





Abstract
The aim of this study was to determine mortality in patients with sleep apnoea/hypopnoea syndrome (SAHS) according to the treatments employed and comorbidity.
An historical cohort of patients with SAHS diagnosed at a university hospital between 1982 and 1992 and followed until 1996 was studied. From a total of 475 SAHS patients, 444 (94%), with a mean±sd apnoea/hypopnoea index at diagnosis of 55±27, were located and included in the study. SAHS treatments employed were: surgery (88), weight loss (134), continuous positive airway pressure (124) and 98 patients were not treated.
By the end of follow-up, 49 patients had died. According to Cox regression analysis, mortality in treated patients was lower than in those not treated, but higher in those with a history of severe chronic obstructive pulmonary disease. Mortality in nontreated patients compared with that of the general population, adjusted for age and sex, showed excessive mortality, which decreased in treated patients. Stratification by age showed a greater mortality rate ratio in patients <50 yrs. These findings were maintained when mortality from cardiovascular causes was compared.
In conclusion, a rise in mortality was found in nontreated sleep apnoea/hypopnoea syndrome patients compared with the general population, whereas mortality in those treated for sleep apnoea/hypopnoea syndrome did not differ significantly from that of the general population.
This study was financed in part by a grant from Agència d'Avaluació de Tecnologia Mèdica (Servei Català de la Salut).
Sleep apnoea/hypopnoea syndrome (SAHS), with a prevalence ∼3% of the general population 1, 2, constitutes a major public health problem. It has been associated with a lack of normal nocturnal decrease in blood pressure 3 and the presence of diurnal systemic arterial hypertension (AHT) 4, 5. Cross-sectional studies have related SAHS to coronary heart disease 6, 7 and stroke 8. Sleep disruption and daytime sleepiness seen in SAHS patients also give rise to an increase in road accidents 9. Other complications such as cor pulmonale 10 or respiratory failure 11 occur in some patients.
It has been postulated that the above-mentioned complications could account for the increased mortality observed in a reduced number of studies in clinical populations 12–14. The availability of nasal continuous positive airway pressure (nCPAP) since the early 1980s 15, which is effective in improving symptoms and limiting apnoea/hypopnoea episodes 16, implies that it is not ethical to conduct long-term studies that involve random assignment of symptomatic patients to groups without treatment. The introduction of nCPAP into the current authors' centre in 1988 afforded a historical cohort of patients with severe SAHS, treated or not, in whom mortality in the long term was evaluated according to the treatment applied and comorbidity present at diagnosis. Furthermore, this mortality was compared with that of the general population used as an external control group.
Patients and methods
Cohort recruitment
All patients residing in Catalonia, Spain and diagnosed with SAHS between January 1982 and December 1992, in an out-patient department for sleep-disordered breathing of a university hospital (belonging to the National Health System (NHS), with universal coverage), were evaluated. The inclusion period for nontreated patients was considered closed in December 1987, since the advent of nCPAP in 1988 modified the characteristics of patients who remained untreated after this date. Patients <16 yrs, those treated by tracheostomy, or who presented hypothyroidism, acromegaly or malformations of the base of the skull were excluded from the study.
Diagnosis
Patients were referred to the clinic for suspected SAHS. They were assessed by a single physician (A. Roca); clinical history was recorded systematically and, if considered indicated, nocturnal polysomnography (PSG) was performed. The PSG collected the recordings of the electroencephalogram, electro-oculogram and chin electromyogram, electrocardiogram, oro-nasal airflow by thermistor and thoraco-abdominal movements. Arterial oxygen saturation (Sa,O2) throughout the night was monitored by an oxymeter, initially by an ear sensor (47201A; Hewlett Packard, Waltham, MA, USA) and later by digital pulsioximetry (Pulsox 7; Minolta, Schaffhausen, Switzerland). Sleep stages were interpreted according to the usually accepted criteria 17: an apnoea was defined as the absence of airflow for at least 10 s; and a hypopnoea was considered at any reduction ≥50% in oro-nasal flow, of at least 10 s duration, accompanied by a decrease in Sa,O2. Finally, the apnoea/hypopnoea index (AHI) was defined as the number of apnoeas or hypopnoeas per hour of sleep. An AHI ≥10 was considered diagnostic of SAHS.
