





Abstract
Exhaled nitric oxide (NO) concentration is a noninvasive measure of airway inflammation and is increased in asthma. Inhaled glucocorticoids decrease exhaled NO concentration, but the relative contributions of alveolar and bronchial levels to the decrease in exhaled NO concentration are unknown. Alveolar NO concentration and bronchial NO flux can be separately approximated by measuring exhaled NO at several exhalation flow rates. The effect of steroid treatment on alveolar and bronchial NO output in asthma was studied.
Alveolar NO concentration and bronchial NO flux were assessed in 16 patients with asthma before and during treatment with inhaled fluticasone for 8 weeks and in 16 healthy controls.
Before the treatment, asthmatics had increased bronchial NO flux (mean±sem: 3.6±0.4 versus 0.7±0.1 nL·s−1, p<0.001) but normal alveolar NO concentration (1.2±0.5 versus 1.0±0.2 parts per billion (ppb), p>0.05) compared with controls. Inhaled fluticasone decreased bronchial NO flux from 3.6±0.4 to 0.7±0.1 nL·s−1 (p<0.01) but had no effect on alveolar NO concentration (before: 1.2±0.5; after: 1.2±0.1 ppb, p>0.05). The forced expiratory volume in one second improved, whereas asthma symptom score and serum levels of eosinophil cationic protein and eosinophil protein X decreased during the treatment.
In conclusion, inhaled fluticasone decreases bronchial but not alveolar nitric oxide output simultaneously with clinical improvement in patients with asthma.
- asthma
- eosinophil cationic protein
- eosinophil protein X
- exhaled nitric oxide
- inflammation
- inhaled glucocorticoids
The present study was supported by grants from the National Technology Agency (Tekes), Tampere University Hospital Medical Research Fund, Tampere Tuberculosis Foundation and the Academy of Finland.
Nitric oxide (NO) is a gaseous signalling molecule participating in airway physiology. As pulmonary NO production increases in inflammation, the measurement of NO concentration in exhaled air provides a noninvasive method to detect airway inflammation 1, 2. Patients with an inflammatory airway disease like asthma have increased exhaled NO concentrations 3, 4. Exhaled NO levels in asthma correlate with the severity of airway inflammation 2. Treatment with inhaled glucocorticoids reduces increased exhaled NO concentration in asthma towards normal 5, 6. Further, bronchial inducible nitric oxide synthase (iNOS) expression 7 and bronchial NO output 8 have been shown to decrease during inhaled corticosteroid treatment. However, it is not known whether the decreased exhaled NO concentration during steroid treatment is explained solely by the decrease in bronchial NO output, or whether steroids also affect alveolar NO output.
