





Abstract
Small airway disease in infants is characterised by abnormal lung volume and uneven ventilation distribution. An inert tracer gas washin/washout technique using a pulsed ultrasonic flow meter is presented to measure functional residual capacity (FRC) and ventilation distribution in spontaneously breathing and unsedated infants.
With a pulsed ultrasound sent through the main stream of the flow meter, flow, volume and MM of the breathing gas can be calculated. Sulphur hexafluoride was used as a tracer gas. In a mechanical lung model (volume range 53–188 mL) and in 12 healthy infants (aged 38.3±9.2 days; mean±sd) accuracy and reproducibility of the technique was assessed. Indices of ventilation distribution such as alveolar-based mean dilution number (AMDN) and pulmonary clearance delay (PCD) were calculated.
Mean error of volume measurement in the lung model was 0.58% (coefficient of variance (CV) 1.3%). FRC was in the low predicted range for normal infants (18.0±2.0 mL·kg−1) and highly reproducible (5.5±1.7% intra-subject CV). AMDN was 1.63±0.15 and PCD was 52.9±11.1%.
Measurement of functional residual capacity and ventilation distribution using a sulphur hexafluoride washin/washout and an ultrasonic flow meter proved to be highly accurate and reproducible in a lung model and in healthy, spontaneously breathing and unsedated infants.
- functional residual capacity
- infant lung function
- lung model
- ultrasonic flow meter
- ventilation distribution
This study was supported by the Swiss National Foundation (SCORE 32-51974.97), Australian National Health and Medical Research Council, Swiss CF Foundation, AstraZeneca (Switzerland)
Infants with small airways disease such as wheezing disorders, cystic fibrosis and chronic lung disease have hyperinflated lungs and ventilation inhomogeneities 1, 2. In infants it is difficult to target small airways function. The rapid thoracic compression technique and whole-body plethysmography have been proposed to provide a measure of small airways function, however these methods have limited capacity, require sedation and might be not suitable for larger epidemiological studies.
To quantify the degree of functional abnormalities of the lung and to study the therapeutic effect of inhaled bronchodilators or topical anti-inflammatory drugs, an accurate and easy-to-use technique to measure lung volume and ventilation distribution in infants is necessary. This can be achieved by multiple breath gas washout techniques. Gas dilution techniques determine functional residual capacity (FRC) by measuring areas of the lung that readily communicate with the central airways during tidal breathing. Two gas dilution techniques frequently used are closed helium (He) dilution and open-circuit multiple-breath nitrogen washout (MBNW). Although MBNW can be performed easily, the considerable change in gas viscosity during the washout manoeuvre significantly affects the accuracy of the gas flow (V′) measurement by pneumotachography 3, 4. The He dilution technique avoids this latter problem, but is based on a closed circuit and leaks in the measuring system reduce its accuracy 5. In addition the He technique has a long time constant and cannot be used to assess gas mixing. Sulphur-hexafluoride (SF6) washout is a potentially suitable technique for children, including those who require near 100% oxygen (O2) to maintain normal haemoglobin saturation 6, 7.
The aim of this study was to develop a simple technique able to measure lung volume (FRC) and ventilation inhomogeneities in spontaneously breathing infants without altering the infant's breathing and reducing problems due to leak. The aim was to validate the accuracy and feasibility of a new SF6 washin/washout technique in a mechanical lung model and in unsedated healthy infants.
Material and methods
Subjects
Twelve healthy infants (four female, eight male), aged 38.3±9.2 days (mean±sd) were measured. The infants had no reported respiratory events prior to study enrolment, were born at term, and had no parental history of asthma or smoking. The study was approved by the ethics committee of the University Children's Hospital, Berne and written parental informed consent was obtained before measurements.
Study design
The SF6 washin/washout technique was initially evaluated in a mechanical lung model and subsequently tested in nonsedated spontaneously breathing, healthy infants. Measured FRC and indices of ventilation distribution were compared to reported results in the literature.