Treatment
When the diagnosis of SAHS was established, and according to the PSG results, subjective symptoms and comorbidity, patients were offered the treatments available. 1) Hygienic dietary measures, consisting of a recommended diet of 1,000–1,500 kilocalories·day−1, increased physical exercise, sleeping in the lateral decubitus position and avoidance of sedatives and alcohol. These measures, recommended in all patients, constituted the only treatment attempt in mild patients or those who rejected other treatments. Patients who received this treatment alone were considered as treated by diet or nontreated according to whether during the year following diagnosis they succeeded in losing 10% of their weight or not. 2) Uvulopalatopharyngoplastic surgery, performed in the Otorhinolaryngology Dept. The effects of diet or surgery were evaluated in a second PSG usually performed when a 10% weight loss had been achieved or at 6 months postsurgery. 3) nCPAP, available at the current authors' centre since 1988, which has become the treatment of choice for moderate-to-severe SAHS 18. In patients for whom this treatment was considered to be indicated, a second nocturnal PSG was performed to determine the pressure level required to suppress apnoeas, hypopnoeas and snoring. If Sa,O2 <90% persisted when effective pressures were reached, oxygen was added to the nCPAP mask at a flow required to achieve saturations >90%. The apparatus was provided and its technical servicing carried out in the patients' home by the supplying company, with the costs covered by the NHS. Sub<1?show=[fo]>jective compliance reported by the patient at the latest visit was recorded.
Follow-up
Patients were included from the time of SAHS diagnosis and the follow-up was closed in December 1996. In patients who abandoned the initial treatment before this date, follow-up was ended at that time and the information generated up to that point was used. Clinical follow-up consisted of medical appointments at 1, 3 and 6 months postdiagnosis, and every 6 months thereafter.
Information on the follow-up period was obtained by personal interview in the out-patient department, telephone or mail. If a patient had died, the next of kin was contacted. In order to obtain information on all deceased patients or those not located, data from the Mortality Registry of Catalonia (MRC; Servei d'Informació i Estudis, Direcció General de Recursos Sanitaris, Dept de Sanitat i Seguretat Social) for 1982–1996 was used, which provided the basic causes of death classified into four groups: 1) cardiovascular causes (International Classification of Diseases (ICD)-9 codes 19 390–459, 798); 2) accidents (ICD-9 codes 800–869, 880–901, 904–906, 910–921, 924–926, 928); 3) respiratory causes (ICD-9 codes 460–519, 786); and 4) others. For labelling of the causes of death, those stated in the clinical history or reported by the relative were considered first, and causes reported by the MRC were considered only in cases not located by other routes. Patients not located by any of the cited routes were not considered in later analyses. The selection and location of patients are depicted in figure 1⇓.

Selection of sleep apnoea/hypopnoea syndrome (SAHS) patient cohort. PSG: polysomnography; AHI: apnoea/hypopnoea index. #: hypothyroidism (n=10), acromegaly (n=4) and Arnold-Chiari malformation (n=1); ¶: the treatments received by nonlocated patients were: surgery (n=5), weight loss (n=18), continuous positive airway pressure (n=3) and nontreated (n=5).
Analysis
Descriptive and bivariate statistical analysis was performed in the first phase. Independent variables analysed in this phase were: age, sex, body mass index (BMI), alcohol consumption and smoking history, AHT, coronary heart disease, stroke, diabetes mellitus, dyslipaemia, chronic obstructive pulmonary disease (COPD), AHI, SAHS treatment and compliance with nCPAP treatment. Tests used were t-test or analysis of variance for continuous variables and Chi-squared for qualitative variables. When the application conditions were not met, Mann-Whitney, Kruskal-Wallis or Fisher's exact test, respectively, were used. Results were expressed as mean±sd for quantitative variables and as percentage for qualitative variables. The Kaplan-Meier method of survival analysis was applied for calculation of survival rates.
In the multivariate phase, the Cox proportional risk model was used to determine the predictive variables of mortality 20. A series of variables of particular interest was selected or “forced” as fixed in the model, and the rest were added one by one and their effect on the predetermined model was evaluated. The independent variables for this phase were selected in accordance with the bivariate analysis (p<0.10) or for being considered biologically plausible. Results of Cox regression were expressed as hazard ratio (95% confidence interval (CI)). Patients who left the initial treatment cohort were considered censored at the time of withdrawal. SAHS-related mortality was considered to be that due to cardiovascular or respiratory causes or accidents. Patients who died of other causes were treated as censored in the analysis of SAHS-related mortality.
