





Figures
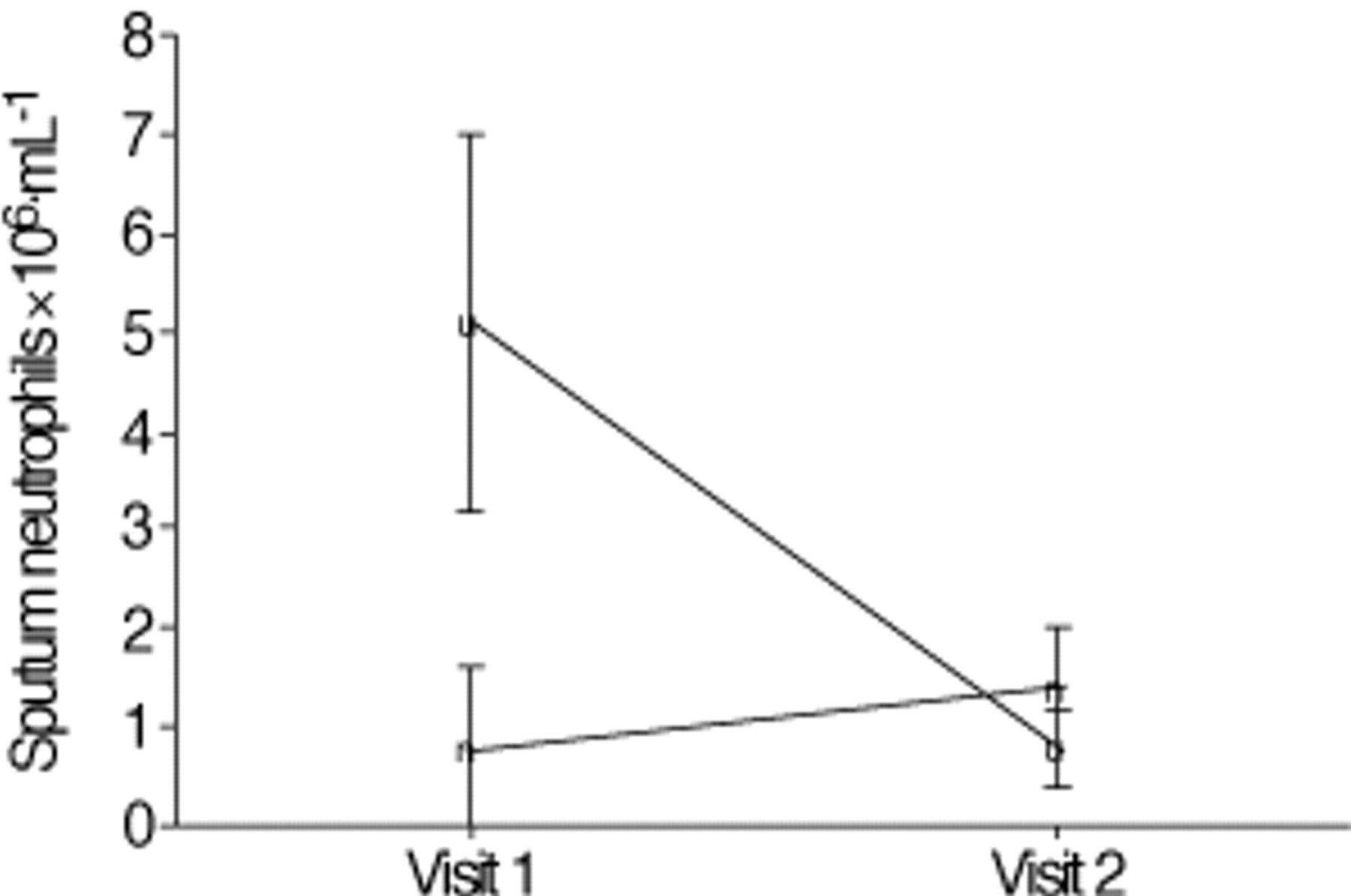
- Fig. 1.—
Induced sputum neutrophils (measured as number of cells ×106·mL−1) in subjects with acute asthma (Visit 1) and upon recovery Visit 2). The points represent the geometric mean±1 sem. Subjects with infective asthma (♦) had higher sputum neutrophils at Visit 1 compared to noninfective asthma (▪) (p=0.02). By Visit 2, sputum neutrophils had fallen in subjects with infective asthma (p=0.04), but no significant change was seen in subjects with noninfective asthma.
- Fig. 2.—
Logistic regression model to predict variables associated with increased sputum neutrophils. An increase in sputum neutrophils was defined as >3.1×106·mL−1. The points represent the odds ratio (OR) and their 95% confidence intervals. ═: the line of unity. The presence of infection and male sex independently predicted the presence of elevated sputum neutrophils at Visit 1.
