





Abstract
Neurokinin (NK) A causes airway narrowing in patients with asthma through direct and indirect mechanisms. The effects of the inhaled glucocorticosteroid fluticasone propionate (FP) on the bronchial responsiveness to NKA and methacholine were studied.
Patients (n=11) with mild asthma participated in a randomized, double-blind, placebo-controlled crossover trial. FP (500 µg b.i.d) or matched placebo was administered via DiskhalerTM for 14 days. Bronchial challenges were performed on days 1 and 13 (methacholine) and 0 and 14 (NKA) for each treatment period.
At the active treatment period, the mean log2 provocative concentration causing a 20% fall in the forced expiratory volume in one second (PC20)±sem for NKA was −12.72±0.63 at the beginning and −9.77±0.49 at the end of the period (p<0.0001), while under placebo, it was −12.16±0.82 and −12.19±0.51 respectively (ns). At the active treatment period, the mean log2 PC20 for methacholine was −5.25±0.40 at the beginning and −4.22±0.31 at the end of the period (p=0.012), while under placebo, it was −5.47±0.47 and −5.24±0.42 respectively (ns). The reduction in response to NKA was significantly larger than that for methacholine.
A 2-week course of an inhaled steroid reduces bronchial responsiveness to neurokinin A, an effect more pronounced than the reduction in bronchial responsiveness to methacholine.
The present study was supported by GlaxoWellcome plc, UK.
The tachykinins, substance P and neurokinin (NK) A are potential mediators of asthma. They are produced by sensory airway nerves and nonneural cells, such as endothelial cells, eosinophils, macrophages, and dendritic cells. Substance P and NKA have potent effects on the bronchomotor tone, airway secretion, bronchial circulation (vasodilatation and microvascular leakage) as well as on inflammatory and immune cells 1, 2.
Patients with asthma are hyperresponsive to inhaled substance P and NKA 3, 4. In vitro studies have revealed that NKA contracts airway smooth muscle directly, by stimulation of tachykinin (NK2) receptors 5. In patients with asthma the inhalation of tachykinins causes a dose-dependent airway narrowing which is largely preventable by inhalation of nedocromil sodium. Hence inhaled tachykinins act mainly as indirect bronchoconstrictor stimuli 6, 7. The indirect airway-narrowing effect of the tachykinins is mediated by tachykinin NK1 receptors 8–10.
Glucocorticoids may enhance the expression of neutral endopeptidase, which is the major degrading enzyme of the tachykinins in the airways 11, 12. Moreover, glucocorticoids are able to reduce the expression of the tachykinin NK1 and NK2 receptors 13, 14. The effect of inhaled steroids on the bronchial responsiveness for direct stimuli such as histamine or methacholine is well documented 15. It is not known whether steroids can affect the bronchoconstrictor response to substance P or NKA. The aim of the present trial was to study the effects of inhaled steroids on NKA-induced airway narrowing. Moreover the authors wanted to compare the eventual changes in bronchial responsiveness to NKA with those to methacholine. Therefore, airway responsiveness to NKA and methacholine was assessed prior to and following a 2-week course of inhaled fluticasone propionate (FP), 1000 µg ·day−1, in a group of patients with mild-to-moderate asthma.
Methods
Patients
Adult subjects with stable mild-to-moderate asthma 16 were recruited for the trial. They had to be nonsmokers or exsmokers (defined as having a cumulative smoking history of ⩽5 pack-yrs, and having ceased smoking for at least 1 yr prior to the start of the trial). Females of childbearing potential had to use reliable contraceptives, and pregnant or lactating women were excluded from participation. No relevant concomitant diseases were present. The only treatment allowed during the study consisted of inhaled salbutamol (VentolinTM; GlaxoWellcome, Stockley Park, UK) as reliever medication. Patient nos. 4, 6 and 10 were on inhaled steroids (budesonide 400 µg·day−1, budesonide 800 µg·day−1 and beclomethasone dipropionate 1000 µg·day−1, respectively) and discontinued its use at least 4 weeks prior to the first screening visit. Their morning baseline forced expiratory volume in one second (FEV1) was at least 70% of the predicted and the provocative concentration causing a 20% fall in the forced expiratory volume in one second (PC20) at the screening methacholine and NKA challenges was <8 mg·mL−1 and 1.0×10−6 mol·mL−1, respectively. No patient was studied within 4 weeks of an upper or lower respiratory tract infection or exacerbation of asthma.
