





Abstract
A recent case of iatrogenic Cushing's syndrome and complete suppression of the pituitary-adrenal-axis in a patient with cystic fibrosis (CF) and allergic bronchopulmonary aspergillosis treated with itraconazole as an antifungal agent, and budesonide as an anti-inflammatory agent led to a systematic assessment of this axis and gonadal function in all patients treated with itraconazole in the authors' CF centre. Itraconazole can inhibit CYP3A, thus interfering with synthesis of gluco- and mineralocorticoids, androgens and oestradiol as well as the metabolism of budesonide. The aim of this study was to evaluate adrenal and gonadal function in patients treated with itraconazole with or without budesonide.
An adrenocorticotrophic hormone (ACTH) test (250 µg tetracosactid) was performed in 25 CF patients treated with both itraconazole and budesonide, and in 12 patients treated with itraconazole alone (six patients with CF and six with chronic granulomateous disease). Mineralocorticoid and gonadal steroid function were evaluated by measurements of plasma-renin, follicle stimulating hormone, luteinising hormone, progesterone, oestradiol, testosterone, serum-inhibin A and B. ACTH tests performed as part of a pretransplantation programme in an additional 30 CF patients were used as controls.
Eleven of the 25 patients treated with both itraconazole and budesonide had adrenal insufficiency. None of the patients on itraconazole therapy alone nor the control CF patients had a pathological ACTH test. Mineralocorticoid and gonadal insufficiency was not observed in any of the patients. Only one patient with an initial pathological ACTH-test subsequently normalised, the other 10 patients improved but had not achieved normalised adrenal function 2–10 months after itraconazole treatment had been discontinued.
Suppression of the adrenal glucocorticoid synthesis was observed in 11 of 25 cystic fibrosis patients treated with both itraconazole and budesonide. The pathogenesis is most likely an itraconazole caused increase in systemic budesonide concentration through a reduced/inhibited metabolism leading to inhibition of adrenocorticotrophic hormone secretion along with a direct inhibition of steroidogenesis. In patients treated with this combination, screening for adrenal insufficiency at regular intervals is suggested.
- adrenal insufficiency
- allergic bronchopulmonary aspergillosis
- budesonide
- CYP3A
- cystic fibrosis
- itraconazole
Allergic bronchopulmonary aspergillosis (ABPA) is characterised by a dual-type immune response with immunoglobulin (Ig) E and IgG antibodies to the fungus Aspergillus fumigatus 1. It is diagnosed in ∼8% of cystic fibrosis (CF) patients and in 1–2% of patients with bronchial asthma 2–4. The mainstay of treatment for ABPA in CF, as in patients with bronchial asthma, has been systemic glucocorticoids, but this is associated with serious side-effects particularly in growing children 5–7. Treatment with itraconazole, an orally administered triazole antifungal agent, has recently been recommended for the treatment of ABPA as an efficient alternative or steroid-sparing therapy without serious side-effects 8–10. Itraconazole is, like other antibiotics, administered in high doses in CF patients due to the endobronchial barrier and altered pharmocokinetics, especially with regard to the increased renal excretion 11. Budesonide is given as an anti-inflammatory agent in many CF centres 12, 13. High-dose budesonide was primarily recommended to CF patients chronically infected with Pseudomonas aeruginosa 14, but has since been extended to include CF patients with other bacterial infections. Azoles such as ketoconazole and itraconazole are strong inhibichrome P450-dependent enzymes such as 17,20 desmolase, 16α-hydroxylase, 17α-hydroxylase, 18 hydroxylase and 11β-hydroxylase enzymes (listed with decreasing activity), thus potentially compromising steroidogenesis in the adrenals and gonads 18, 19. Budesonide is metabolised to 16‐α‐hydroxyprednisolone and 6‐β‐hydroxybudesonide by hepatic CYP3A 15, and the metabolism is therefore reduced in individuals taking drugs that inhibit CYP3A.
The frequency of suppression of the pituitary-adrenal-axis and gonadal steroidogenesis due to pharmacological interaction of itraconazole and budesonide was prospectively studied in a group of 31 patients with CF and six patients with chronic granulomateous disease (CGD) and compared to a control group of 30 CF patients who had been tested as part of a pretransplantation programme.
Patients and methods
Patients
All CF patients (n=31) from the Danish CF Centre, Copenhagen, who were treated with itraconazole for ABPA agreed to participate in the study. Up until the end of 1999 31 patients (16 females, 15 males, median age 18 yrs (range 9–33 yrs)) of a total of 271 patients (11%) were treated with high-dose itraconazole (400–600 mg·day−1, 10 mg·kg−1·day−1). Five patients were also treated with prednisolone and four patients with clarithromycin. Eight of the females aged >15 yrs used oral contraception and three females did not. Of the five female patients aged <15 yrs one was Tanner stage of puberty 4, two were stage 4–5, one was stage 5 and in one patient the stage was unknown.