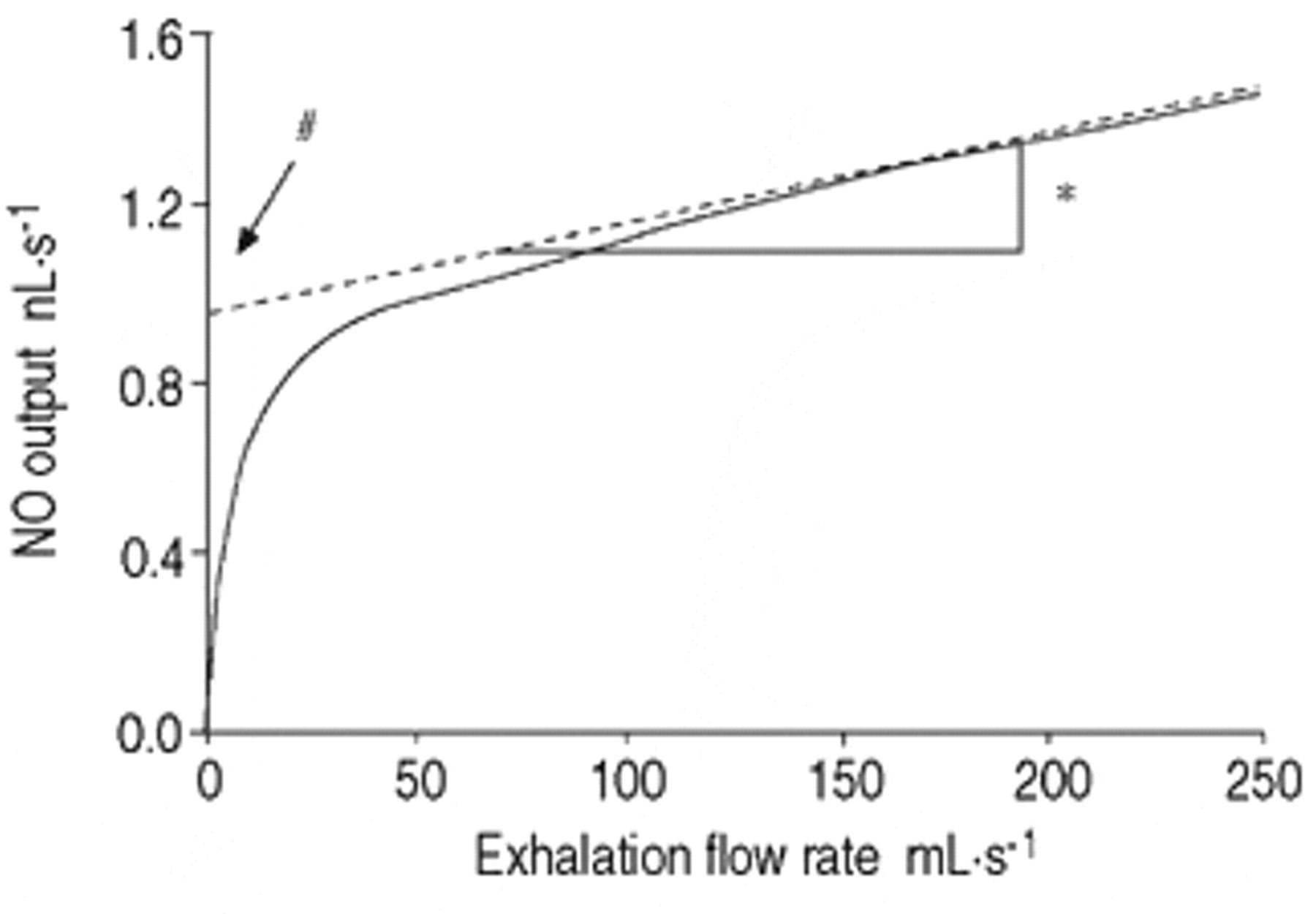
Recent mathematical models of pulmonary NO dynamics provide theoretical means to separately assess alveolar and bronchial NO output 8–11. In these models, the lung is divided into two separate compartments, namely alveolar and bronchial compartments. Air in the alveoli is supposed to have a certain concentration of NO (alveolar NO concentration). During exhalation, the alveolar air travels through the bronchial compartment, where NO diffuses between the bronchial wall and luminal air, and the exhaled air gains its final NO concentration. Because the amount of NO diffusing from the bronchial wall to exhaled air depends on the time that the exhaled air lingers in the bronchial compartment, exhaled NO concentration decreases, whereas NO output (exhaled NO concentration multiplied by exhalation flow rate) increases as a function of exhalation flow rate (fig. 1⇓). Alveolar NO concentration and bronchial NO flux (the quantity of NO diffusing from bronchial wall to luminal air in a unit time) can be calculated by measuring exhaled NO at several exhalation flow rates and then fitting a regression line on the linear part of the NO output curve against exhalation flow rate (flow rate >50 mL·s−1). The slope and the intercept of this regression line are approximates of alveolar NO concentration and bronchial NO flux, respectively 9 (fig. 1⇓). Thus, increased bronchial NO flux will cause a higher intercept, whereas increased alveolar NO concentration will cause a steeper slope of the regression line. It has previously been shown that this method can be used to differentiate between alveolar and bronchial inflammation, and that NO output in steroid-naive asthma is enhanced in the bronchial but not the alveolar compartment 12, 13.

Nitric oxide (NO) output (—) against exhalation flow rate and a regression line (-; -; -; -;) fitted to the linear part of the NO output curve. The slope (*) and the intercept (#) of the linear regression are approximates of alveolar NO concentration and bronchial NO flux, respectively 9.
In this study, the bronchial NO flux and alveolar NO concentration was assessed in 16 patients with newly diagnosed asthma before and during treatment with inhaled fluticasone for 8 weeks. The aim of the study was: 1) to assess the effect of inhaled fluticasone on alveolar and bronchial NO output in asthma; 2) to compare the time course of changes in bronchial and alveolar NO output, forced expiratory volume in one second (FEV1) and asthma symptom score during steroid treatment; and 3) to study whether the change in exhaled NO correlates with changes in serum markers of eosinophilic inflammation.