The trial protocol was approved by the ethical committee of the Ghent University Hospital. All participants gave their written informed consent.
Study design
The study was of a randomized, double-blind, placebo-controlled, two-period crossover design. On screening day 1 (visit one), the patients underwent a methacholine challenge. The baseline FEV1 prior to each subsequent challenge had to be within 15% of the screening baseline FEV1 obtained at visit one. Short-acting β2-agonists and caffeine-containing foods and beverages had to be withheld for at least 10 h before each challenge. A NKA challenge on screening day 2 (visit two) was performed 24–72 h later. Study-period one commenced within 10 days after visit two; firstly, a methacholine and a neurokinin-A challenge was performed on days 1 (visit three) and 0 (visit four), respectively. At visit four (day 0), the study medication was handed over to the participants, who started using it from day 1 and for the following 14 days. The study medication consisted of FP (FlixotideTM; GlaxoWellcome, Stockley Park, UK), 2×500 µg·day−1 or matched placebo, which was inhaled as a dry powder from a DiskhalerTM (GlaxoWellcome, Stockley Park, UK). The morning dose was inhaled between 06.00–08.00 h and the evening dose between 20.00–22.00 h. Following each dose, the mouth was rinsed with tap water, following which the water was spat out. On days 13 (visit five) and 14 (visit six) respectively, the last 2 days of the treatment period, methacholine and NKA challenges were repeated. Following treatment-period one, there was a washout period of 4 weeks±5 days, counted from day 15, the first day without study medication. After this, the patients crossed over to the other medication in study-period two, which was identical to period one. As in period one, methacholine and neurokinin-A challenges were performed on separate, consecutive days at the beginning (visits seven and eight) and the end (visits nine and ten) of this second treatment period, respectively.
Pulmonary function testing
Pulmonary function tests were performed using a water-sealed spirometer (Pulmonet III; Sensormedics, Bilthoven, the Netherlands), in accordance with the European Respiratory Society guidelines 17. The highest value of three consecutive manoeuvres was accepted for evaluation at each performance. Spirometry was performed with the patient in a sitting position, the nose occluded by a clip. The lung-function technician and the spirometer were the same throughout the study.
Bronchial challenge tests
The methacholine challenge was performed by inhaling doubling concentrations of methacholine from a “Wiesbadener Doppel Inhalator” (Wiesbadener Inhalatoren-Vertrieb, Wiesbaden, Germany), until the FEV1 fell by >20% of the postdiluent baseline FEV1 of that day, according to the method of Cockcroft et al. 18. The methacholine diluent (phosphate-buffered saline (PBS)) and the subsequent methacholine concentrations (2, 4, 8, 16 and 32 mg·mL−1) were inhaled during 2 min of quiet tidal breathing, in a sitting position, the nose being occluded by a clip. Measurements of FEV1 were performed at 30 and 90 s after the inhalation of each concentration. The nebulizations of the different concentrations were initiated at 5-min intervals.
NKA challenge was performed by inhaling increasing concentrations of NKA, as described previously 10. Prior to each NKA challenge, baseline FEV1 was determined. The subjects then inhaled the NKA diluent and FEV1 was measured 3 and 7 min after the start of the inhalation, the lowest value of both being considered as the postdiluent baseline FEV1. The actual NKA challenge was performed provided the FEV1 did not fall by >10% after inhaling diluent. During the challenge, increasing concentrations of NKA (3.3×10−9, 1.0×10−8, 3.3×10−8, 1.0×10−7, 3.3×10−7 and 1.0×10−6 mol·mL−1) were inhaled until FEV1 fell by ≥20% of its respective postdiluent baseline value.