Group 1: Twenty-five patients were treated, concomitantly with high-dose budesonide inhalations (Spirocort Turbohaler®, AstraZeneca, Albertslund, Denmark) (800–1600 µg day, median age 18 yrs (range 9–33 yrs)) and itraconazole. Group 2: Six patients were treated with itraconazole alone. Group 3: Six patients with CGD who were on continuous prophylactic treatment with high-dose itraconazole for ABPA (two females, four males), median age 24 yrs (range 15–32 yrs). None of these patients were or had been treated with budesonide or clarithromycin. Group 4: The adrenocorticotropic hormone (ACTH) test results from a group of 30 CF patients were retrospectively included as controls (14 females, 16 males), median age 29 yrs (range 21–43 yrs). An ACTH test had been performed as part of a pre-operative evaluation for lung transplantation. None of these patients were treated with itraconazole but 24 of them had been treated for several years with high-dose inhaled budesonide. The remaining six were not treated with glucocorticosteroids.
Follow-up
Patients with pathological ACTH test results, not treated with prednisolone, started with hydrocortisone substitution therapy (10–12 mg·m−2·day−1) after withdrawal of itraconazole. The budesonide treatment was slowly withdrawn if the patients did not experience a deterioration in asthmatic symptoms. After withdrawal of itraconazole the adrenal function was retested with ACTH tests at intervals of 1–3 months.
Methods
Measurements of glucocorticoids and mineralocorticoids
Adrenocorticotropic hormone test
Plasma cortisol was measured before (time 0), 30 and 60 min after intravenous (i.v.) injection of 250 µg tetracosactid (Synacthen®, Novartis Healthcare, Copenhagen, Denmark). The normal response was defined as an increase of plasma cortisol to at least 500 nmol·L−1 after 60 min (AutoDelfia, Wallac, Finland). Patients treated with prednisolone at the time of testing did not take the medication on the test day. In these patients cortisol was measured using high-performance liquid chromatography (Merck, Hitachi, Japan), a method in which cross-reactivity between cortisol and prednisolone is avoided.
Plasma adrenocorticotropic hormone
Plasma ACTH was measured at time 0 (normal range 2–11 pmol·L−1) using a radioimmunoassay (RIA) (Nichols Inst., Diagnostics, CA, USA).
Measurements of gonadal hormones
Sex-hormone analyses (at time 0): plasma follicle stimulating hormone (detection limit 0.05 IU·L−1), luteinizing hormone (detection limit 0.06 IU·L−1) and progesterone concentration (detection limit 0.8 nmol·L−1) were measured by a time-resolved immunofluorometric assay (Delfia, Wallac, Finland).
Testosterone concentration (detection limit 0.23 nmol·L−1) was determined by RIA (Coat‐a‐Count; Diagnostic Products Corporation, LA, USA). Oestradiol concentration (detection limit 18 pmol·L−1) was also determined by RIA (Immunodiagnostic Systems, Boldon, UK). Inhibin‐A (detection limit 7 pg·mL−1) 22 and inhibin‐B concentrations (detection limit 18 pmol·L−1) 23 were determined by enzyme-linked radioimmunosorbant assay (ELISA).
Statistics
Statistical analysis was performed using the nonparametric Mann-Whitney U‐test for comparison between two groups. For comparison between more than two groups the nonparametric Kruskall-Wallis test was used. A p<0.05 was considered significant.
Ethics
Ethical approval was obtained ((KF) 01-046/00) and the study was performed according to the Helsinki II declaration.
Results
Glucocorticoid and mineralocorticoid function
A pathologically low response to the ACTH test was found in 11 of 25 (44%) CF patients treated with itraconazole and budesonide (Group 1a) (table 1⇓). Plasma ACTH was low in eight of the 11 patients, normal in two patients and in one patient plasma ACTH was not measured initially but a subsequent analysis was normal (table 1⇓). Some patients were treated with prednisolone or claritromycin (table 1⇓). One patient developed Cushing's syndrome with moon face, striae, facial hair growth, headache, mood swings, increased insulin requirement, dysregulation of diabetes, high HbA1c and irregular menstruations (table 1⇓, patient no. 3).
