





Abstract
The present study compared the safety of 4.5 µg formoterol with 0.5 mg terbutaline, both by Turbuhaler® and used as needed, in addition to regular formoterol in moderate asthma.
In this double-blind parallel-group study, 357 patients taking a moderate-to-high dose of inhaled corticosteroids and additional terbutaline (2–5 inhalations·day−1 during run-in) were randomised to either formoterol or terbutaline as needed in addition to formoterol 9 µg b.i.d. over 12 weeks. Adverse events, serum potassium levels, electrocardiogram, vital signs and lung function were assessed monthly; peak expiratory flow and severe asthma exacerbations were recorded daily.
Patients used 2.16 (range 0.0–6.3) formoterol and 2.34 (range 0.1–7.5) terbutaline relief inhalations·day−1. No clinically significant differences in safety variables were found between treatments. Statistically greater increases in cardiac frequency (2.6 beats·min−1, p=0.03) were found on terbutaline. There were 44 and 52 severe asthma exacerbations with formoterol and terbutaline, respectively, with no significant difference in time to first exacerbation. There was also no difference between treatments for other efficacy measures (peak expiratory flow, forced expiratory volume in one second and morning/evening symptom scores).
Formoterol 4.5 µg as needed was at least as safe, well tolerated and effective as terbutaline 0.5 mg in stable patients (requiring up to 6 relief inhalations·day−1) taking formoterol plus inhaled corticosteroids regularly over 12 weeks.
This study was supported by AstraZeneca R&D Lund, Lund, Sweden.
Asthma therapy continues to evolve. Current treatment guidelines recommend inhaled corticosteroids for first-line anti-inflammatory therapy with short-acting β2-agonists as “relievers”, taken as needed for acute symptoms, and to prevent bronchospasm induced by exercise or other stimuli 1. Long-acting β2-agonists produce long-lasting bronchodilation and, added twice daily as regular maintenance therapy, reduce symptoms and exacerbations and improve quality of life 2–5. There is, however, an essential clinical difference between the two available long-acting β2-agonists formoterol and salmeterol. Formoterol displays a rapid onset of effect similar to that of the short-acting β2-agonists salbutamol or terbutaline, producing 80–90% of maximal effect within 5–10 min 6. By contrast, salmeterol takes ∼60 min to achieve this 7. Because of its rapid and long-lasting properties, formoterol can act as a reliever in acute attacks 8, rapidly reverse methacholine-induced bronchoconstriction 9 and prevent bronchoconstriction induced by exercise 10 and other stimuli 11. Hence, formoterol has the potential to replace a short-acting β2-agonist as a reliever, reducing the number of different inhalers necessary. This is likely to have a significant impact on adherence to therapy and has the potential to enhance asthma control.
Evidence for the effectiveness of formoterol as a reliever is rapidly accumulating 12, 13. However, before this unique role for formoterol, as (twice daily) maintenance medication and (as needed) reliever, is adopted, further evidence of safety and tolerability in patients taking multiple relief inhalations is required. Previous studies have compared formoterol with salbutamol, both used as needed 14–17.
A primary objective of the present study was to investigate the safety of as-needed formoterol as an alternative to a conventional short-acting β2-agonist reliever. In this study, the conventional short-acting β2-agonist terbutaline was used as the compaator because it was available in a Turbuhaler® (AstraZeneca, Lund, Sweden) in all participating countries. Formoterol and terbutaline, both by Turbuhaler®, were compared in a 12-week double-blind reference-controlled clinical trial in patients requiring reliever medication despite regular maintenance twice-daily, inhaled corticosteroids and formoterol 9 µg b.i.d.
Materials and methods
Patient characteristics
The study was performed in males and females aged >18 yrs with asthma according to the American Thoracic Society definition 18. Prior to enrolment, their asthma had to have been stable on an adequate constant dose of an inhaled corticosteroid for >4 weeks. Patients could also be included if they took a constant low dose of an oral steroid (maximum 10 mg·day−1 prednisolone or equivalent) during this period, provided that this dose was continued throughout the study. For inclusion, baseline forced expiratory volume in one second (FEV1) had to be >50% of the predicted normal value 19. Patients with significant cardiovascular or other disease, pregnant or breast-feeding females, or patients with hypersensitivity to lactose or β2-agonists were not enrolled. β2-Agonists (other than the study drugs), anticholinergics, leukotriene receptor antagonists, cromones or immunotherapy were not permitted.