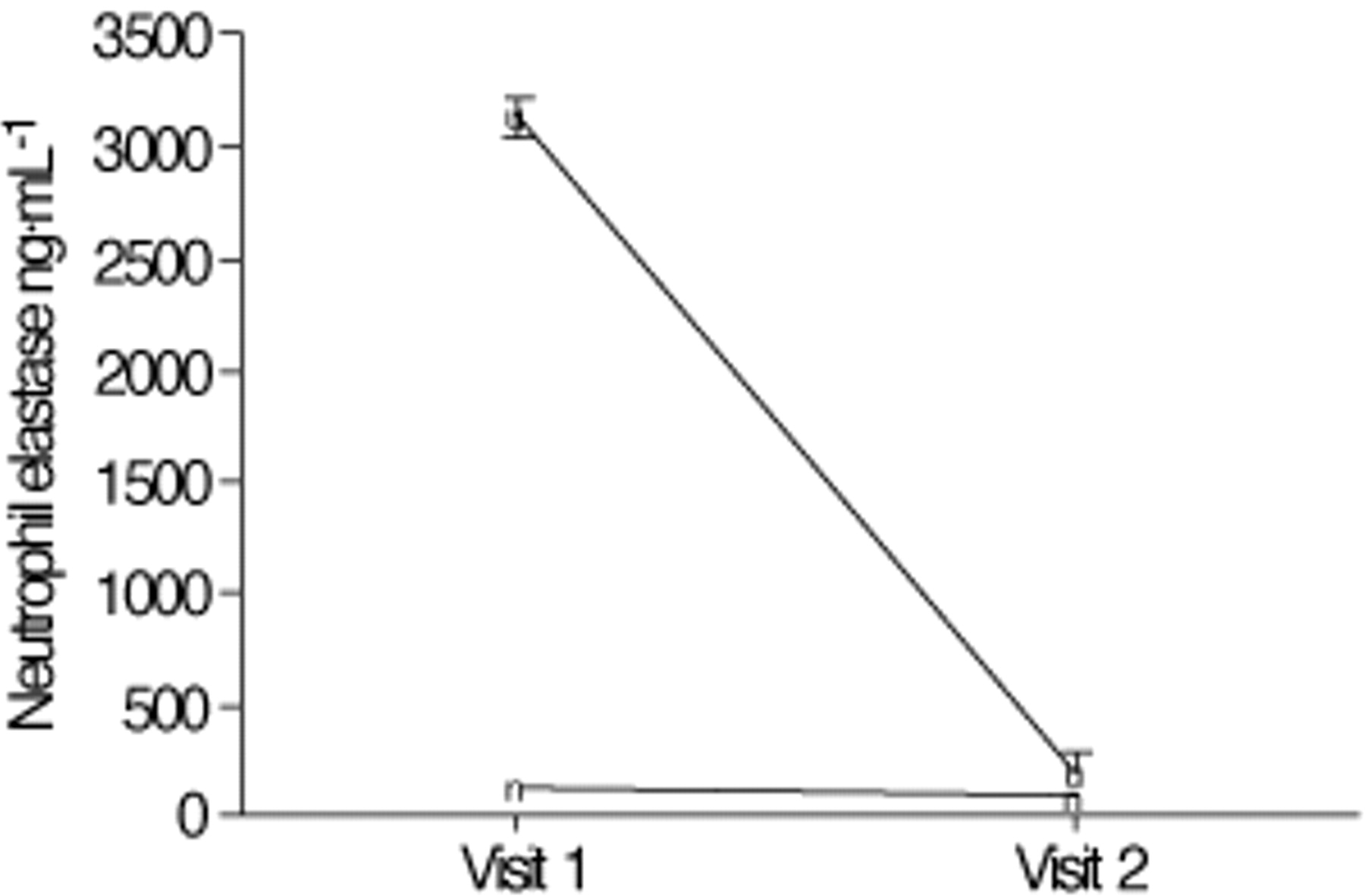
- Fig. 3.—
Sputum neutrophil elastase (ng·mL−1) in subjects with acute asthma (Visit 1) and upon recovery (Visit 2). The points represent the geometric mean±1 sem. Subjects with infective asthma (♦) had higher sputum neutrophil elastase at Visit 1 compared to noninfective asthma (▪) (p<0.05). By Visit 2, this had fallen in subjects with infective asthma (p<0.05), but no significant change was seen in subjects with noninfective asthma.