Sulphur hexafluoride multiple-breath washin/washout system
FRC and ventilation indices were measured with a multiple-breath washin/washout technique using SF6 as a tracer gas. The system used was adapted from a previous study of FRC in ventilated children and animals 8. The system (fig. 1⇓) included a computer, a constant bypass flow (8–12 L·min−1), an ultrasonic flow meter (Spiroson® Scientific; ECO Medics AG, Dürnten, Switzerland) and an airtight face mask. A pressure driven blender, controlled by the computer was used to switch from room air to a gas mixture containing room air and 4% SF6. Inspiratory and expiratory V′ were measured with the ultrasonic flow meter and integrated to calculate inspired and expired volumes (V). Flow is determined by measuring the transit time of a pulsed ultrasound travelling through the streaming medium. The sound is either accelerated or de-accelerated by the movement of the medium, causing, for a fixed distance across the medium, a decrease in the downstream and an increase in the upstream transit time. This change in transit time is related to gas velocity. The molar mass (MM in g·mol−1) of the gas in the main stream of the flow meter can be computed from the transit time with high accuracy and its value is directly proportional to the density of the medium. The MM can be assessed with the Spiroson® ultrasonic flow meter over the range of molar mass of 20–45 g·mol−1 with a precision of 0.01 g·mol−1. Hence using the formula:  the MM can be calculated (where φ is the gas density, MM is the molar mass, p is the pressure, R is the gas constant and T is the temperature). However the precise temperature along the sound transmission path must be determined. Due to the complexity of the determination of the temperature along the sound transmission path and because minor changes in temperature are present during tidal breathing, the changes of temperature along the sound path can be simulated using a temperature model. The temperature model uses the measured flow, instrumental dead space and the preset temperature (at body temperature and ambient pressure, and saturated with water vapour (BTPS) correction parameters) of the inspiratory and expiratory gas to calculate the temperature changes along the sound transmission path. The composition of the inspiratory gas differs from the expiratory due to pulmonary gas exchange. Normally the inspiratory gas constitutes 21% O2 and 79% nitrogen (N2) resulting in a MM of 28.85 g·mol−1. During expiration the MM is slightly higher due to the presence of carbon dioxide (CO2), the MM of which is ∼29.09 g·mol−1. To take account of these effects of temperature and gas composition on the MM signal, the authors subtracted from the measured MM during washin and washout, the baseline MM which was obtained during the corresponding phase of tidal breathing prior to the SF6 washin (assuming that during a measurement the breathing conditions remain constant). The difference between measured and baseline MM is called ΔMM. The washin or washout curve of SF6 was described using ΔMM. To obtain the instantaneous SF6 fraction at every moment during washin and washout, ΔMM was divided by the MM of SF6 (146.05 g·mol−1). A two-point calibration of the MM signal was performed using room air and 4% SF6.
the MM can be calculated (where φ is the gas density, MM is the molar mass, p is the pressure, R is the gas constant and T is the temperature). However the precise temperature along the sound transmission path must be determined. Due to the complexity of the determination of the temperature along the sound transmission path and because minor changes in temperature are present during tidal breathing, the changes of temperature along the sound path can be simulated using a temperature model. The temperature model uses the measured flow, instrumental dead space and the preset temperature (at body temperature and ambient pressure, and saturated with water vapour (BTPS) correction parameters) of the inspiratory and expiratory gas to calculate the temperature changes along the sound transmission path. The composition of the inspiratory gas differs from the expiratory due to pulmonary gas exchange. Normally the inspiratory gas constitutes 21% O2 and 79% nitrogen (N2) resulting in a MM of 28.85 g·mol−1. During expiration the MM is slightly higher due to the presence of carbon dioxide (CO2), the MM of which is ∼29.09 g·mol−1. To take account of these effects of temperature and gas composition on the MM signal, the authors subtracted from the measured MM during washin and washout, the baseline MM which was obtained during the corresponding phase of tidal breathing prior to the SF6 washin (assuming that during a measurement the breathing conditions remain constant). The difference between measured and baseline MM is called ΔMM. The washin or washout curve of SF6 was described using ΔMM. To obtain the instantaneous SF6 fraction at every moment during washin and washout, ΔMM was divided by the MM of SF6 (146.05 g·mol−1). A two-point calibration of the MM signal was performed using room air and 4% SF6.

Configuration of the sulphur hexafluoride (SF6) washin/washout equipment.