Study design
This was a randomised double-blind reference-controlled trial performed in two parallel groups in 42 centres in five countries (the UK, Spain, Israel, Finland and Hungary). There was an initial single-blind 2-week run-in period during which all patients received formoterol (Oxis®; AstraZeneca) 9 µg b.i.d. (delivered dose corresponding to a metered dose of 12 µg) and terbutaline 0.5 mg as needed, both by Turbuhaler®. Patients requiring a mean of 2–5 inhalations·day−1 terbutaline 0.5 mg during the run-in period were randomised. For safety reasons, patients who used >8 inhalations during a single day were not included in the study. All patients who completed the run-in period according to the protocol were randomised to a 12-week treatment phase consisting of formoterol 9 µg b.i.d. and either formoterol 4.5 µg or terbutaline 0.5 mg as needed. During the study, patients attended the clinic on five occasions. Between visits, they were telephoned to check usage of reliever medication and occurrence of adverse events. A measure of compliance was obtained by asking the patients to record morning and evening usage of their regular formoterol Turbuhaler® medication.
Before the run-in and treatment periods, patients were instructed to use their as-needed medication for either relief of asthma symptoms or prevention of bronchoconstriction (e.g. before exercise) and to appraise the effect of each inhalation before proceeding with a second. To preserve blinding, both formoterol and terbutaline were administered by identical Turbuhaler® devices.
The study was performed in accordance with the Declaration of Helsinki. Each local Independent Ethics Committee approved the study protocol and patient information sheet and each investigator obtained signed informed consent before conducting any study-related procedures.
Primary outcome measures
Serum potassium level, electrocardiogram, laboratory measurements and vital signs
Blood (4 mL) was collected for serum potassium measurements before enrolment and after 1 and 3 months of treatment. The protocol specified that patients experiencing a fall in serum potassium (of >1 mM) should be retested weekly until a satisfactory stable level, as judged by the investigator, was reached. If the serum potassium settled at >0.7 mM below the lower limit of the reference range, the patient was to be withdrawn from the study and potassium levels measured until normalisation (compared with pretreatment value) occurred.
A 12-lead resting electrocardiogram (ECG) was recorded at all visits to determine cardiac frequency, PR interval, QRS duration and QT interval (lead II), in addition to rhythm, ST and T wave changes, and overall interpretation. Any clinically relevant deterioration was documented as an adverse event.
Blood and urine samples were collected for routine laboratory measurements (haematology and clinical chemistry) at enrolment and the final visit.
At all visits, after a 15-min rest in a sitting position and before lung function measurements, pulse rate was measured over 30 s, following which systolic and diastolic blood pressure were recorded.
Adverse events
Adverse events were detected by means of the standard question “Have you had any health problems since the last visit/telephone call?” The question was addressed to each patient at the end of the run-in period and at all subsequent visits during the treatment period, including the three telephone contacts. Spontaneously reported and/or observed adverse events and the patient's response to this question were recorded along with information about severity, date of onset and recovery, maximum intensity, action taken and outcome.
Secondary outcome measures
Extent of reliever use
The number of inhalations of as-needed medication taken during the day and night were recorded and differences between the treatment groups analysed.
Asthma exacerbations
A severe asthma exacerbation was defined as a requirement for oral glucocorticosteroids, either as judged by the investigator or following a drop in morning peak expiratory flow (PEF) on 2 consecutive days to <70% of a mean baseline value established during the run-in period. Severe exacerbations were treated with oral prednisolone 30 mg·day−1 for 10 days, reducing by 5 mg·day−1 over the next 5 days. In the case of a second severe exacerbation, the patient was withdrawn.
Lung function
PEF was measured using a peak flow meter (Vitalograph®; Vitalograph, Buckingham, UK), and recorded morning and evening as the highest of three readings before intake of twice-daily study medication.