NKA was obtained from Peninsula (St. Helens, UK) and was diluted in saline containing 1% human serum albumin (Behringwerke AG, Marburg, Germany). The dilutions of NKA were freshly prepared on the morning of the challenge and kept on ice until nebulization. The aerosols were produced using a Mallinckrodt jet nebulizer 19. A collapsible 30-L plastic bag, which served as a drying chamber, was filled with nitrogen (N2) gas. Then, 0.5 mL of diluent or each subsequent NKA concentration was sprayed by compressed N2 (4 bar) in 1 min±10 s into the drying chamber, in which the droplets rapidly evaporated to dry particles. Finally, the patient inhaled the aerosol from the bag during 2 min of quiet tidal breathing through a three-way valve and a mouthpiece, until collapse of the bag. Supplementary oxygen (at a flow of 4 L·min−1, inspiratory oxygen fraction: 0.995) was supplied into the mouthpiece. The patients performed the inhalation in a sitting position, the nose being occluded by a clip. Pulmonary function measurements were performed at 3 and 7 min after the start of the inhalation of each concentration. The nebulizations of the different concentrations were initiated at 10-min intervals.
All methacholine and NKA challenges were performed in the morning, starting between 08.00–09.00 h. After having completed the challenge, the patients were allowed to leave the dept, on the condition that their FEV1 had returned to within 10% of their prechallenge FEV1 on that day.
Statistical analysis
The morning FEV1 prediluent baseline values on the different visits were compared by means of an analysis of variance (ANOVA), to test for treatment and carry-over effect.
For the data analysis of the airway responsiveness, the values of PC20 for methacholine and NKA were converted into moles and then log2 transformed, in order to obtain doubling steps. A PC20 value of 64 mg·mL−1 for methacholine (one doubling-concentration higher than the highest concentration tested), or of 3.3×10−6 mol·mL−1 for NKA (a 0.5 log10 higher concentration than the highest concentration tested) was attributed in those cases where the desired fall in FEV1 was not obtained.
The effect of a treatment on the airway responsiveness was calculated by pairwise comparison of the log2 PC20 values at the beginning and end of the respective treatment period, using a paired t-test. This was carried out separately for the methacholine and NKA challenge results.
In order to compare the FP-induced changes in airway responsiveness between NKA and methacholine challenges, the difference between the log2 PC20 value at the end and the beginning of the FP period, hereafter called Δlog2 PC20 (PostFP-PreFP), was calculated for NKA and methacholine separately. The changes obtained for NKA and methacholine (their respective Δlog2 PC20 (PostFP-preFP)), were then compared, by means of a paired t-test.
For all analyses, a p-value of <0.05 was considered significant. Data are expressed as mean±sem.
Results
Patient characteristics at screening
Eleven patients, aged 18−49 yrs (mean: 27.5 yrs), 7 females and 4 males, participated in the trial. Their mean±sem baseline FEV1 was 3.20±0.16 L or 88.0±3.44% of the predicted. Their mean screening log2 PC20 for methacholine was −5.96±0.20, while their mean screening log2 PC20 for NKA was −12.71±0.63 (table 1⇓).
Patient characteristics at screening
The effect of treatment on the morning baseline forced expiratory volume in one second values
FP significantly increased the baseline prechallenge FEV1 values, compared to placebo; this was the case for the premethacholine challenge baselines (p=0.006) as well as for the pre-NKA challenge baselines (p=0.027) (table 2⇓). Neither the baseline FEV1, nor the bronchial responsiveness to NKA or to methacholine at the beginning of each treatment period were different, so that a carry-over effect could be ruled out.
Evolution of the morning baseline prechallenge forced expiratory volume in one second during the trial
The effect of fluticasone propionate on bronchial hyperresponsiveness to neurokinin A
At the active treatment period, the mean log2 PC20 for NKA was −12.72±0.63 at the beginning and −9.77±0.49 at the end of the period (p<0.0001). The mean log2 PC20 for NKA was −12.16±0.82 at the beginning and −12.19±0.51 at the end of the placebo period (ns) (fig. 1⇓).