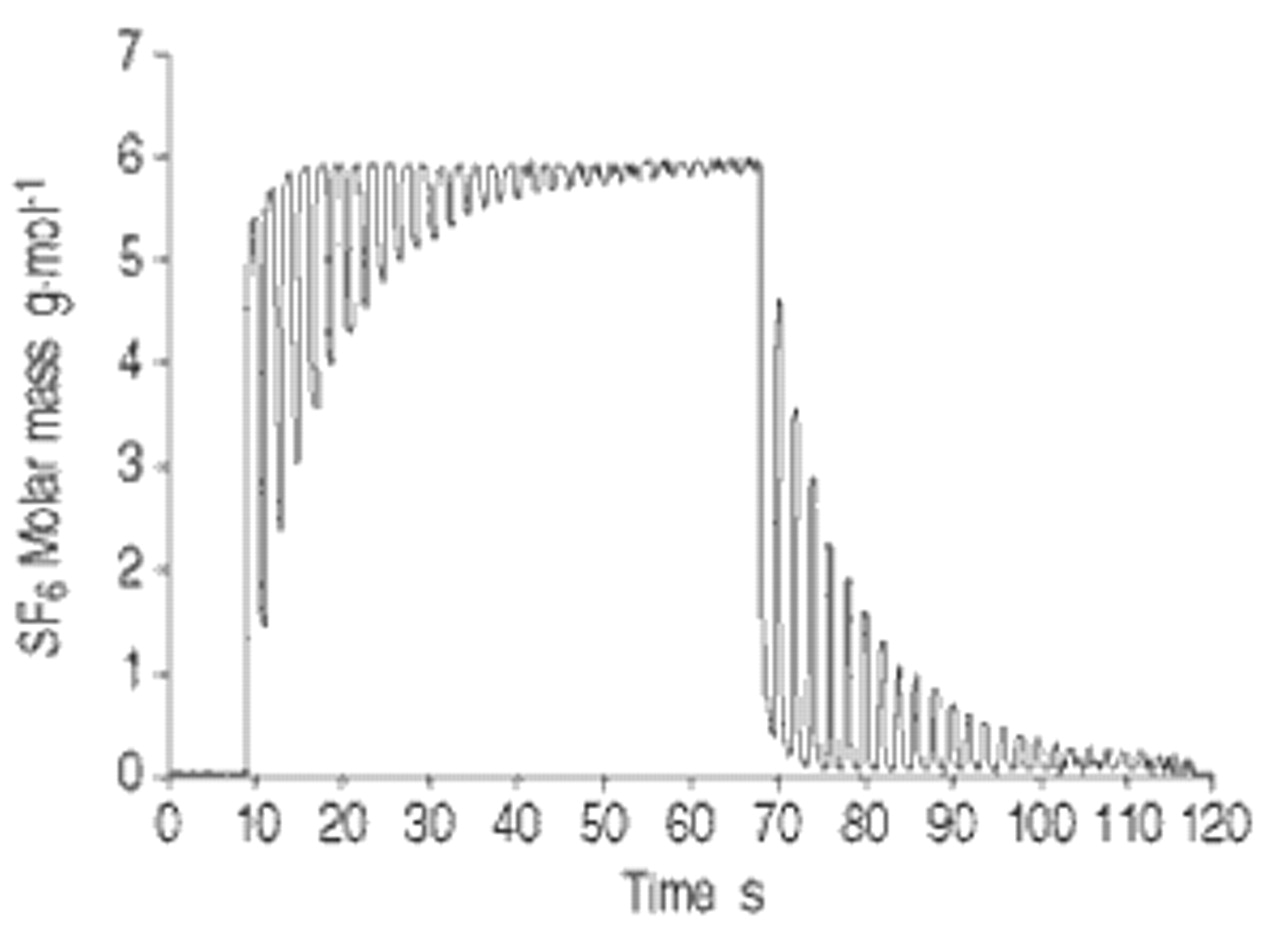
An infant ultrasonic flow meter (dead space of 1.3 mL) was used for measurements in infants. A medium ultrasonic flow meter (dead space of 3.2 mL) with a larger inner diameter was used in the lung model due to the higher flow encountered when the model was ventilated at a rate of 60 min−1 and with a tidal volume (VT) of 80 mL. The flow meter was calibrated with a high precision calibration syringe (Hans Rudolph, 5510 Series; Gambro AG, Hünebach, Switzerland) and considered to be calibrated adequately if integrated volume was within 1% of 100 mL. The authors ensured the flow head was airtight up to a pressure of 20 cmH2O. The MM of the in- and exhalation gas was measured with the ultrasonic flow meter (fig. 2⇓). The signals of V′ and MM were acquired by the Spiroson control unit, digitised and sampled at a rate of 200 Hz. The digitised signals were processed and stored on the computer.