Details of 11 patients with cystic fibrosis and allergic bronchopulmonary aspergillosis showing a pathological adrenocorticotropic hormone test
A normal response to the ACTH test was found in the remaining 14 CF patients treated with itraconazole and budesonide (Group 1b) and the six CF patients treated with itraconazole alone (Group 2) (fig. 1⇓). Two patients were treated with clarithromycin and two other patients with prednisolone. The plasma-ACTH levels were within the normal range (fig. 2⇓).

Maximal plasma-cortisol levels 60 min after stimulation with tetracosactid (250 µg) in patients treated with budesonide and itraconazole with a low response to the adrenocorticotropic hormone test (Group 1a, n=11), patients treated with budesonide and itraconazole with a normal response to the adrenocorticotropic hormone test (Group 1b, n=14), patients treated with itraconazole alone (Group 2, n=6), patients with chronic granulomateous disease treated with itraconazole (Group 3, n=6), and controls (Group 4, n=30). The minimal level of a normal response is 500 nmol·L−1. Two patients in Group 4 had levels <500 nmol·L−1 due to administration of prednisolone at time of testing.

{kind=link}
{kind=link}
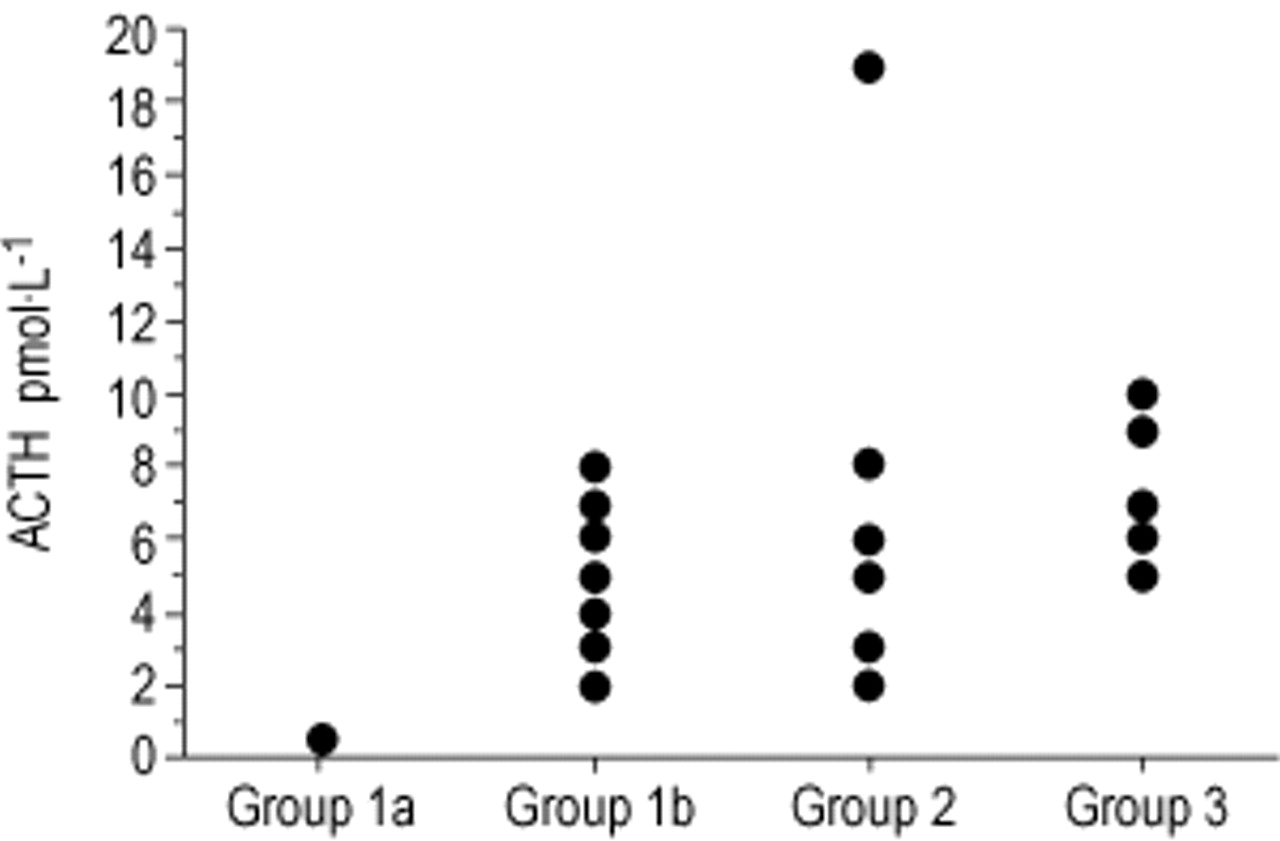
Plasma-adrenocorticotropic (ACTH) levels in patients treated with budesonide and itraconazole with a low response to the ACTH test (Group 1a, n=11), patients treated with budesonide and itraconazole with a normal response to the ACTH test (Group 1b, n=14), patients treated with itraconazole alone (Group 2, n=6), patients with chronic granulomateous disease treated with itraconazole (Group 3, n=6).