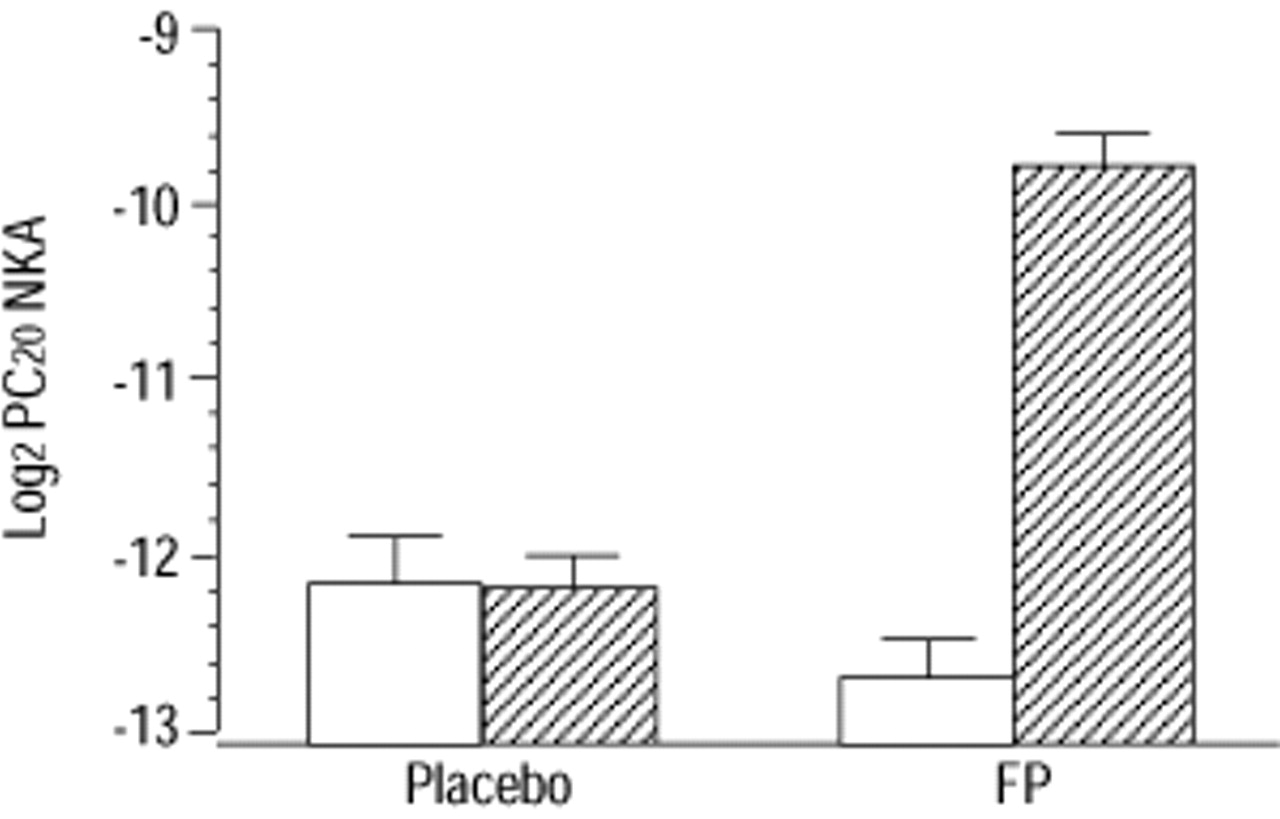
Log2 provocative concentration causing a 20% fall in the forced expiratory volume in one second (PC20) for neurokinin A (NKA) before (□) and at the end of both treatment periods (└) (data are presented as mean±sem; n=11). Post- versus preplacebo: ns; post- versus prefluticasone propionate (FP): p<0.0001.
The effect of fluticasone propionate on bronchial hyperresponsiveness to methacholine
At the active treatment period, the mean log2 PC20 for methacholine was −5.25±0.40 at the beginning and −4.22±0.31 at the end of the period (p=0.012). The mean log2 PC20 methacholine was −5.47±0.47 at the beginning of the placebo period and −5.24±0.42 at the end (ns) (fig. 2⇓).