Subjects and methods
Subjects
Steroid-naive, nonsmoking patients (n=16, 5 males, mean age of 36 yrs, range: 20–57) with newly diagnosed asthma were recruited. Asthma diagnosis was based on symptoms and reversible or variable airway obstruction (β2-;agonist induced increase in peak expiratory flow (PEF), forced vital capacity (FVC) or FEV1 ≥15% or diurnal variability in PEF ≥20% or exercise induced decrease in FEV1 ≥15%). Exhaled NO was also measured in 16 age- (±5 yrs) and sex-matched nonsmoking healthy controls with no asthmatic symptoms and normal lung function. The study was approved by the ethical committee of Tampere University Hospital and all subjects gave written informed consent.
Study design
An 8-;week, open, follow-up study was conducted. All patients started treatment with inhaled fluticasone propionate (Flixotide Diskus 250 µg, GlaxoWellcome, Ware, UK) dosed 500 µg twice daily during weeks 1–4, and 250 µg twice daily during weeks 5–8. Alveolar NO concentration and bronchial NO flux were assessed, spirometry was measured and patients scored their asthma symptoms on nine occasions: before the treatment and on 8-;weekly visits during the follow-up. Serum levels of eosinophil cationic protein (ECP) and eosinophil protein X (EPX) were measured before and after 8 weeks of treatment.
Exhaled nitric oxide and airway function
Exhaled NO was measured with a Sievers NOA 280® NO analyser (Sievers Instruments, Boulder, CO, USA) at three exhalation flow rates, 100, 175 and 370 mL·s−1 with a mouth pressure of 9 cmH2O 12. The analyser was calibrated daily with a known NO concentration (103 parts per million (ppm), AGA, Sweden) and before every subject with filtered NO-free air. Alveolar NO concentration and bronchial NO flux were calculated for each subject using the method of Tsoukias and George 9. Airway function was measured with a Vmax 20 C spirometer (SensorMedics, Yorba Linda, CA, USA).
Asthma symptom score
Asthma symptoms were scored using a written questionnaire. Cough, wheeziness and chest tightness during the past week were each scored as 0=none, 1=symptoms at 1 day, 2=symptoms at ≥2 days, 3=symptoms every day. Nocturnal asthma symptoms during the past week were scored as 0=no nocturnal symptoms, 1=symptoms on 1 night, 2=symptoms on ≥2 nights, 3=symptoms every night. Thus, the maximum symptom score was 12.
Serum markers
Venous blood was collected into 4 mL Vacutainer hemogaard SST tubes (Becton Dickinson, Franklin Lakes, NJ, USA) for serum ECP and EPX measurements. The samples were allowed to clot for 60 min at 22°C and then centrifuged at 1,300×g for 10 min to separate the serum. Radioimmunoassay (ECP RIA and EPX RIA, Pharmacia AB, Uppsala, Sweden) was used to measure ECP and EPX levels.