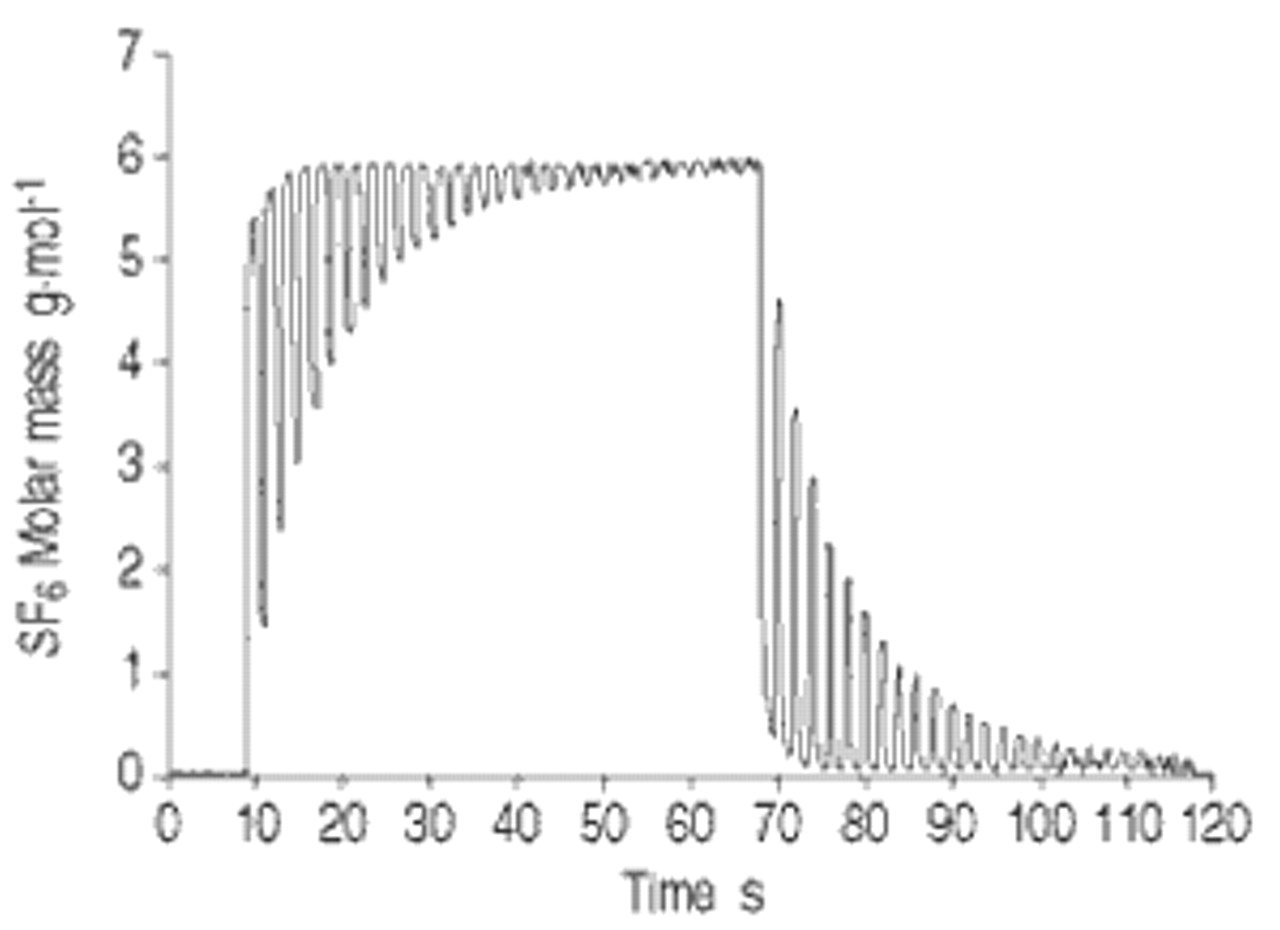
A typical washin and washout of sulphur hexafluoride (SF6). Washout of SF6 is initiated when end expiratory SF6 concentration is constant.