{kind=link}
{kind=link}
Log2 provocative concentration causing a 20% fall in the forced expiratory volume in one second (PC20) for methacholine (M) before (□) and at the end of both treatment periods (└) (data are presented as mean±sem; n=11). Post- versus preplacebo: ns; post- versus prefluticasone propionate (FP): p=0.012.
Comparison of the fluticasone propionate-induced changes in bronchial hyperresponsiveness between neurokinin A and methacholine challenges
The Δlog2 PC20 (PostFP-PreFP) was 2.90±0.47 for the NKA challenge, and 1.03±0.34 for the methacholine challenge (p=0.004).
Discussion
In this study a 2-week treatment with the inhaled steroid FP reduced bronchial responsiveness to NKA in patients with asthma. The reduction in bronchial responsiveness to NKA was larger than the reduction in responsiveness to methacholine.
The bronchoconstrictor effect of NKA in asthma is well documented 3, 4. Although NKA contracts airway smooth muscle directly 5 the in vivo bronchoconstrictor effect of inhaled NKA and the related tachykinin substance P are mainly due to indirect airway-narrowing effects such as stimulation of inflammatory cells 6, 7, stimulation of cholinergic nerves 20, 21, and induction of plasma protein extravasation 22. The effects of inhaled tachykinins are potentiated by inhibitors of the degrading enzyme neutral endopeptidase (NEP) 4.
This study clearly demonstrated that treatment of patients with mild asthma for 14 days with an inhaled steroid reduced the bronchial responsiveness to NKA. Glucocorticosteroids have a very broad spectrum of activity that might explain their therapeutic activity in asthma 23. Glucocorticosteroids can specifically interfere with the mechanisms involved in the airway response to inhaled tachykinins, by affecting expression of degrading enzymes or by affecting the presence and/or expression of tachykinin receptors. Indeed, several authors have shown that glucocorticosteroids enhance the expression of NEP, the major neuropeptide-degrading enzyme in the airways 11, 12. Glucocorticosteroids may also affect the number of tachykinin receptors in the airways. They have been shown to reduce tachykinin NK1 13 and NK2 14 receptor gene expression. Moreover, by decreasing the number of inflammatory cells carrying the tachykinin NK1 receptor, they could reduce the airway narrowing effects of NKA and substance P 24. These known effects of glucocorticosteroids on tachykinin action and degradation can at least partially explain the observed decrease in bronchial responsiveness to NKA. Inhaled steroids reduce the inflammatory-cell infiltrate in patients with asthma 25, and by doing so, less cells, for instance mast cells, are available in the airways for interaction with the inhaled tachykinin and for the development of bronchoconstriction.
High doses of inhaled steroids decrease bronchial responsiveness to methacholine and histamine within 2−8 weeks in steroid-naive mild asthmatics; however their effect is limited 26, a finding which was again confirmed in this study (fig. 2⇑). The results of the present study indicate that steroid treatment improved the bronchial responsiveness to NKA to a larger extent than the bronchial responsiveness to methacholine. Indeed treatment with FP for 2 weeks caused a larger shift in responsiveness for NKA than methacholine. Inhaled steroids have previously been shown to have more of an effect on the response to indirect stimuli such as adenosine monophosphate 27, 28, hypertonic saline 29 and exercise 30, 31, than to direct stimuli such as histamine or methacholine. The present findings demonstrated that this was also the case for the indirect bronchoconstrictor agonist NKA.
To conclude, the study demonstrated, for the first time that inhaled steroids are able to reduce the bronchial responsiveness to the tachykinin neurokinin A, an effect that was already observed after 2 weeks of treatment. The reduction in bronchial responsiveness to neurokinin A was more pronounced than that for methacholine.
Acknowledgments
The authors would like to thank V. Collart for the lung function measurements and G. Van der Reysen for statistical assistance.
- Received July 25, 2001.
- Accepted January 19, 2002.
- © ERS Journals Ltd
References









