation of results. The internal validity of the study was ensured by a randomised, double-blinded, controlled study complying with good clinical practices. The external validity was enhanced by the fact that the choice of the comparator was left to the discretion of the investigator prior to randomisation. This feature allowed the optimisation of the choice of treatment based on the patient's presentation. The predefined choice of alternative antibiotics was carefully selected to represent current guidelines. Inclusion/exclusion criteria were left as broad as possible, so that the study population remained as similar as possible to CAP patients in the real world. Likewise, protocol-driven requests were limited as much as possible (no requested bacteriological, radiological follow-up). Finally, patient-reported outcomes measures have been included in the study. This was meant to reinforce the generalisation of study results from both a healthcare effectiveness and a patient's perspective 25–27.
Recent guidelines for management of CAP in adults were reflected by the choice of antibiotics selected in this study 10–14. Both monotherapy, a new macrolide or a β‐lactam (usually an aminopenicillin at a high dose) or combination of these drugs are recommended as first-line in nonhospitalised and hospitalised CAP patients. New fluoroquinolones in monotherapy, such as moxifloxacin, gatifloxacin or levofloxacin, have been suggested as first-line antibiotics in CAP. Several studies have compared new fluoroquinolones with amoxicillin 28–31 or with second- and third-generation cephalosporin 32–35 or macrolide, such as clarithromycin 36–41. However, no single study has embraced all of the therapeutically recognised options in CAP in an effectiveness analysis like that conducted in the present investigation. The present study was not designed to show equivalence with a single monotherapy regimen, although descriptive analyses per-product are consistent with previously published studies. Clinical success rates with moxifloxacin in CAP have ranged 90–94% in phase III studies against clarithromycin 36 and high-dose amoxicillin 28. The clinical cure rate of 93% with moxifloxacin was in keeping with previous studies; however, this study involved a range of illness severities comprising PSI I–V cases representing all severity stages of the disease. Again, according to recent ATS guidelines 14, this finding suggests that new quinolones in monotherapy are at the same level of efficacy as β‐lactams alone or in combination with macrolides for treatment of hospitalised and nonhospitalised CAP.
A strength of the present study was also its demonstration of equivalence to a potentially much stronger comparator arm, i.e. the free choice by clinician between two monotherapy and one combination therapy options. In fact, when asked about treatment choice in the present study, investigators in a vast majority (88% of patients were concerned) indicated that the clinical presentation of the patients was the major factor of the treatment decision. This attitude is consistent with the view of most clinicians, which takes into account the clinical status and the probable bacteriological diagnosis in the initiation of the proper therapeutic class choice for first-line treatment.
This innovative study design also provided some insight into the impact of CAP on quality of life and specific symptoms. The combined approach, using both a generic and a disease-specific instrument, was complementary in the evaluation of disease treatment and provided useful findings for any further research in CAP care assessment 15.
Moxifloxacin treatment was significantly better tolerated than standard regimens with fewer adverse events and premature discontinuations. The drug-related events seen in this study are usual in antimicrobial treatments, with a predominance of mild gastrointestinal upsets. The rate of these events compares favourably with previous clinical trial experiences seen with both regimens. Recent data on moxifloxacin showed nausea (8%) and diarrhoea (6%) as being the most frequent events 42, 43.
The mortality rate seen in this study was low (nine of 553). Indeed, most of the deaths were not attributable to studied treatment. There were insufficient cases in the more severe groups (PSI class V), where mortality rates are generally higher, to draw any conclusions. Thus, the safety profiles of the two treatment groups were generally unremarkable and revealed only typical adverse events associated with antimicrobials, such as diarrhoea and nausea. Overall, however, moxifloxacin-treated patients had a significantly lower incidence of adverse events.