Calculation of functional residual capacity and indices of ventilation distribution
The FRC of washout was obtained by dividing the measured expired SF6 volume with the end-tidal SF6 concentration before washout. The initial SF6 volume within the flow meter and the connectors was subtracted from the total of the exhaled SF6 volume. The FRC of the washin was determined similarly using the mathematical mirror image of the washout signal. FRC was measured in duplicate for each washin/washout. In each infant at least three SF6 washin/washouts were performed and the six FRC values were calculated. V′, V and FRC were corrected to BTPS conditions. The calculation of the washout indices was limited to the most frequently reported and calculated as described by the original authors. The lung clearance index (LCI) is the number of volume turnovers required to reduce end-tidal SF6 concentration to one-fortieth of the tracer concentration at the start of the washin/washout 9. The alveolar-based mean dilution number (AMDN) is the ratio between the first and the zero moments of the washout curve. The number of volume turnovers was calculated using the cumulative expired alveolar volume (VT minus dead space volume) 10. The mean dilution number (MDN) was calculated similarly to AMDN but the cumulative expired alveolar volume is not corrected for Fowler dead space 3. The pulmonary clearance delay (PCD) is defined as 100×(actual average time a tracer gas remains in the lungs – the ideal time)/the ideal time 9. The mixing ratio is the ratio between the observed and the ideal number of breaths required reducing the end-tidal tracer gas concentration to one-fortieth of the concentration at the start of the washout 11. A low value of any index indicates even ventilation.
The Fowler dead space (VD) was obtained from the first three expirations during washout 9. VD was defined as the volume expired when the SF6 concentration reached 50% of the end-tidal SF6 concentration of that breath. At least four VT prior to and following the SF6 washin were recorded to evaluate if the breathing pattern changes during the SF6 washin.
FRC and ventilation indices were calculated using the software provided with the ultrasonic flow meter and the authors' own algorithms written in LabView 5.0.
Measurements in infants
SF6 washin/washout was performed during regular sleep without sedation and in supine position. The transcutaneous haemoglobin saturation was continuously monitored during the measurement (Ohmeda 3800 Pulse Oximeter, Helsinki, Finland). A face mask, sealed around the nose and mouth to ensure an airtight fit, was carefully manipulated into place for the measurements. The face mask had an effective dead space of 5 mL (measured by water displacement). At least three washin/washout of SF6 were performed in every infant.
Lung model
The lung model has been described previously 12. Shortly summarised, a linear pump (Scireq Inc., Montreal, Canada) with a precision of 0.5% (full stroke), enabling the simulation of tidal and forced flow patterns was used 13. The VT can be reproduced with a precision of ±1% at frequencies between 10–120 beats per minute (bpm). The linear pump was connected to a series of known volumes (55, 60, 80, 90, 95, 110, 115, 120, 125, 130, 135, 140 and 185 mL). In the present experiment the lung model was washed out using breathing frequencies of 20, 40 and 60 bpm and VT of 24, 34, 40, 49, 56, 68, 74 and 79 mL. The ratio of VT to FRC was chosen to be between 0.4–0.6. The volumes were built of copper and filled with copper wool in order to maximise and homogenise the heat dissipation. The exact volumes of these elements were calculated from water displacement as well as from their physical dimensions, in which both copper wool and connector volumes were taken into account. A minimal leak of the lung model was observed using a pressure up to 20 cmH2O. This leak was dependent on pressure as well as frequency and VT. To quantify the effect of the leak on the accuracy of FRC measurement the following set-up was used: the lung model was flushed with a mixture of room air 4% SF6. An empty rubber balloon was attached to the distal end of the ultrasonic flow meter. The linear pump then ventilated the lung model at different frequencies (20 to 60 bpm) and the VT were adjusted to have a VT/FRC ratio of 0.4 and 0.6. The empty highly compliant rubber balloon was needed to achieve a closed system without adding dead space and to keep the pressure within the system similar to those encountered during FRC measurements in infants. Therefore the balloon served as a reservoir to ensure an approximately constant volume low pressure closed system over the whole breath cycle. The MM signal was then measured over 260 s (approximately five times longer than the average washin/washout time of the lung model). Any decrease of the MM indicated a loss of SF6 and hence allowed the magnitude of a leak to be quantified.