Mortality rates of the cohort were compared with those of the general population of Catalonia from 1982 to 1996, as an external control group. For this, the MRC provided the causes of death in the cited period and the population in the 1991 census of Catalonia was considered 21. Specific mortality rates were calculated, according to the cause of death, by age and sex, using Poisson regression and the person-year method 20, and compared with the number of deaths observed. The linear trend in the risk was evaluated for the age variable. Taking into account the effect of age on mortality, this analysis underlines the real prognostic impact of age.
Two-tailed p-values of <0.05 were considered significant.
Results
Baseline characteristics
The population studied consisted of 444 patients with SAHS, of whom 389 were males (88%), age 53±10 yrs, BMI 32±5 kg·m−2 and AHI at diagnosis 55±27. The patients were referred for consultation by a general practitioner (23%), ear, nose and throat specialist (29%), pneumologist (26%) or other specialists (22%). Many of the patients had associated comorbidity at diagnosis of SAHS: AHT (43%), coronary heart disease (7%), stroke (2%), diabetes mellitus (8%), dyslipaemia (19%) and COPD (27%). No significant differences were observed when all the previously cited characteristics in patients studied were compared with those of nonlocated patients (n=31). Eighty-eight patients were treated by surgery, 134 by diet and 124 by nCPAP, while 98 received no treatment. The baseline characteristics, grouped according to treatment cohort, are shown in table 1⇓. The surgically treated group were younger and had lower BMI and history of AHT and COPD than the other treatment groups.
Baseline characteristics of sleep apnoea/hypopnoea syndrome patients according to treatment group
Follow-up
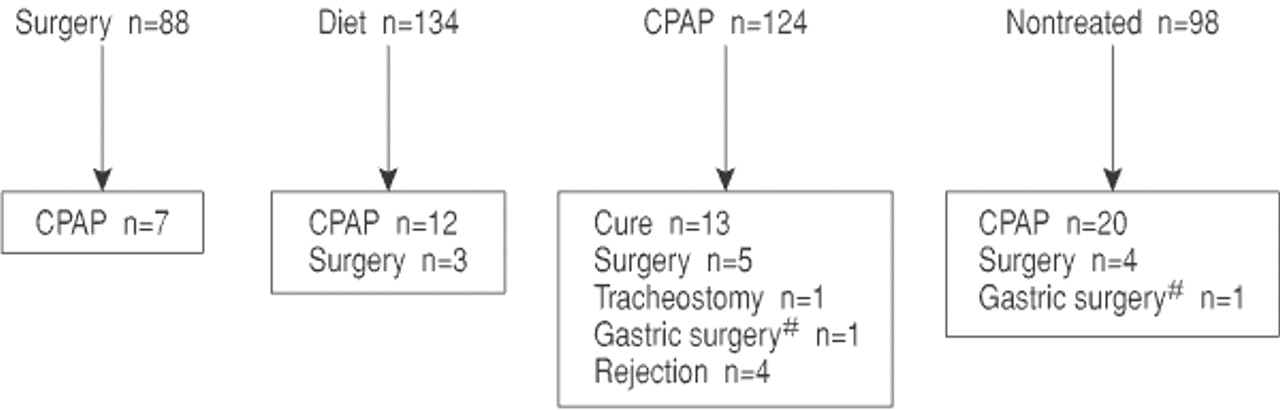
Mean follow-up of the different cohorts was 7.1±2.0 yrs in surgery, 7.2±2.4 diet, 5.2±1.9 nCPAP and 7.2±3.1 in those nontreated. Control PSG was performed in 75 patients treated with surgery (85% of those belonging to this cohort), with AHI of 22±22 (AHI at diagnosis 58±26; p<0.001); 29 patients (33% of those surgically treated) were cured of SAHS (AHI <10 on control PSG). Similarly, a second PSG was performed approximately 1 yr after diagnosis in 112 treated with diet (84%; BMI 27±3 versus 32±4 kg·m−2 at diagnosis; p<0.001) with AHI 24±26 (54±27 at diagnosis; p<0.001); cure of SAHS was recorded in 49 patients (37%). At the end of the follow-up, BMI in those treated with surgery or diet was 27±3 and 30±4 kg·m−2, respectively. Subjective compliance with nCPAP treatment was 6.9±1.7 h·day−1; 85% of patients reported compliance of at least 6 h. The follow-up was closed before December 1996 owing to change of the initial treatment cohort in 71 out of the 444 patients (fig. 2⇓).