The accumulated itraconazole dose in CF patients with a pathologically low response to the ACTH test was not significantly different from the accumulated itraconazole dose in CF patients with a normal response to the ACTH test (median 420 g (range 3–788 g) versus 453 g (range 4.8–1047 g) (p=0.95).
All six CGD patients (Group 3) treated with itraconazole alone had a normal reponse to the ACTH test (fig. 1⇑) as well as a plasma ACTH within the normal range (fig. 2⇑). The plasma ACTH values were not statistically different within the different groups (p=0.1).
Twenty-four of the 30 CF patients in the control group treated with high-dose budesonide alone (Group 4), had a normal response to the ACTH test (fig. 1⇑). Plasma-ACTH was not measured in these patients.
Mineralocorticoid insufficiency was not observed in any of the 31 CF patients treated with itraconazole as indicated by normal plasma-renin concentrations (Group 1a: median 21, range 7–84 mIU·L−1; Group 1b: median 18, range 5–46 mIU·L−1; Group 2: median 14, range 4–53 mIU·L−1; Group 3: median 21, range 11–107 mIU·L−1). The renin values were not statistically different within the groups (p=0.9). Renin measurements were not performed in Group 4.
Gonadal function
Suppression of sex-hormone secretion was not observed in any of the 31 CF patients or the six CGD patients treated with itraconazole. In one male CF patient a high follicle stimulating hormone (FSH) (24.9 nmol·L−1) and low serum-inhibin B (<20 pg·mL−1) level were observed indicating lack of Sertoli cell function unrelated to the current investigation and the disease being studied.
Follow-up
Most of the patients with an initial pathological ACTH test improved, but the adrenal function did not normalise after a follow-up of 2–10 months (table 1⇑). In six patients the tetracosactid-stimulated plasma cortisol level increased after withdrawal of itraconazole to levels of ∼250–400 nmol·L−1. The subsequent tests showed only a slow further improvement in adrenal function. Substitution with hydrocortisone at a standard dose resulted in symptoms of Cushing's syndrome, consisting of moon face and deterioration in glucose tolerance, in two patients.
After withdrawal of itraconazole treatment, all the patients were closely controlled with specific IgG subclass antibodies to A. fumigatus 24 in order to follow the activity of ABPA. In patients with increasing specific IgG subclass antibodies and clinical signs of exacerbation in ABPA, itraconazole treatment was restarted after withdrawal of budesonide.
In all CF and CGD patients with an initial normal ACTH test a retest was performed ∼3 months later. A normal test was obtained in all these patients.
Discussion
Adrenal insufficiency was found in 11 of 25 CF patients with ABPA treated with a combination of itraconazole and budesonide. Only patients treated with both itraconazole and budesonide showed adrenal insufficiency, whereas none of the patients treated with either itraconazole or budesonide alone were affected. None of the 11 patients with adrenal insufficiency had experienced severe disease or other traumas.
The observed suppression of adrenal cortisol synthesis combined with Cushing's syndrome in one of the patients, most likely represents a pharmacological interaction between budesonide and itraconazole. Thus, Cushing's syndrome in this patient may be explained by an increased systemic concentration of budesonide due to inhibition of CYP3A4, and in turn, suppression of pituitary ACTH production leading to adrenal insufficiency. In addition, steroidogenesis in the adrenals may be suppressed by itraconazole 25.
The antifungal activity of azoles is exerted through the binding to and deactivation of the cytochrome P450 mediated enzyme, 14-desmethylase, responsible for converting lanesterol into ergosterol, which is an essential component of the fungal membrane 8, 26. Ketoconazole is known to produce clinically relevant interactions 27, and is utilised in certain patients to control hypercortisolism of either pituitary or adrenal origin 28, 29. Though itraconazole is a 10-times less potent inhibitor of CYP3A than ketoconazole in vitro 30, it is a potent inhibitor of the metabolism of various CYP3A4 drugs in vivo, including some synthetic glucocorticoids e.g. dexamethasone and methylprednisolone 17. Although other azole compounds (itraconazole, fluconazole and miconazole) have a higher affinity to the fungal than the human enzyme system and are assumed to induce less side-effects 26, 27, 31, these drugs may also compromise the adrenal function when given in high doses and over long periods of time 25.