Statistics
For each parameter and set of six measurements (three washin and three washout) the mean±sd were calculated. Reproducibility of the system in vitro and in vivo was evaluated by calculating the coefficient of variation (CV). The accuracy of the measurements (limits of agreement) in the mechanical lung model was assessed with the difference between the measured volume and the mean of measured and preset volumes 14. To examine the effect of VT on the accuracy of FRC measurements in the lung model a two-way analysis of variance was used. Per cent error was defined as: 100×absolute value of (preset volume−measured volume)/preset volume. Differences between volume measurements in the lung model were assessed using a paired t-test. A p-value <0.05 was considered to be significant.
Results
Lung model
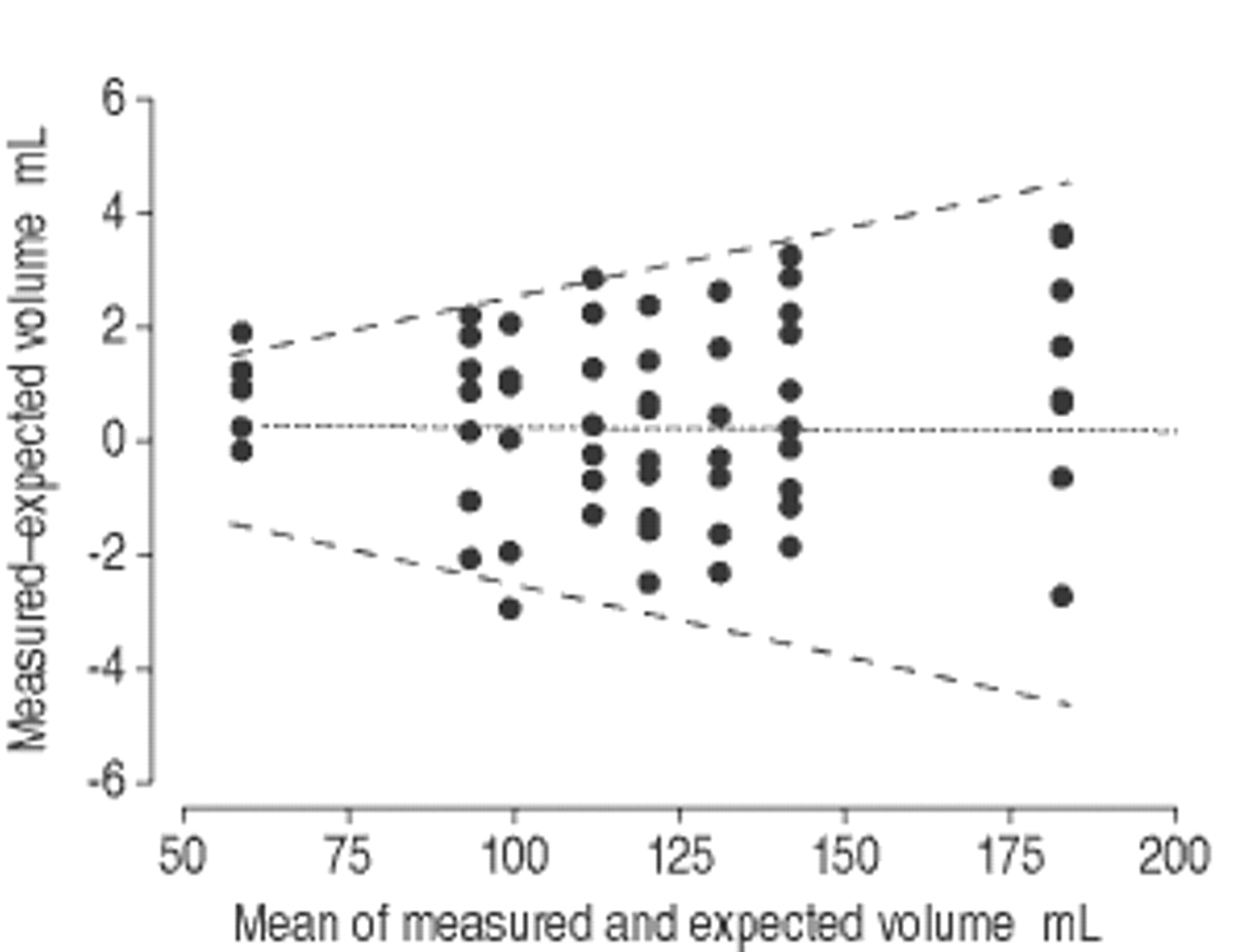
Bench tests in the mechanical lung model showed highly accurate volume measurements using the SF6 gas washin/washout technique. The FRC measurement error was 0.62±1.49 mL (range: 0–3.66 mL), with a CV of 1.3% and the error expressed in percent was 0.58±1.3% (range: 0–3.2%). The Altmann and Bland 14 plot in fig. 3⇓ shows the agreement between the measured and known volume of the mechanical lung model. Changes in VT or respiratory rate did not affect the accuracy of volume measurement in the lung model (p=0.46). Table 1⇓ compares the results with similar bench tests for measurements reported in the literature. The maximal leak was observed at a breathing frequency of 60 bpm and a VT of 74 mL. The MM signal decreased at these settings at a rate of 0.014 g·mol per min−1 (0.24% of the observed end-washin SF6 concentration) or with 0.00052 g·mol per breath−1 (0.009%). The authors therefore compensated the measured FRC data for the measured leak of the lung model. The precision of the measurement was within recommended measurement variability specified by the recent ERS-standards for infant lung function equipment 17, 18 (<2.5% for infant lung volumes between 50 and 300 mL, minimal 2 mL).
{kind=link}
{kind=link}
{kind=link}