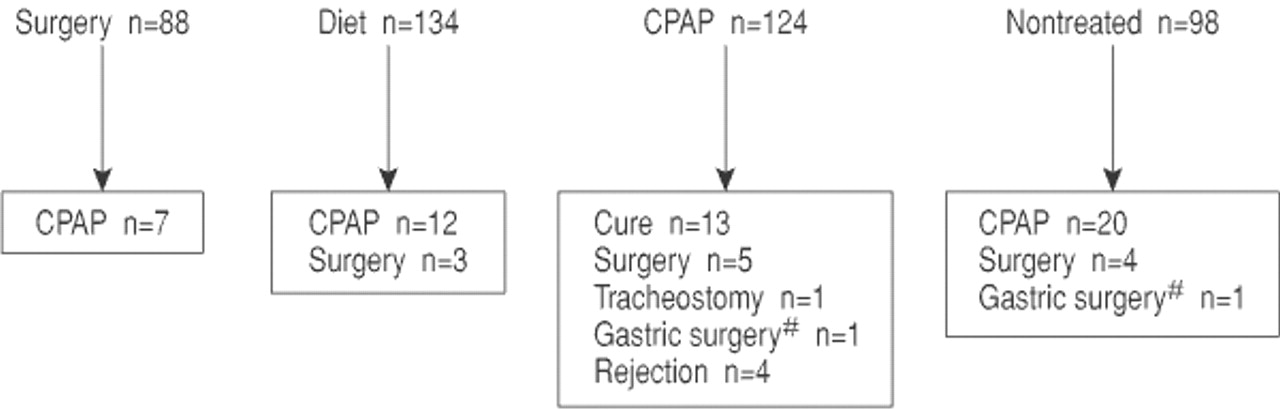
Patients leaving their original treatment cohort before the end of follow-up. CPAP: continuous positive airway pressure. #: gastric surgery as treatment for obesity.
Mortality
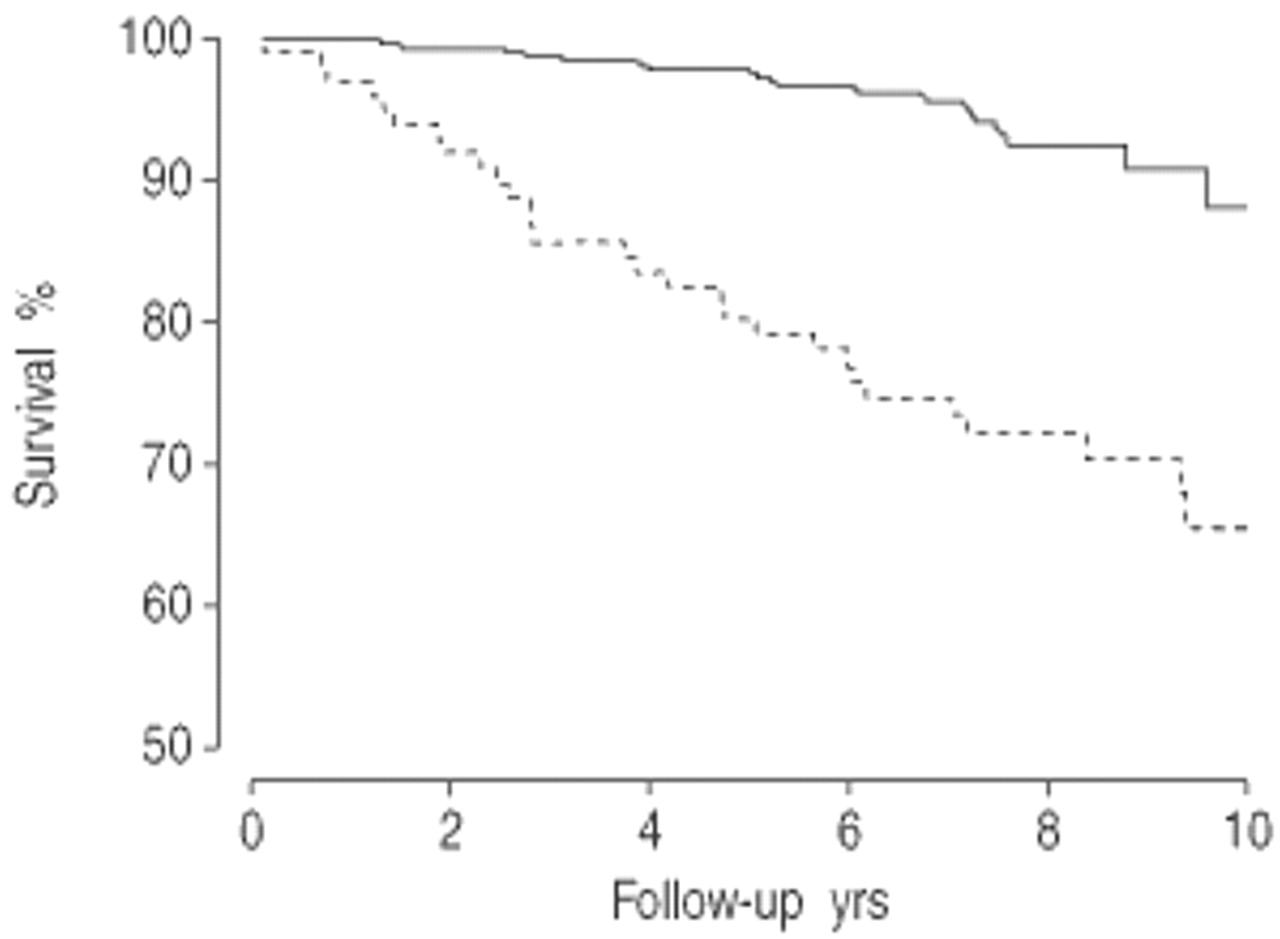
By the end of follow-up, 49 patients had died (11%). Their mean age at the time of diagnosis was 55±11 yrs, 42 were males, BMI 33±7 kg·m−2 and AHI 53±30. The causes of death are detailed in table 2⇓. Survival rate at 5 yrs for nontreated patients was 0.80 (CI 95% 0.72–0.88), while in those treated with surgery, diet or nCPAP it was 1, 0.97 (0.94–0.99) and 0.97 (0.94–1.00), respectively. Figure 3⇓ depicts the Kaplan-Meier survival curve for patients treated or nontreated.
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier estimate of the survival curve for sleep apnoea/hypopnoea syndrome patients, according to whether they were treated (—) or nontreated (---).
Causes of death in sleep apnoea/hypopnoea syndrome patients, grouped according to treatment
Multivariate analysis by Cox regression, to find predictive factors of overall and SAHS-related mortality, showed a reduction with the different treatments applied, but an increase with a history of severe COPD (tables 3 and 4⇓⇓). For instance, nCPAP treatment (hazard ratio 0.23, CI 95% 0.09–0.58) led to a reduction in mortality compared with nontreated patients of at least 40%, when the upper limit of the 95% CI was considered. These results were maintained even when coronary heart disease, smoking and COPD were taken into account. A trend towards increased SAHS-related mortality was also observed with BMI >35 kg·m−2. Sex, AHI and AHT history did not influence the adjusted models. Even when AHI was analysed exclusively in nontreated SAHS patients, no relationship was found with mortality (p>0.20).
Cox regression: overall mortality
Cox regression: sleep apnoea/hypopnoea syndrome-related mortality
