





Abstract
Although some asthmatic children seem to recover from their asthma, 30–80% develop asthma again in later life. The underlying risk factors are unknown. The hypothesis for this study was that children with apparently outgrown asthma would have underlying airway inflammation.
Nonbronchoscopic bronchoalveolar lavage was performed on normal children (n=35) and children who had wheezed previously (n=35).
Eosinophils were raised in the lavage fluid of atopic children who had apparently outgrown asthma (median (interquartile range) 0.36 (0.05–0.74) compared to controls 0.10 (0–0.18), p=0.002). There was no relationship between length of remission and degree of airways eosinophilia.
Thus, there is persistent airways inflammation in some children with outgrown asthma and this may be a risk factor for future relapse.
This study was supported by the National Asthma Campaign, UK and the Research and Development Office for Northern Ireland.
It is well recognized that children with asthma often enter remission, commonly in the second decade of life, and seem to outgrow their asthma 1, 2. Studies have shown that 30–80% of previous asthmatics may relapse in later life 1–5. Eosinophilic airways inflammation plays an important role in asthma and the current thinking is that undertreatment of airways inflammation may lead to long-term structural changes such as airways remodelling and irreversible airflow obstruction 6. While studies have documented pulmonary function abnormalities and bronchial hyperresponsiveness in previous childhood asthmatics 2, 7–11, to the best of the authors' knowledge there are no reports of persistent airways inflammation in children who have outgrown asthma. This study examined direct measures of airways inflammation in children who had had wheezing episodes in the past.
Methods
Seventy children (35 with previous wheeze (PW) and 35 nonatopic normal controls (of similar age and sex distribution)) attending The Royal Belfast Hospital for Sick Children for elective surgical procedures were recruited. Bronchoalveolar lavage (BAL) was performed using a non-bronchoscopic technique immediately after induction of anaesthesia, as described previously 12. Parental written informed consent was obtained and the study was approved by the Research Ethics Committee. BAL fluid was centrifuged (200×g, 5 min, 4°C) and cytospin preparations produced using a modified coverslip method 12. Cells were stained with Diff-Quik® (Baxter Healthcare Ltd, Compton, UK) for differential cell counting (minimum of 1,000 cells counted) and with Toluidine Blue for mast-cell counting (2,000–5,000 cells counted).
PW was defined as episodes of wheezing in the past, but no symptoms for at least 12 months and currently on no medication. After the administration of a detailed respiratory/atopy questionnaire 12, the PW group was subdivided into atopic asthma outgrown (AAO) and viral wheeze outgrown (VWO) on the basis of atopic status and clinical history. Atopy was defined as in previous publications 12, 13 as either a personal history of atopic disease, or two first-degree relatives with atopic disease or a raised total serum immunoglobulin-E (IgE). None of the control group were atopic. The Mann-Whitney U- and Kruskal-Wallis (with multiple comparisons adjustment) tests were used to compare BAL eosinophil percentages between subgroups. Spearman's correlations were performed to examine the relationship between length of remission and BAL eosinophil percentage.