Accuracy of in vitro assessment of lung volume. The average of the measured and known volume of a mechanical lung model is plotted against the differences. The dashed lines indicate the 95% confidence interval between the expected and the measured volumes (European Respiratory Society standards). ═: mean.
Accuracy of volume measurements in mechanical lung models reported in the literature
Healthy infants
Biometric data, FRC, and indices of ventilation distribution are shown in Table 2⇓. For each infant a minimum of six FRC (three washin and three washout) calculations were made. The mean CV for FRC during spontaneous breathing was 5.5±1.6% (range: 1.7–7.3%). FRC measured during washin showed no significant difference from FRC measured during washout (p=0.52), nor was there any change in tidal breathing during the washin or washout of SF6, VT prior to washin was 28.9±6.6 mL and VT at the end of washin was 29.7±6.8 mL. The VT/FRC ratio was within normal range (0.4–0.6). Table 3⇓ compares the ventilation indices with reported values in the literature.
Functional residual capacity (FRC) and measured ventilation distribution indices in 12 healthy infants
Comparison of ventilation distribution indices reported in the literature
Discussion
The measurement of lung volume (FRC) and ventilation inhomogeneities in infants with small airway disease is important to monitor the effects of therapeutic interventions such as bronchodilators and inhaled topical steroids. The breath-by-breath inert gas washout method provides a unique opportunity to diagnose such conditions without radiation or open lung biopsy or at least reduce the use of such methods. A new SF6 washin/washout technique to measure FRC and ventilation distribution was validated in a mechanical lung model and in unsedated healthy, spontaneously breathing infants. An ultrasonic flow sensor was used to simultaneously measure V′, V and the tracer gas concentration. High accuracy and reproducibility of the measurement technique could be demonstrated in a mechanical lung model. SF6 washin/washout measurements could be easily obtained in all infants, and reproducible FRC and ventilation distribution data calculated.