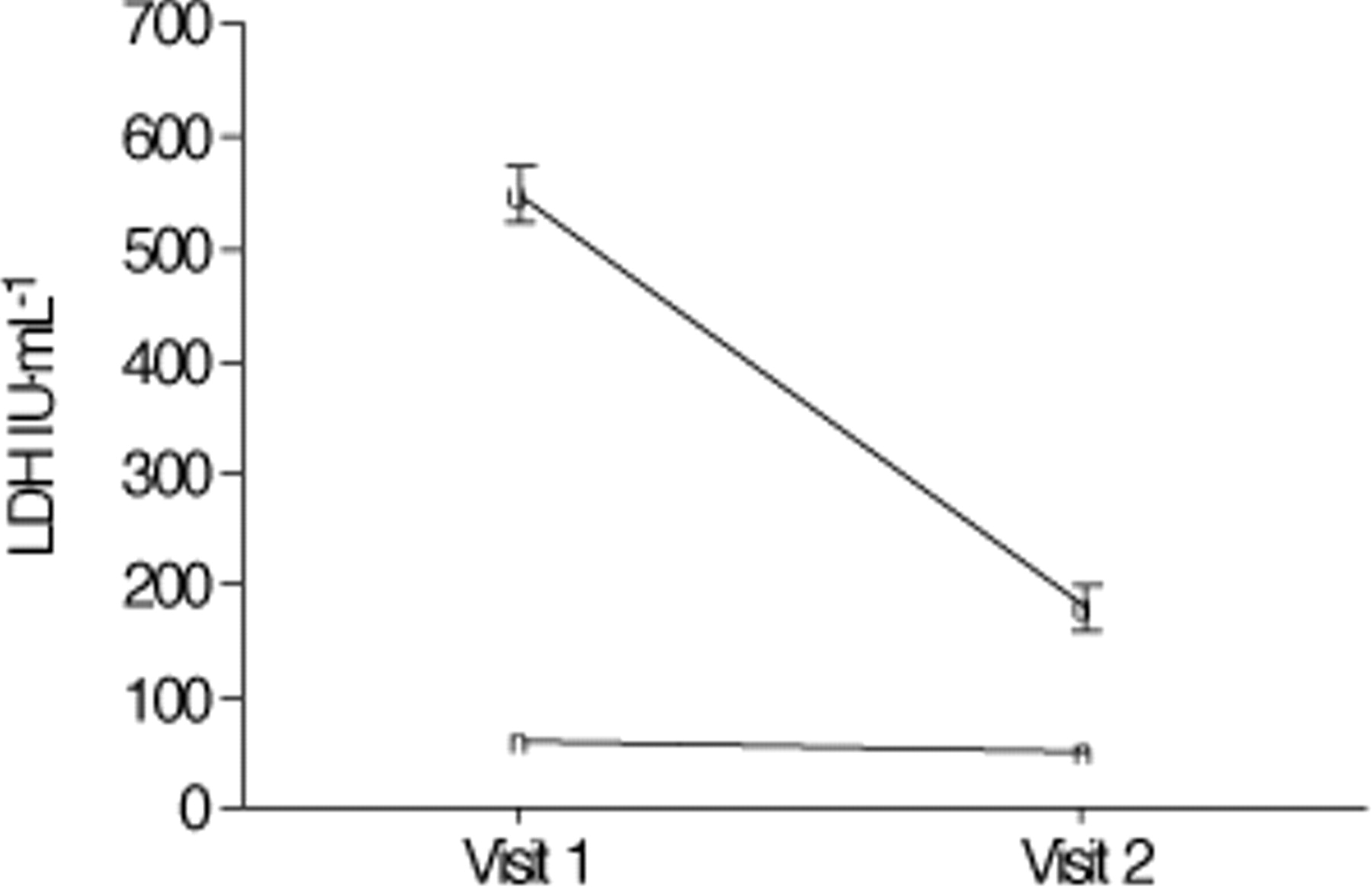
- Fig. 4.—
Mean sputum lactate dehydrogenase (LDH) in subjects at Visit 1 and Visit 2. The points represent the geometric mean±1 sem. Subjects with infective asthma (♦) had higher sputum LDH at Visit 1 compared to noninfective asthma (▪) (p<0.05). By Visit 2, sputum LDH had fallen significantly in all subjects (p<0.05). IU: international units.