FEV1 was determined as the best of the two highest recordings, from a minimum of three measurements, where the lower value was within 5% of the higher. At all clinic visits, FEV1 was measured before and after inhalation of 1.5 mg terbutaline to assess maximum bronchodilator response and evaluate change in lung function over time.
Asthma symptoms
Throughout the study, the patients completed a symptom-scoring diary twice daily, in the morning directly after awakening for night-time asthma (0: no symptoms during the night; 1: symptoms causing you to wake once or to wake early; 2: symptoms causing you to wake twice or more (including waking early); 3: symptoms causing you to be awake for most of the night; and 4: symptoms so severe that you did not sleep at all) and at bedtime for daytime asthma (0: no symptoms during the day; 1: symptoms for one or more short periods during the day; 2: symptoms for most of the day which did not affect your normal daily activities; 3: symptoms for most of the day which affected your normal daily activities; and 4: symptoms so severe that you could not go to work or perform normal daily activities). Symptom scores (0–4) were recorded for breathlessness, chest tightness, wheeziness and cough, with or without sputum.
Statistical analysis
When planning the study, there were no background data available from similar studies. However, the sample size was chosen so as to be sufficiently large to document the safety of formoterol Turbuhaler® 4.5 µg administered as needed.
The adverse event profile was analysed using descriptive statistics and qualitative analyses. Statistical analyses for detecting significant differences between the treatments were not performed. For vital signs, ECG and laboratory values, changes between baseline and the end of the treatment period were analysed using a Wilcoxon rank sum test for independent samples.
The change in the mean daily number of as-needed inhalations from the last 7 days of the run-in period to the last 28 days of the treatment period for each patient was compared between the two treatment groups. Change was evaluated using an analysis of variance model with treatment and centre as fixed factors and the number of run-in mean daily relief inhalations as covariates. An intention-to-treat analysis was used; all patients who were randomised and yielded data from the run-in and treatment periods were included. Other diary card variables (symptom scores and PEF) were described and analysed in the same way. The number of severe asthma exacerbations was described and the time to the first severe asthma exacerbation was compared between the two groups using a log-rank test.
The values listed in the results are presented as the means from the run-in and treatment periods. Changes from run-in to the end of the treatment period and differences between formoterol and terbutaline are the estimated means from analysis of variance. Consequently, the differences between run-in and treatment means do not, in general, coincide exactly with the estimated changes and mean differences. For adverse events, the analysis was restricted to a descriptive comparison because there was a wide range of classifications. Formal statistical testing would have needed multiple tests, introducing a high type I error risk.
Results
Study population
Of the 632 patients who entered the run-in period, 275 were not eligible for randomisation, mainly because they used their relief medication either too much (>5 inhalations·day−1) or too little (<2 inhalations·day−1) during run-in. A total of 357 patients were randomised to treatment; 176 were given formoterol and 181 terbutaline. There were no differences between the two treatment groups in demographic data or baseline characteristics (table 1⇓), and 83% of each group completed the 3-month treatment period. Of the 62 patients who did not complete the study, 17 were incorrectly included, 20 (10 formoterol and 10 terbutaline) experienced asthma deterioration and eight (four formoterol and four terbutaline) exhibited other adverse events, such as haematological and other laboratory abnormalities, which led to an intervention, dose reduction or significant additional therapy. Nine patients were lost to follow-up and eight discontinued for personal reasons. Compliance in the study was good, with ≥90% of patients taking 4 inhalations·day−1 of their b.i.d. medication (formoterol 4.5 µg) as instructed.
Patient demographics
Primary outcome measures
Serum potassium level, electrocardiogram, laboratory measurements and vital signs
Changes in serum potassium level, ECG measurements and vital signs from run-in to the end of treatment are presented in table 2⇓. In addition to these results, analysis of variance revealed that the mean differences between groups, with regard to changes from the run-in period, were not significantly different for serum potassium level, pulse rate, systolic or diastolic blood pressure, or PR interval. However, compared with the formoterol group, the terbutaline group experienced small but significantly greater increases in cardiac frequency (2.6 beats·min−1, p=0.03). The QT interval was significantly more prolonged (by a mean of 6.7 ms) in the formoterol group compared with the terbutaline group (p=0.02), but comparison of cardiac frequency-adjusted QTc did not show any significant differences between the two groups (p=0.82).