Any gas dilution technique to measure FRC has intrinsic limitations. He dilution can determine FRC highly accurately, provided there is no leak in the system. The technique is limited, however, as He analysers are sensitive to gases, other than He, such as CO2, O2, N2, and water vapour. In addition, it is not possible to assess ventilation distribution of the lung with the He dilution technique as the end-tidal He concentration is not analysed breath by breath. FRC and ventilation distribution can be measured with the multiple-breath N2 washout. However, MBNW using 100% O2 as a rebreathing gas should be avoided, as rebreathing pure O2 changes the breathing pattern during the measurement 15. Although MBNW is simple to perform in spontaneously breathing infants, changes in gas viscosity and travelling time of the sample gas to the N2 analyser will significantly affect the accuracy of the measurement 23. SF6 washout is a potentially suitable technique for infants, including those requiring near 100% O2 to maintain normal haemoglobin saturation. SF6 concentration has previously been measured using an infrared analyser, however these analysers have a low signal-to-noise ratio and variable response times 6, 7. SF6, He and N2 may be measured by a mass spectrometer with high precision, but the equipment is bulky and requires experienced staff to operate it. The gas dilution technique using an ultrasonic flow meter is unique, as V′ and MM can be measured simultaneously. Flow is determined by measuring the transit time of a pulsed ultrasound travelling through the streaming medium. The MM (g·mol−1) can subsequently be computed from the transit time with high accuracy and its value is directly proportional to the density of the medium. The ultrasonic flow sensor has several advantages over previous washin/washout techniques. Flow and gas concentrations are measured simultaneously and no cumbersome calibration and adjustment of the delay time between flow and tracer gas signal is necessary. Any inert gas with a different MM from air (28.85 g·mol−1) such as SF6 (146 g·mol−1) or He (4 g·mol−1) can be used as a tracer gas. Further, the same equipment can be used during both spontaneous breathing and mechanical ventilation 8. The SF6 technique is therefore highly suitable for measuring FRC and ventilation distribution.
The FRC values of the healthy infants in the present study were significantly lower than the calculated predicted values measured by the He dilution technique 19 (Table 2⇑). Some but not all difference may be explained by the different Bunsen coefficients (solubility) of He and SF6 (αSF6=0.0086 and αHe=0.0068 respectively, αSF6/αHe=0.79), which results in higher He reabsorbtion of the lungs and may lead an overestimation of FRC by 1.2% compared to SF6. SF6 has a 36-fold higher MM than He (146 g·mol−1 and 4 g·mol−1 respectively). Infants exhale to the closing volume of the lung during tidal breathing. It can be speculated, that more SF6 is trapped into these dependent parts of the lungs than He, resulting in underestimation of FRC. Furthermore previous studies with a He or N2 dilution technique used a much higher instrumental dead space, which may result in artifactually high FRC values. However, these differences are not of clinical relevance. In contrast to MBNW with 100% O2 15 the SF6 washin/washout did not change the breathing pattern of the investigated subjects with the measured VT remaining constant during the SF6 washin/washout. The different variability of the measured volumes in the lung model (1.3%) and the healthy infants (5.5%) may be explained by the irregular breathing patterns of infants. The variability of the measured FRC in the present study's healthy infants is similar to values reported in the literature and well within acceptable limits for infant lung function testing 7, 15.
There are only limited values of normal distribution indices reported in the literature (Table 3⇑). The present authors previously calculated AMDN, MDN and LCI of the MBNW in spontaneous breathing infants with lung disease 15. A low value of any index indicates even ventilation. AMDN discriminates between the healthy infants of the present study and the previously described infants with lung disease. PCD was higher than the values reported by Vilstrup et al. (healthy preterm infants) 7 but was lower than values measured in ventilated children with lung disease 8. Bronchial reactivity studies in infants with lung disease are needed to accurately quantify the sensitivity of the reported distribution indices.
Conclusion
Most of the current methods to measure functional residual capacity use either the N2 washout or the He dilution techniques in infants with lung disease. These techniques are only available for research purposes and are not commercially available. The all-in-one ultrasonic flow meter is highly suitable to measure functional residual capacity and ventilation distribution since flow, volume and gas concentration can be measured simultaneously using a single signal of a pulsed ultrasound and no cumbersome calibration and signal adjustment prior to the measurement is necessary. The present authors have demonstrated that such a technique has acceptable accuracy and has a good reproducibility in vitro as well as in vivo. A complete set of measurements can be easily obtained during regular and unsedated sleep in healthy infants. The breathing pattern of the investigated infants was unaffected by the measurement technique. Therefore a new noninvasive technique has been developed that can easily assess ventilation inhomogeneities and lung volumes, a potential sensitive marker of small airway disease in unsedated infants. This makes the technique useful for large epidemiological studies in healthy infants or for uncomplicated use in a clinical setting.
- Received March 15, 2001.
- Accepted March 22, 2002.
- © ERS Journals Ltd
References