The overall mortality rates observed in nontreated SAHS patients compared with those expected in the general population, adjusted for age and sex, showed excessive mortality (table 5⇓), both in males (rate ratio (RR) 4.58, CI 95% 3.09–6.78) and females (RR 8.07, CI 95% 2.09–31.19). Stratification by ages performed only in males, given the scant number of deceased females, reflected an increase in mortality RR in the youngest patients that decreased progressively with age, although it remained high in those >60 yrs. In contrast, when treated SAHS patients were analysed, overall mortality rates decreased and were somewhat higher compared with those calculated for the general population, though without reaching a statistically significant difference (RR 1.29, CI 95% 0.80–2.07 in males; RR 1.11, CI 95% 0.16–7.70 in females). These trends were maintained when SAHS-related (data not shown) and cardiovascular mortality rates (table 6⇓) were compared.
Observed and expected overall mortality, adjusted for age and sex, rate ratio (RR) and 95% confidence interval (CI)
Observed and expected cardiovascular mortality, adjusted for age and sex, rate ratio (RR) and 95% confidence interval (CI)
Discussion
The present study, conducted in a clinical severe SAHS cohort, showed that patients with untreated SAHS presented higher mortality than the general population, adjusted for age and sex. Given the wide CI shown by the mortality rate ratios, the lower limit of these intervals can be considered the minimum risk consistent with the present data. Thus, the relative risk of mortality presented by patients with nontreated SAHS would be at least in the order of 2–3 times that of the general population. As in previous works, the excess of mortality detected was basically due to cardiovascular 13, 14, 22, 23 and respiratory 22 causes, which have been related to SAHS. Conversely, when SAHS patients were treated by surgery, weight loss or nCPAP, mortality was similar to that of the general population. This lower mortality observed in patients with treated SAHS persisted once other possible confounders had been adjusted by Cox regression.