Vital signs, electrocardiogram parameters and serum potassium level measurements
There were no changes in mean haematology or clinical chemistry laboratory values for either reliever. Individual laboratory values generally showed only small isolated changes that were not considered clinically relevant. The number of individual treatment-related laboratory changes was similar for both the formoterol and terbutaline groups.
Adverse events
Both treatment groups showed a similar distribution with regard to the total number of adverse events, reported symptoms and intensity of symptoms; table 3⇓ presents the most frequently reported adverse events. Seven adverse events in the formoterol group (three aggravated asthma, one pneumonia, one diabetes mellitus, one osteoporosis and one angina pectoris) and one in the terbutaline group (accident and/or injury) were reported as serious adverse events. Of these serious adverse events, only one (in the formoterol group) was considered to be possibly related to the study drug; the patient complained of pain/angina pectoris in connection with an asthma attack. Fourteen patients in each treatment group discontinued the study due to adverse events. For 10 patients in each treatment group, this was due to aggravation of the patient's asthma. In the formoterol-treated group, four patients discontinued due to pneumonia, angina pectoris, dysphonia and osteoporosis, respectively. Events necessitating discontinuation in four terbutaline-treated patients were headache, pharyngitis, cramps and fibromyalgia syndrome.
Adverse events
There is no clear pattern indicating difference between treatment groups with regard to tremor (table 3⇑). In the group that received formoterol 9 µg b.i.d. plus terbutaline as needed during the run-in, and then were randomised to as-needed formoterol, 11 patients showed tremor while on terbutaline as needed in the run-in but only six continued with tremor after changing to formoterol. Two patients started experiencing tremor after changing from terbutaline to formoterol. Likewise, in the group that received formoterol 9 µg b.i.d. plus terbutaline as needed during the run-in, and continued with the same as-needed treatment, five patients experienced tremor during run-in, three showed continued tremor and only one patient started experiencing tremor during the randomised treatment.
Secondary outcome measures
Extent of reliever use