To conclude, this innovative outcomes study supports the use of moxifloxacin as a first-line option for CAP. This treatment was as effective as an alternative of mono- or combination therapy, selected by a physician as the optimal treatment on a patient basis, and representing the maximal therapy option from main current guidelines. The safety profile of moxifloxacin was also favourable, with fewer drug-related adverse events in comparison to alternative standard treatment options.
These results of the Community-Acquired Pneumonia 2000 study may be the basis for future studies that could be in agreement with American Thoracic Society recommendations, advising the use of the most potent antipneumococcal antibiotics when the suspicion of resistances to Streptococcus pneumoniae is high, which may translate into differences in resistance rates and clinical success in the future.
Acknowledgments
The authors would like to gratefully acknowledge L.A. Mandell for advising on the study design and providing input to the manuscript. The authors would also like to thank all the study investigators in each of the following clinical sites. France: D. Benhamou, J-F. Muir, P. Petitpretz, R. Azarian, L. Bernabeu, P. Dumont, B. Castan, J. Vanche, L. de Saint Martin Pernot, J. Clavier, D. Yatim, D. Baron, A. Le Groumellec; Germany: K. Colberg, H. Common, R. Dichmann, C. Klein, J. Minnich, O. Gobrecht, G. Krause, K. Fehring, U. Harnest, R. Kraas, L. Leonhardt, S. Molitor, K. Kurz, W. Kreisel; Hungary: M. Szilasi, N. Dudas, I. Edes, A. Hainess, G. Nyarfas, T. Toth, V. Sarosi, Z. Baliko, L. Kovacs, F. Valikovics, J. Szegedi, S. Angyal, Z. Zilahi, A. Ferencz, S. Palinkasi, E. Walcz, J. Schlezak, M. Bisits, W. Younes; Israel: M. Moscovici, S. Oren, K. Riesenberg, F. Schlaeffer, A. Lalkin, R. Lang, M. Dan, D. Zeltser; Italy: G. Cervio, O. Filieri, A. Rossi, F. Marelli, G. Marchetti, A. Santolicandro, F. Tana, G. Meregalli, G. Losito, L. Petrozzi, D. Rizonelli, D. Sella; Norway: A. Bucher, A.B. Brandsaeter, P. Olsen, I.J. Hagen; Poland: J. Malolepszy, R. Dobek, A. Wolanczyk-Medrala, E. Liebhart, R. Suchnicka, G. Wojtas, T. Targowski,S. Gruska, M. Tazbirek, W. Pierzchala, M. Trzaska, M. Jarecki, A. Rydzewski, J. Gozdowska, M. Faber, T. Plusa, A. Kucharczyk, K Jahnz-Rozyk; Portugal: J Moita; South Africa: E. Seller, J. Crafford, M. Heystek, S. Oosthuizen, T. Fisher, Y. Botha, A. Engelbrecht, J. van Graan, L. Fourie, M. van Rooyen, S. Laloo, T. Kluÿts, W. Dannheimer, F. Ogundare, G. Ngombe, M. Siddiqui, J. Viljoen; Spain: A. Rosell, J. Morera, R. Pifarré, A. Torres, J. Angrill, M. Abel, C. Santana, J. Lope, J.C. Rodriguez, R. Esparza, V. Medina, J. Aspa, B. Nieto, O. Rajas, J. Fullana, C. Pellicer, M.J. Cremades, C. Vilarino, F. Iglesias, J.C. Barros, F. Del Campo, J.L. Perez, J. Frutos, M. Puyo; Sweden: M. Erntell, S.A. Hedström, B. Ljungberg, F. Killander, H. Norrgren, P. Akesson, B.O. Larsson, M. Whl, S. Jakobsson, B.O. Nillsson; Switzerland: J. Bartenstein; UK: M. Britton, P.A. Corris, S. O'Hickey, N.K. Harrison, O. Khair, M. Finnegan, D.P. Spence, T. Rogers, C. Connolly, A. Henderson.
- Received May 29, 2002.
- Accepted August 27, 2002.
- © ERS Journals Ltd
References