Analysis
Differences in NO levels between patients with asthma and healthy controls were analysed with an unpaired t-;test. Changes in NO parameters, lung function and symptom score during the treatment were analysed using repeated measures analysis of variance with Dunnett's post-test. Changes in serum markers were analysed with a paired t-;test. Pearson's r was used to study the correlation between changes in different parameters. Results are expressed as mean±sem.
Results
Bronchial and alveolar nitric oxide
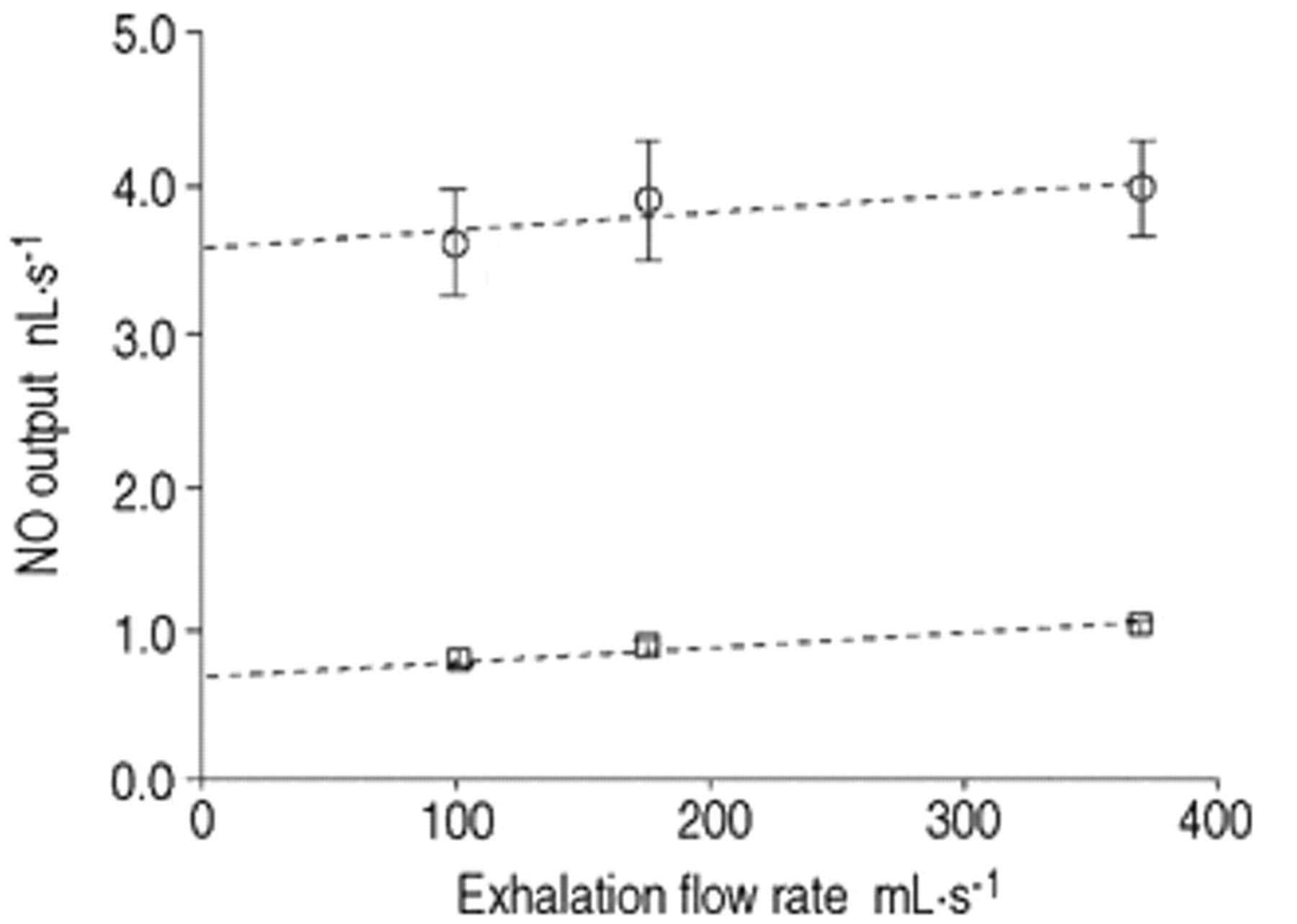
Before treatment, bronchial NO flux was increased in patients with asthma compared with healthy controls (3.6±0.4 versus 0.7±0.1 nL·s−1, p<0.001), while alveolar NO concentration was normal (1.2±0.5 versus 1.0±0.2 parts per billion (ppb), p>0.05) (fig. 2⇓). Treatment with inhaled fluticasone for 8 weeks decreased bronchial NO flux in asthmatics from 3.6±0.4 to 0.7±0.1 nL·s−1 (p<0.01) and the decrease was significant after 1 week. After treatment, bronchial NO flux in asthmatics was equal to that of healthy controls (p>0.05). The treatment had no effect on alveolar NO concentration (before: 1.2±0.5 ppb, after: 1.2±0.1 ppb, p>0.05) (fig. 3⇓) (table 1⇓).

Nitric oxide (NO) output (mean±sem) against exhalation flow rate and linear regression in 16 patients with asthma before steroid treatment (○) and in 16 healthy controls (□).

{kind=link}
{kind=link}
{kind=link}
a) Bronchial nitric oxide (NO) flux, b) alveolar NO concentration, c) forced expiratory volume in one second per cent of predicted (FEV1 % pred), d) asthma symptom score, before and during 8 weeks of treatment with inhaled fluticasone in 16 patients with newly diagnosed asthma. ppb: parts per billion. **: p<0.01, compared with baseline value before the treatment.
Subject characteristics
Forced expiratory volume in one second, asthma symptom score and serum markers
Fluticasone treatment improved FEV1 % predicted from 85%±3% to 93%±4% (p<0.01) and the improvement was significant after 2 weeks (fig. 3⇑). There was a trend towards a correlation between the change in bronchial NO flux and the change in FEV1, but this was not significant (r=−0.42, p=0.11).
The asthma symptom score decreased from 6.2±0.9 to 0.3±0.2 (p<0.01) during the treatment. The time course of symptom score was similar to that of bronchial NO flux. Halving the fluticasone dose after 4 weeks caused no shift in bronchial NO flux, FEV1 or symptom score (fig. 3⇑).