The very low plasma ACTH levels in all the patients with adrenal insufficiency indicate that reduced metabolism of budesonide may be the primary problem. High levels of plasma-ACTH in response to low plasma-cortisol levels should have been measured if itraconazole had only significantly suppressed steroidogenesis. After itraconazole withdrawal, the tetracosactid-stimulated cortisol level initially only reached subnormal levels. Itraconazole, given its long half-life in plasma (days), specific kinetic properties and high accumulation in various tissues 32, 33 may act intracellularly for an extended period of time, which may explain why the suppression of the axis persists for a long period after treatment withdrawal. ACTH production reached normal levels earlier which may reflect decreased serum budesonide and thus, re-establishment of an intact pituitary-adrenal negative feedback mechanism.
Cushing's syndrome has been reported previously in patients treated with orally administered glucocorticoids in combination with itraconazole 34, 35. Case studies of Cushing's syndrome and adrenal suppression due to treatment with inhaled steroids have also been reported 36, 37. Thus, daily doses of 800–4,000 µg beclomethasone dipropionate (BDP) (mean 1465 µg·day−1) were reported to cause a moderate and dose-dependent adrenocortical suppression, but as assessed by a low-dose ACTH test, lower BDP or budesonide doses (250–1058 µg·m−2, mean 507 µg·m−2) also appear to impair adrenal function 37–39. The endogenous cortisol production may decrease by ∼20% in predisposed individuals treated with budesonide in doses of 800 µg twice daily 40, 41. However, the authors have shown previously that budesonide used long-term as an anti-inflammatory agent in doses of 1,600 µg daily in CF patients does not suppress adrenal function 14. Hydrocortisone metabolism may also be impaired, as seen in the patients with Cushingoid symptoms during substitution treatment at standard doses, because the drug is metabolised by the same pathways as budesonide.
The interaction between itraconazole and budesonide, inducing high systemic budesonide levels, may in part explain the reported ability to reduce the glucocorticoid dose 6, 9, 10, 42, 43. If this is the case, the use of itraconazole may “spare” the administered dose of steroids but its effect, or side-effects, remain.
Some authors have suggested the possibility of drug-induced Conn's syndrome during itraconazole treatment due to the presence of hypokalemia, oedema and hypertension 25, 44–46. In the present study normal plasma-renin levels indicate that no involvement of mineralocorticoid secretion was present in any of the patients. Ketoconazole has been associated with a number of gonadal adverse effects, i.e. depression of testosterone synthesis, gynecomastia and impotence 47–49. However, suppression of gonadal steroids was not observed in any patient in the present study. Itraconazole has been reported to have a greater sensitivity for 11β-hydroxylase and a relative sparing of the C17-20 lyase enzyme activity (and androgen activity) 25, 26, 34, which may explain the finding of adrenal but no gonadal suppression.
As clarithromycin, a macrolide antibiotic administered for atypical mycobacteria in patients with CF, has an inhibitory effect on CYP3A and may interfere with the metabolism of budesonide 50–52, some caution is advisable when it is used in combination with itraconazole. Furthermore, a bidirectional interaction between clarithromycin and itraconazole through their effect on CYP 3A4 activity may result in increased levels of both 53.
Recent studies have recommended itraconazole as an effective and steroid-sparing treatment of ABPA 6, 9, 10, 42, 43. In some patients, worsening of the clinical symptoms of ABPA and an increase in specific IgG subclass antibodies to A. fumigatus resulted in re-administration of itraconazole. Suppression of cortisol production was not observed within 2–3 months after re-start of itraconazole treatment in these patients.
Adrenal suppression only seems to be a risk in patients treated with budesonide in combination with itraconazole, yet it did not include all patients on combination therapy despite a similar accumulated dose and duration of treatment. Whether the side-effects are due to high systemic steroid concentrations, absorption influenced by the degree of inflammation and perfusion, dose and duration of treatment or individual receptor susceptibility is at present unknown. In addition, the amount of CYP3A4 in an individual patient, which varies considerably, may correlate with the magnitude of inhibition and thereby the possible effect of a given inhibitor. Finally, concomitant administration of other drugs may induce or inhibit CYP 3A4 activity.
To conclude, care should be taken when itraconazole or other potent CYP3A inhibitors are prescribed concomitantly with steroids including inhaled steroids such as budesonide. The authors recommend that tests for adrenal insufficiency are performed at regular intervals in such patients. In case of adrenal insufficiency, substitution with hydrocortisone needs additional careful monitoring as metabolism of hydrocortisone may also be compromised.
- Received May 29, 2001.
- Accepted January 17, 2002.
- © ERS Journals Ltd
References