Results
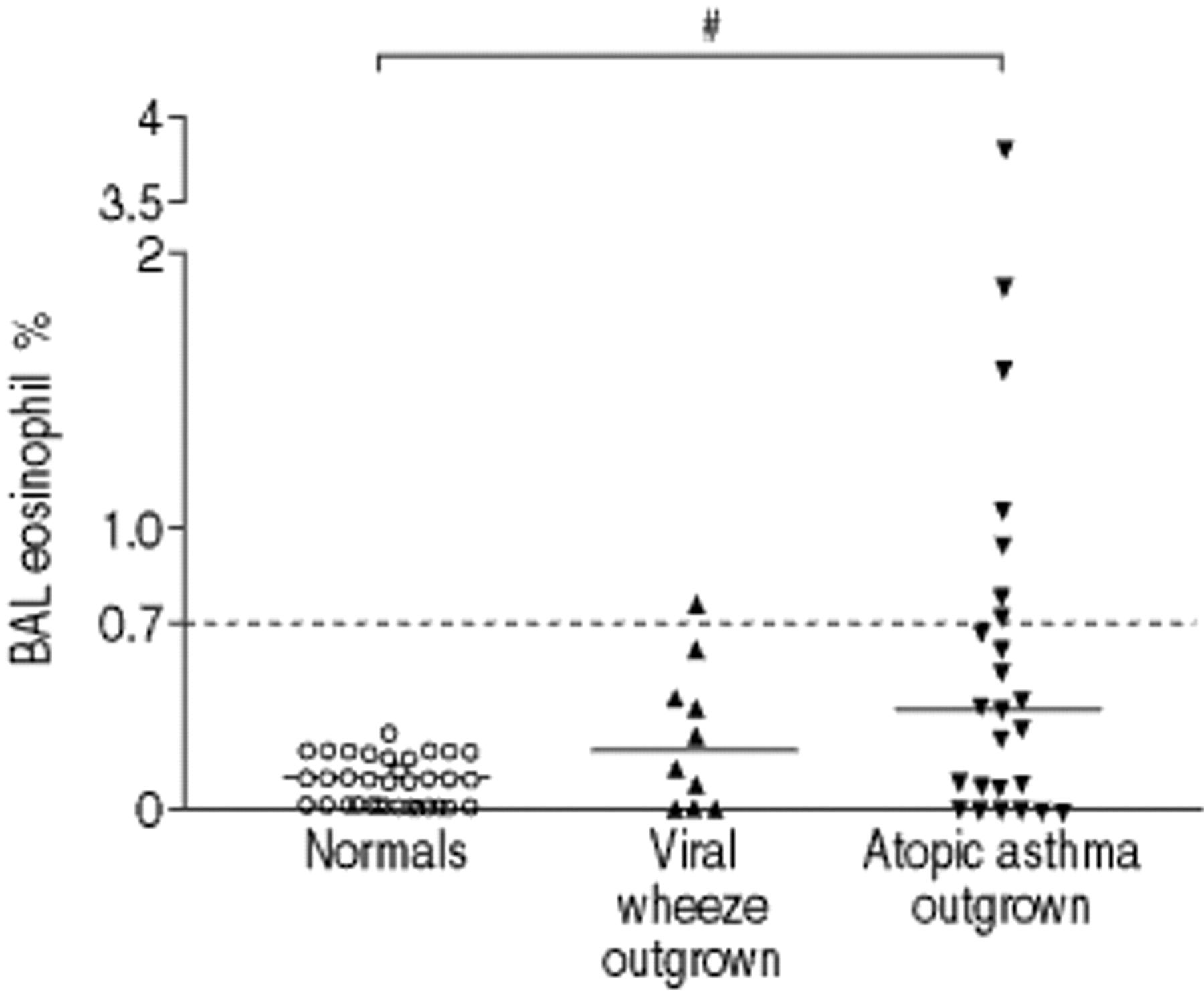
The patient characteristics and BAL data are shown for the three groups in table 1⇓. The PW group had significantly higher eosinophil percentages (median % (interquartile range): 0.3 (0–0.64)) when compared to the normal control group (0.1 (0–0.18), p=0.002). The median eosinophil percentage was higher in the AAO group compared with the normals (difference in median 0.27, 95% confidence interval 0.09–0.49, p=0.002, fig. 1⇓). Three of the six children in the AAO group with elevated eosinophils had a raised IgE and a personal history of allergic disease at the time of examination. Of the other three, one child had atopic eczema and the two others had a strong family history of atopy. Nineteen children in the AAO group did not have raised eosinophils and five of these subjects had an elevated IgE level. Three of these five subjects had a personal history of allergic disease compared with six of the remaining 12. There were no differences between the groups for any other cell type in BAL. There was no correlation between duration of remission in the AAO group and degree of airway eosinophilia (r=0.12, p=0.6).

{kind=link}
Kruskal-Wallis test (with multiple comparisons) on bronchoalveolar lavage (BAL) eosinophil % for normals, viral wheeze outgrown and atopic asthma outgrown. The value marked “0.7” (dashed line) corresponds to the previously defined upper limit of normal BAL eosinophil % 12, and the solid lines represent median values. #: p=0.002.