- Fig. 5.—
Sputum lactate dehydrogenase (LDH) isoenzymes expressed as a per cent of the total LDH activity at the initial visit. Data are presented as medians and interquartile ranges.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- Table 1—
Clinical characteristics
Noninfective Infective Analysis Subjects n 12 37 NA Male sex 3 (25) 15 (41) p=0.3 Age yrs 37.3±16.1 40.5±17.9 p=0.2 Smokers 3 (25) 2 (17) p=0.2 Atopy 8 (67) 21 (57) p=0.4 Aas score 7 4.1±1.0 3.9±1.4 p=0.2 Maintenance ICS¶, µg BDP·day−1 1475±861 1606±826 p=0.8 Admitted 4 (33) 10 (83)* p<0.01# Admitted to ICU 0 2 (17) p=0.2# Length of stay in days 0.7±1.4 4.7 (5.9)* p=0.02 Acute FEV1 % pred 70.4±24 45.3±31.7* p=0.04 FEV1 % pred at follow-up 86.5±23.1 70.1±31.2* p=0.04 Maintenance ICS at follow-up, µg BDP·day−1 1523±806 1865±886 p=0.5 Data are presented as n (%) or mean±sd unless otherwise stated
ICS: inhaled corticosteroids
BDP: beclomethasone dipropionate
ICU: intensive care unit
FEV1: forced expiratory volume in one second
NA: not applicable
¶: ICS dose expressed as total daily dose of BDP in µg·day−1, where 1 µg BDP equals 1 µg budesonide and 0.5 µg fluticasone
*: p<0.05, significantly different from those with noninfective acute asthma
#: analysis using Chi-squared test
- Table 2—
Sputum cell counts in acute asthma
Visit 1 Visit 2 Noninfective Infective Noninfective Infective Nebulizer time min 2.6±1.7 2.8±1.9 4.8±1.6 4.9±1.6 TCC×106·mL−1 2.8±2.9 8.3±2.5* 3.3±2.2 2.2±1.5*** Neutrophils×106·mL−1 0.8±5 5.1±12.1* 1.4±2.2 0.8±3.4*** Neutrophils % 31.6±2.5 63.1±3.2 36.6±2 39.8±1.6 Eosinophils×106·mL−1 0.2±4.5 0.2±2.5 0.01±4.5 0.03±2.5 Eosinophils % 7.2±3.3 1.5±3.4 2.5±2*** 1.2±6.7 Macrophages % 40.5±1.8 18.2±3.7 44.7±1.5 45.7±2 Lymphocytes % 1.1±2.2 1.1±2.5 1.7±2 1±3 Epithelial cells % 2.7±2.7 3.3±5.5 1.4±1.3 2.2±6.1 Squamous cells % 4.9±2.7 4.6±3.1 5±3.3 4.4±1.2 IL-8 ng·mL−1 20.9±5.5 35±3.7 11.8±6.1 17.8±6.1 IL-5 positive cells % 15.6±1.8 8.4±1.6 2±0.4 1.4±1.8 ECP ng·mL−1 3072±55 3090±49 460±5*** 398±18 Neutrophil elastase µg·mL−1 169±3.3 3129±7.4* 100±2.5 120±9.6*** LDH IU·mL−1 182±2.2 550±16* 54±12.7*** 64±1.9*** Data are presented as mean±sd
TCC: total cell count
IL: interleukin
ECP: eosinophil cationic protein
LDH: lactate dehydrogenase
IU: international units. The analysis was carried out using unpaired t-tests on log-transformed data
*: p<0.05, significantly higher than subjects with noninfective acute asthma at Visit 1
#: p<0.05, significantly higher than subjects with infection and acute asthma at Visit 1
***: p<0.001, significantly lower than Visit 1
- Table 3—
Linear regression analysis to predict sputum lactate dehydrogenase (LDH)
Log LDH IU·mL−1 Coefficient Standard error P>t Log neutrophils×106·mL−1 0.42 0.1 p=0.001 Log eosinophils×106·mL−1 −0.18 0.09 p=0.06 Log ECP ng·mL−1 0.21 0.15 p=0.2 Log neutrophil elastase 0.02 0.08 p=0.5 Log IL-8 ng·mL−1 0.33 0.18 p=0.09 Constant 2.2 1.1 p=0.059 IU: international units
ECP: eosinophil cationic protein
IL: interleukin. Probability F>0.0001, adjusted R2=0.787
- Table 4—
Linear regression analysis to predict length of hospital stay in acute asthma
Length of stay days Coefficient Standard error P>t Log neutrophils×106·mL−1 0.44 0.37 p=0.3 Log eosinophils×106·mL−1 −0.31 0.25 p=0.3 Log LDH IU·mL−1 2.56 0.6 p=0.002 Log ECP ng·mL−1 1.19 0.4 p=0.02 Log neutrophil elastase 0.10 0.21 p=0.6 Age yrs 0.03 0.02 p=0.3 Sex −1.3 0.62 p=0.06 Smoking status 1.7 0.86 p=0.08 Prednisone use 0.85 0.73 p=0.3 Aas severity score 7 −0.82 0.34 p=0.04 Constant −1.97 3.15 p=0.549 LDH: lactate dehydrogenase
IU: international units
ECP: eosinophil cationic protein. Probability F=0.004, adjusted R2=0.797