In addition to regular use of formoterol (2×4.5 µg b.i.d.), patients took on average either 2.16 doses of formoterol 4.5 µg or 2.34 doses of terbutaline 0.5 mg as needed. The mean daily number of inhalations of reliever medication throughout the study is shown in figure 1⇓. The reduction in number of inhalations immediately after randomisation is an artefact rather than a real decline in reliever use, since it represents daytime use only rather than usage over 24 h.

Use of reliever medication (□: formoterol; ▪: terbutaline) throughout the study. Data are presented as daily means (═: end of run-in and start of treatment period).
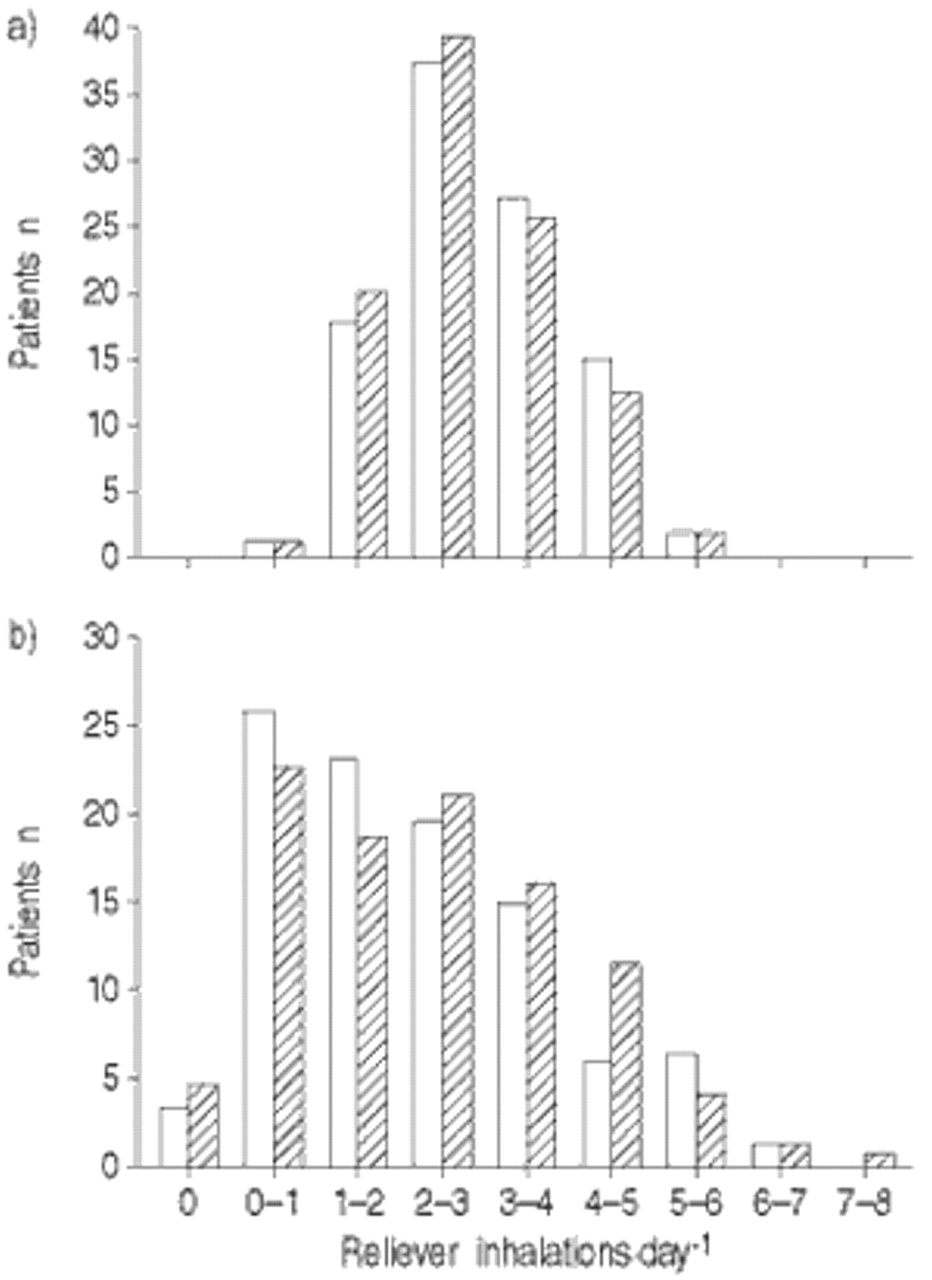
The number of daytime and night-time as-needed inhalations during the run-in and treatment periods was very similar in the two groups (table 4⇓). On average, patients in the formoterol group decreased their reliever use by 0.21 inhalations·day−1 compared with the terbutaline group, but this was not significant. However, the mean reduction in daytime reliever use (0.21 inhalations) was significantly greater with formoterol compared with terbutaline (p<0.05) (table 4⇓); night-time reliever use did not differ between the two treatments. The distribution of the mean number of daily reliever inhalations during the last 7 days of the run-in and last 28 days of the treatment period is shown in figure 2⇓; there was no difference between treatments. A total of 24 patients occasionally exceeded a total of 12 inhalations·day−1 (i.e. >8 as needed plus 4 regular formoterol), 11 in the formoterol group and 13 in the terbutaline group; 67% of these patients did so for only 1 day.

Distribution of as-needed reliever use (□: formoterol; └: terbutaline) during: a) the last 7 days of the run-in period; and b) the last 28 days of the treatment period.
Daily use of reliever and asthma control medication
Asthma exacerbations
Severe asthma exacerbations have previously been used as an important measure of asthma control 3. In the formoterol group, 34 patients had a severe exacerbation, 10 of whom had a second exacerbation and were accordingly withdrawn from the study. Similarly, in the terbutaline group, 39 patients had a severe exacerbation; of these patients, 13 had a second exacerbation, but only 10 were withdrawn as three were not detected in time. There was no significant difference between the two groups in estimated probability of not having a severe asthma exacerbation or discontinuation/hospitalisation due to deterioration of asthma.