Patient characteristics, remission length and bronchoalveolar lavage (BAL) cellular data
Discussion
In this study the authors have shown that children with previous episodes of wheezing have elevated numbers of eosinophils in their airways compared to normal controls. The only significant difference was between the AAO group and normals. The presence of persistent raised BAL eosinophil percentages in children who have outgrown asthma has not been documented previously. In the AAO children, there were no clinical differences between those with elevated eosinophils and those without. Gruber et al. 7 have shown that atopic asthmatic children in remission have evidence of pulmonary function abnormalities and bronchial hyperresponsiveness. However, it was not clear whether these findings were suggestive of continuing airways inflammation, or merely indicative of previous airway damage. The findings of the present study lend support to the former hypothesis. Unfortunately, as the children in this study were attending for elective surgical procedures, the authors were unable to obtain ethical permission for quantification of bronchial hyperresponsiveness or skin-prick testing.
Nonatopic children who had wheezed previously, only in association with upper respiratory tract infections were classified as VWO. These children did not have raised BAL eosinophil percentages when compared with normal controls. This would be in keeping with the present understanding of viral wheeze being a condition usually limited to early childhood and carrying an excellent long-term prognosis 14, 15. A previous study from this research group has also shown that there is no evidence of eosinophilic inflammation in current viral wheezers 13, and the values for all other cell types in the VWO and AAO groups were similar to values published previously 12, 13.
The possibility that the raised BAL eosinophil percentages may be related to the length of remission was considered. However, as the results show, there was no relationship between these two variables, which suggests that these findings are not simply reflecting the gradual subsidence of airways inflammation, as remission increases in duration.
It is accepted that a number of children who have apparently “outgrown” their asthma will relapse in later life. Asthma disease severity, degree of airflow obstruction and bronchial hyperresponsiveness are thought to be potential predictors of the persistence of asthma symptoms or future relapse of asthma 3. It seems reasonable to also consider that persistent airways inflammation may be a risk factor that could predict those patients at risk of future relapse. Van den Toorn et al. 16 have shown that adolescents in asthma remission have elevated levels of exhaled nitric oxide (ENO), which corresponds to persistent bronchial hyperresponsiveness. ENO is thought to be a noninvasive marker of airways inflammation and further prospective studies are required to examine the possibility that ENO corresponds with persistent airways inflammation, and hence, may be a noninvasive predictor of future asthma relapse. This study was a case-control study, which carries its own limitations. In an ideal situation, a group of asthmatics would have been followed-up prospectively and had BAL performed at regular intervals, however, for ethical reasons this was not possible. Future work may address this issue by follow-up of children using induced sputum or possibly ENO measurements. The children in this study who had outgrown their asthma had a median age of 7.3 yrs, which is younger than the traditionally perceived age for outgrowing asthma, that of the early teenage years. This may reflect that the children in this study had mild asthma, which makes the presence of persisting inflammation in some of them more noteworthy.
In a previous study, the authors have shown that the upper limit of normal for BAL eosinophil percentage is 0.7% 12. The finding that eosinophils in BAL are elevated in some children (24% above normal range) who no longer wheeze, would suggest other components of inflammation need to be present for symptoms to persist. Recent studies have highlighted the potential contribution of neutrophils in asthmatic inflammation 17, 18. The present study however, does not demonstrate any difference in BAL neutrophil percentage in previous asthmatics compared with normal controls. In a previous study from this group, neutrophilic airways inflammation was only found in children with chronic nonspecific cough 19. Obase et al. 20 studied induced sputum from symptom-free young adults with a previous history of childhood asthma. They found elevated sputum eosinophils, eosinophil cationic protein and tumour necrosis factor-α in some of these subjects compared to normal controls, but normal levels of granulocyte-macrophage colony-stimulating factor (a cytokine involved in eosinophil activation) when compared to symptomatic asthmatics 20. Further study of this outgrown asthma group may help determine what has been “switched off” in the asthmatic inflammatory process.
In conclusion, the authors have shown that eosinophilic airways inflammation may persist in atopic children who have apparently outgrown asthma, and it is speculated that this may have implications for the risk of future relapse in these individuals.
- Received September 6, 2001.
- Accepted October 8, 2001.
- © ERS Journals Ltd
References