Certain considerations should be borne in mind regarding the design of the present study. First, there may have been a selection bias; nevertheless, the distribution of age at diagnosis (53±10 yrs) and sex (88% males), similar to that of other clinical cohorts reported in the literature, supports the representative nature of the present cohort. Secondly, the treatments were not randomly distributed among the patients. This may have given rise to differences among the treatment groups, such as the lower comorbidity registered in those treated by surgery. Although the use of Cox regression tended to reduce this bias, it may not have eliminated it completely. Thirdly, a further possible source of bias arose from the 71 patients who, throughout the follow-up, changed their original treatment cohort and were considered censored thereafter. However, the abandonments principally affected the group of nontreated patients. Thus, it was to be expected that the present analysis in fact tended to underestimate the mortality of the nontreated cohort. Fourthly, the nontreated patients in this study presented more severe SAHS than patients not treated since the advent of nCPAP, who were not included in this analysis. The evolution of these milder SAHS is an objective of large prospective studies currently underway 1, 24.
The present results concur with those of previous studies in which mortality in SAHS patients treated with nCPAP was lower than that reported in nontreated patients 12 and similar to that of the general population 22, 23. The application of nCPAP suppresses apnoeas, and subsequently eliminates recurrent episodes of hypoxaemia and the cardiovascular consequences associated with them 25. In the long term, this could contribute to reducing mortality, which in fact occurred in this study, although the nCPAP users may not have been as adherent as their subjective reports indicated 26. However, the lower mortality registered in the present study in SAHS patients treated with diet or surgery had not been found previously 12, 13. In the control PSG, performed in 84% of these patients, a significant reduction in sleep-disordered breathing and cure of SAHS was observed in 35%, which could have had a similar influence to that of treatment with nCPAP. It should be emphasised that patients who received both treatments maintained a weight lower than that at diagnosis, which has been proved to be an important factor in maintaining the benefits achieved with them 27, 28 and which has been related to the periodic clinical follow-up 28. Furthermore, the periodic clinical follow-up of these patients permitted the detection of therapeutic failures and establishment of alternative treatment that may have favoured the results of treatment with diet or surgery.
Of the characteristics present at diagnosis of SAHS, age, history of severe COPD, smoking and obesity proved to have a significant impact on mortality of the present cohort. As reported in previous studies 12, 14, in the present study the RR of overall and cardiovascular mortality in untreated male SAHS patients increased in the youngest, and was higher in those <50 yrs of age. The poor prognosis of the SAHS-COPD association had previously been reported, even in patients treated with nCPAP 22, 23. The greater hypoxaemia present in patients with COPD and SAHS 29 or the incidence of severe respiratory complications 11 could be responsible for the mortality in these patients. Furthermore, the trend of BMI to increase SAHS-related mortality, together with the benefits reported with diet treatment, emphasises the importance of weight reduction as a complementary measure in the management of these patients.
By contrast, AHI at diagnosis, AHT and sex did not influence survival in the present study. In the case of AHI, an index usually employed to quantify SAHS severity and related in previous studies to mortality in these patients 12, 14, the fact of its being homogeneously raised in the cohort in this study and its modification by the treatments applied could have masked its importance. In the case of AHT, despite the existence of epidemiological studies that point to SAHS as a causal factor of diurnal AHT 4, 5, study of the adverse effect of blood pressure in these patients may require analysis of its nocturnal behaviour 3, 30. Finally, although particular characteristics of SAHS have been described in females 31 and a preliminary study pointed to a possible increase in mortality 32, no differences were found according to sex.
In conclusion, the authors found an increase in mortality in nontreated sleep apnoea/hypopnoea syndrome patients compared with the general population, with patients under 50 being at greatest risk. Furthermore, a decrease in this mortality was observed in patients receiving sleep apnoea/hypopnoea syndrome treatment. These results underline the need for early detection and treatment of sleep apnoea/hypopnoea syndrome and its subsequent clinical follow-up which permits detection of therapeutic failures.
Acknowledgments
The authors would like to thank Mortality Registry of Catalonia for providing mortality data, Laboratori de Bioestadística i Epidemiologia, Universitat Autonoma de Barcelona, for advice in the analysis and C. O'Hara for help with the English translation.
- Received January 4, 2002.
- Accepted July 12, 2002.
- © ERS Journals Ltd
References