Lung function
The mean±sd morning PEF during the last 7 days of the run-in period was 350±99 L·min−1 in the formoterol group and 347±103 L·min−1 in the terbutaline group; this remained unchanged for both drugs throughout the treatment period (mean of the last 28 days) (fig. 3⇓). Similarly, evening PEF did not change in either group from the mean run-in values (357±103 and 356±103 L·min−1 in the formoterol and terbutaline groups, respectively). Furthermore, there were no differences in diurnal variation in PEF with either treatment, although there was a nonsignificant trend towards higher PEFs with formoterol.

Morning peak expiratory flow (PEF) throughout the study (□: formoterol; ▪: terbutaline). Data are presented as means (═: end of run-in and start of treatment period).
Neither FEV1 nor maximum bronchodilator response (after terbutaline 1.5 mg) changed throughout the study (fig. 4⇓), confirming that there was no development of tolerance. There were no significant differences between the two treatment groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mean forced expiratory volume in one second (FEV1) on formoterol 4.5 μg (▴) and terbutaline 0.5 mg (▪) as needed before (––––) and after (- - -) inhalation of 1.5 mg terbutaline.
Asthma symptoms
The mean symptom score at run-in was low for daytime and night-time symptoms (1.3 and 0.8 out of a possible 4.0, respectively) so there was little room to show improvement with either treatment. The changes between run-in and treatment were small, with no significant differences between treatments.
Discussion
Long-acting inhaled β2-agonists are recommended as add-on therapy for patients with suboptimally controlled asthma despite regular inhaled corticosteroid and short-acting β2-agonist reliever medication 1. However, the rapid onset of action of formoterol suggests a possible additional therapeutic role, replacing a conventional short- and rapid-acting β2-agonist as a reliever.
The primary objective of the present study was to examine the relative safety of as-needed formoterol 4.5 µg in comparison with terbutaline 0.5 mg in patients with moderately severe asthma who required approximately three rescue inhalations of β2-agonist in addition to regular b.i.d. formoterol 9 µg plus inhaled corticosteroid. In general, both treatments at standard doses were shown to be equally safe and effective with no clinically relevant differences between the groups. An apparent excess incidence of tremor on formoterol can be accounted for by patient randomisation. Of the eight patients experiencing tremor on formoterol, only two started to report this effect when randomised to formoterol, six having already reported it while on terbutaline in the run-in period. Similarly, five patients in the terbutaline group experienced tremor during run-in, three continued to report this effect after randomisation, with a further patient developing tremor. Although there were no previous studies on which to base any power calculation, the sample size allowed detection of significant differences that favoured formoterol. Significantly higher mean cardiac frequencies were observed in the terbutaline group and an increased mean QT interval in the formoterol group. However, cardiac frequency-adjusted QTc did not differ between treatments. No other significant differences in ECG, vital signs or laboratory measurements were found.
The number and pattern of adverse events were similar for both treatments with no trends suggesting adverse drug effects. A single nonlife-threatening episode of angina pectoris in connection with an asthma attack was reported in the formoterol group, and was classified according to the protocol as “possibly drug-related” because this effect has been reported rarely for β2-agonists. In the 24 h prior to the occurrence of this event, the patient had taken the most as-needed formoterol treatment amongst patients in the trial (6 inhalations) and had also taken additional terbutaline (2 inhalations). Au and co-workers 20, 21 evaluated retrospectively the effect of β2-agonist use on risk of myocardial infarction, demonstrating, in one US health maintenance organisation, that patients with a history of cardiovascular disease who collected their first prescribed β2-agonist metered-dose inhaler had an increased risk of myocardial infarction within 3 months compared with matched controls. However, this effect was not seen at higher doses of β2-agonist and the study did not involve proven asthmatics on regular therapy, or monitoring (diary recordings of β2-agonist use, symptoms or PEF). This, therefore, represents a hypothesis-generating epidemiological observation in a very different population to the present study, and the one angina pectoris case cannot definitely be attributed to treatment.