Fluticasone treatment decreased serum levels of ECP from 25±5 to 16±2 µg·L−1 (p<0.05) and EPX from 53±7 to 35±4 µg·L−1 (p<0.01). There was a positive correlation between changes in serum levels of ECP and EPX (r=0.93, p<0.001). There was a trend towards a correlation between the change in bronchial NO flux and the change in serum EPX but this was not significant (r=0.42, p=0.11).
Discussion
An increased bronchial NO flux but normal alveolar NO concentration in patients with newly diagnosed asthma was found. Inhaled fluticasone decreased bronchial NO flux but had no effect on alveolar NO concentration. Bronchial NO flux decreased simultaneously with the improvement in lung function and decrease in asthma symptom score and serum markers of eosinophilic inflammation.
The new method of measuring exhaled NO at several exhalation flow rates used in this study, allows differentiation between alveolar and bronchial NO output. The results showing increased bronchial NO flux but normal alveolar NO concentration in steroid-naive asthma are consistent with earlier studies 12, 13. Bronchial epithelial cells express iNOS in response to inflammatory cytokines 14. Increased exhaled NO concentrations at a single exhalation flow rate in asthma correlate with enhanced iNOS expression in the airways 7. Thus, the enhanced iNOS expression in asthmatic airways probably explains the increased bronchial NO flux before steroid treatment in patients in the present study.
There are earlier studies showing that inhaled glucocorticoids in asthma decrease exhaled NO measured with the single exhalation flow rate technique 5, 6, 15. However, with that technique, the anatomical site where steroids reduce NO production cannot be identified. Silkoff et al. 8 reported that treatment of asthma with inhaled beclomethasone decreased NO production at the bronchial level, but they did not study whether steroids affect alveolar NO concentration. The present study extends the previous data by showing that inhaled fluticasone decreased bronchial NO flux but had no effect on alveolar NO concentration. As only bronchial NO flux was increased in steroid-naive asthmatics and inhaled glucocorticoids decreased bronchial NO flux but had no effect on alveolar NO concentration, the inflammatory component responsible for increased NO synthesis in these patients probably mainly affects the conducting airways.
Earlier reports show either weak 16 or no correlation 17 between airway function and concentrations of exhaled NO measured with the single-exhalation flow-rate technique. In this study, a tendency but not a significant correlation between changes in bronchial NO flux and FEV1 during the treatment period was found. These results suggest that exhaled NO is not a marker of airflow limitation in asthma. However, in the group of patients with newly diagnosed asthma, the change in FEV1 and asthma symptoms took place simultaneously with the decrease in bronchial NO flux.
Bronchial NO flux and serum levels of ECP and EPX all decreased during the treatment. The decrease in bronchial NO flux tended to, but did not significantly correlate with changes in serum EPX. It is possible that exhaled NO and these serum markers of eosinophilic inflammation reflect different aspects of asthmatic inflammation. Exhaled NO reflects inflammatory iNOS expression in epithelial and inflammatory cells of airways 7, whereas serum ECP and EPX reflect general eosinophil activation in the body. Thus, exhaled NO is probably a more sensitive marker than serum proteins to detect the anti-inflammatory effects of inhaled glucocorticoids. It has been shown that levels of exhaled NO correlate with numbers of eosinophils in sputum 18, and a better correlation might have been found between changes in bronchial NO flux and measures of local eosinophil activation in the lungs.
Inhaled glucocorticoids have been shown to reduce iNOS expression in asthmatic airways 7. Steroids may reduce iNOS expression indirectly by suppressing asthmatic airway inflammation and thus, downregulating the synthesis of pro-inflammatory cytokines known to induce iNOS expression. Glucocorticoids can also reduce iNOS expression directly by inhibiting nuclear factor-;κB, a critical factor for transcription of iNOS 19, 20. However, the detailed mechanism of how inhaled glucocorticoids reduce NO production in the airways, and whether the decrease in bronchial NO flux contributes to the anti-inflammatory action of inhaled glucocorticoids still needs to be determined.
In conclusion, inhaled fluticasone in patients with newly diagnosed asthma had no effect on alveolar nitric oxide concentration but decreased bronchial nitric oxide flux simultaneously with clinical improvement and a decrease in serum markers of eosinophilic inflammation.
Acknowledgments
The authors would like to thank P. Pirttimäki and M-;L. Lampén for their skillful assistance with measurements of exhaled nitric oxide and serum markers.
- Received January 18, 2001.
- Accepted June 12, 2001.
- © ERS Journals Ltd
References