These safety outcomes are in line with those of another study in which formoterol 4.5 µg as needed, up to a maximum of 54 µg, was compared with terbutaline 0.5 mg, up to 6 mg, in 362 patients taking inhaled corticosteroids 12. Furthermore, other acute studies have shown formoterol Turbuhaler® to be safe at doses up to 90 µg in patients with stable as well as acute severe asthma 8, 22. For safety reasons, the total dose of formoterol in the present study was not allowed to exceed 54 µg (18 µg regular plus 36 µg as needed), equivalent to 12 inhalations·day−1. In the terbutaline group, the maximal dose was 18 µg formoterol plus 4 mg terbutaline as needed. The patients exhibited a mean as-needed use of 2.16 and 2.34 inhalations·day−1 formoterol and terbutaline, respectively. Although 6.7% of patients exceeded a total daily dose of 12 inhalations, in two-thirds this occurred on a single day only. This study in 176 patients, the first of as-needed formoterol designed with safety as the primary objective, demonstrates that formoterol is at least as safe and well tolerated as terbutaline when taken as reliever medication for a 12-week period despite its longer duration of action. It extends previous observations of the use of formoterol as needed, approximately doubling the numbers of patients studied.
Over the 12-week study, no differences in efficacy were seen between the two treatments. The number of severe asthma exacerbations differed numerically, but not significantly, in favour of formoterol. A small reduction in the daily use of as-needed medication also favoured the formoterol group. Asthma symptom scores were <1.0 (out of a possible 4.0) in both groups. A plausible explanation for the small difference in as-needed use is that relievers were taken to prevent as well as to treat asthma symptoms. The lack of difference in asthma control between additional formoterol as reliever and terbutaline is attributed to the regular use of 9 µg formoterol b.i.d. in both groups. This is compatible with the known flat dose/response associated with regular long-acting β2-agonists 23, 24. The efficacy of formoterol was not specifically investigated as this is well established 3, 12, 25, 26.
It could be argued that different conclusions might be reached in a different patient population, but patients with milder asthma would have required even fewer as-needed inhalations. Patients with more severe asthma could potentially have been selected but the patients investigated resembled those included in another large study 3. The use of formoterol together with inhaled steroids during run-in produced good control with relatively few symptoms, although there remained a need for reliever use, which, in 6.7% of patients, exceeded 8 inhalations·day−1. It might have been considered unethical to include patients with very high reliever use in a study of as-needed formoterol in the first instance. Following the present results, it would be useful to make further comparisons in patients with very severe asthma, e.g. with hypoxaemia. In a small study of patients with acute severe exacerbations of asthma, conducted under close observation, higher doses of formoterol (up to 90 μg over 24 h) were shown to be safe and effective 8.
Salbutamol is the most widely used inhaled β2-agonist. Although minor differences between salbutamol and terbutaline have been demonstrated in carefully controlled dose/response laboratory studies (e.g. Wong et al. 27), no clinically significant differences have been observed at doses of 2–3 inhalations·day−1. Comparison of formoterol with salbutamol in the present study would have involved a more complicated double-dummy design. Previous studies have compared formoterol with salbutamol, both used as needed 14–17, and these have been discussed by Tattersfield et al. 12.
There is general concern that frequent use of β2-agonists may be associated with asthma deterioration or decreased bronchodilator response 28, 29. The present results demonstrate that despite a mean use of 2–3 as-needed inhalations·day−1 formoterol or terbutaline in addition to 9 µg formoterol b.i.d. for 3 months, there was no reduction in PEF or FEV1. Furthermore, postbronchodilator FEV1 remained unchanged throughout the study, indicating no evidence of asthma deterioration or development of tachyphylaxis to terbutaline during the study.
In conclusion, the present study indicates that formoterol is at least as safe, well tolerated and effective as terbutaline when used as needed in patients taking inhaled corticosteroids and b.i.d. formoterol. Hence formoterol could replace conventional short-acting β2-agonists as reliever medication. Current pricing may result in additional drug costs but the requirement of one less inhaler would improve convenience and may improve adherence to treatment regimens. This merits further evaluation in a “real-world” setting.
- Received September 7, 2001.
- Accepted April 27, 2002.
- © ERS Journals Ltd
References









