





Abstract
In cystic fibrosis (CF), low concentrations of exhaled nitric oxide (NO) and reduced expression of inducible nitric oxide synthase (iNOS) in airway epithelium have been reported. However, abundant iNOS expression has been found in the subepithelial tissues and elevated concentrations of NO metabolites in breath condensate and sputum. These conflicting results may be explained by increased scavenging of NO by superoxide radicals, resulting in rapid conversion to peroxynitrite, so that only a small proportion of the NO produced in the lung tissue reaches the airway lumen. If iNOS were active in the CF lung, exhaled NO would be further reduced by glucocorticoid treatment.
CF patients (n=13) were recruited to a double-blind, placebo-controlled study with crossover. Treatment comprised prednisolone or placebo for 5 days with a 9 day washout. After each treatment, exhaled NO was measured, spirometry performed and blood collected for measurement of serum nitrogen dioxide/nitrous oxide (NO2/NO3).
Ten patients (8 male) completed the study. Following prednisolone treatment (mean±sd) exhaled NO concentration (3.1±1.6 parts per billion (ppb)) was significantly reduced versus placebo treatment (4.9±4.2 ppb; p<0.05, Wilcoxon signed-rank test). Spirometric indices and serum NO2/NO3 concentration were unchanged.
These findings support the hypothesis that glucocorticoids suppress nitric oxide production in cystic fibrosis airways by reducing inducible nitric oxide synthase expression or by inhibiting recruitment of neutrophils, cells which express inducible nitric oxide synthase.
Supported by The Cystic Fibrosis Association (Ireland) and The Health Research Board (Ireland).
Low concentrations of nitric oxide (NO) in expired airway gases of cystic fibrosis (CF) patients 1–3 and reduced expression of inducible nitric oxide synthase (iNOS) in CF airway epithelium has been reported 4, 5. However, abundant iNOS expression has been found in the subepithelial tissues of CF lungs 5 and an elevated concentration of NO metabolites has been reported in breath condensate 6 and in sputum 2, 7. A potential explanation of these conflicting results is that there is increased scavenging of NO by superoxide radicals in the inflamed CF lung 8 resulting in the rapid conversion of NO to peroxynitrite, so that only a small proportion of the NO produced in lung tissue reaches the airway lumen. Peroxynitrite is a highly reactive molecule, which has been shown to cause tissue damage by a number of mechanisms 9. iNOS expression is reduced by glucocorticoids but expression of endothelial and neuronal NOS is not 10. Short courses of both oral and inhaled glucocorticoids have been shown to reduce both iNOS expression and exhaled NO 11–14. Therefore, if iNOS contributes to NO production in CF lungs, glucocorticoid treatment would be expected to reduce exhaled NO. The purpose of this study was therefore to measure the effect of oral glucocorticoid treatment on exhaled NO in patients with CF.
Methods
Patients
Thirteen patients with documented CF on the basis of clinical history and abnormal sweat electrolyte measurements (chloride >60 mmol·L−1) were recruited from the National Adult Cystic Fibrosis Unit, St. Vincent's University Hospital (Dublin, Ireland, UK). The study protocol was approved by the Ethics Committee of St. Vincent's University Hospital and all patients gave written informed consent. All patients were free of acute pulmonary exacerbation of CF for at least 2 months. Patients were excluded if they had a history of glucose intolerance, diabetes mellitus, major recent haemoptysis or pneumothorax. All patients had positive sputum cultures for Pseudomonas aeruginosa. No patients were taking oral glucocorticoids, nonsteroidal anti-inflammatory medication or any vasoactive medication at the time of recruitment. Three patients were on inhaled glucocorticoids (Becotide Inhaler® 500 µg, twice a day (two patients) and Flixotide Inhaler® 500 µg, twice a day (one patient)) for at least 1 yr prior to the study.
Study design
Patients withheld inhaled glucocorticoids during a 2-week run-in phase and throughout the study. Treatment was assigned in a double-blinded manner with patients receiving either prednisolone (0.5 mg·kg−1 rounded up to the nearest 5 mg) or matched placebo, each morning for 5 days. On the fifth treatment day they were reviewed, spirometry performed, Schwachman scores calculated, exhaled NO concentration measured and blood collected for full and differential cell counts and the measurement of serum nitrite/nitrate oxide (NO2/NO3) and C-reactive protein (CRP). A 9-day washout phase then preceded the second 5-day period of treatment with prednisolone or placebo after which the patients were again reviewed.
Measurements
Exhaled NO concentration was measured using a chemiluminescent analyser (LR 2000, Logan Research Ltd, Rochester, UK) and conformed to American Thoracic Society guidelines 15. The analyser was calibrated regularly using standard calibration gases (BOC gases Ltd, Dublin, Ireland) and ambient NO concentration was always <4 parts per billion (ppb). Patients exhaled against a fixed resistance while maintaining mouth pressure at 8–10 cmH2O guided by a visual display of mouth pressure giving a flow rate ∼0.43 L·s−1. Lower airway NO concentration was determined at the end of exhalation, as indicated by the plateau phase of the simultaneously measured carbon dioxide (CO2) concentration. This protocol ensured all measurements were made at constant expiratory flow rate and thus any changes directly reflected changes in airway NO excretion. The standard deviation (sd) of repeated measurements was 1.2 ppb. The mean of three measurements was recorded for each subject on each occasion. Spirometry was performed using a Vmax229 (Sensor Medics, Yorba Linda, CA, USA). Serum NO2/NO3 concentration was measured using the Griess reaction as previously described 16.
Statistical analysis
All data are expressed as mean±sd. Wilcoxon signed-rank test was used to assess differences between glucocorticoid and placebo treatments.
Results
Thirteen patients (eight male) were recruited to the study, three of these patients did not complete the study because of intercurrent illness and were excluded from analysis. Percentage predicted forced expiratory volume in one second (FEV1% pred) for these three were within the range of the other 10. Anthropometric data (mean±sd) for the 10 (eight male) patients who completed the study protocol were as follows: age 21.1±2.0 yrs, height 1.75±0.09 m, weight 65.5±12.6 kg, body mass index 21.2±2.5 kg·m−2, Schwachman score 84.9±4.2, forced vital capacity (FVC) 85±19% pred and FEV1 70±24% pred.
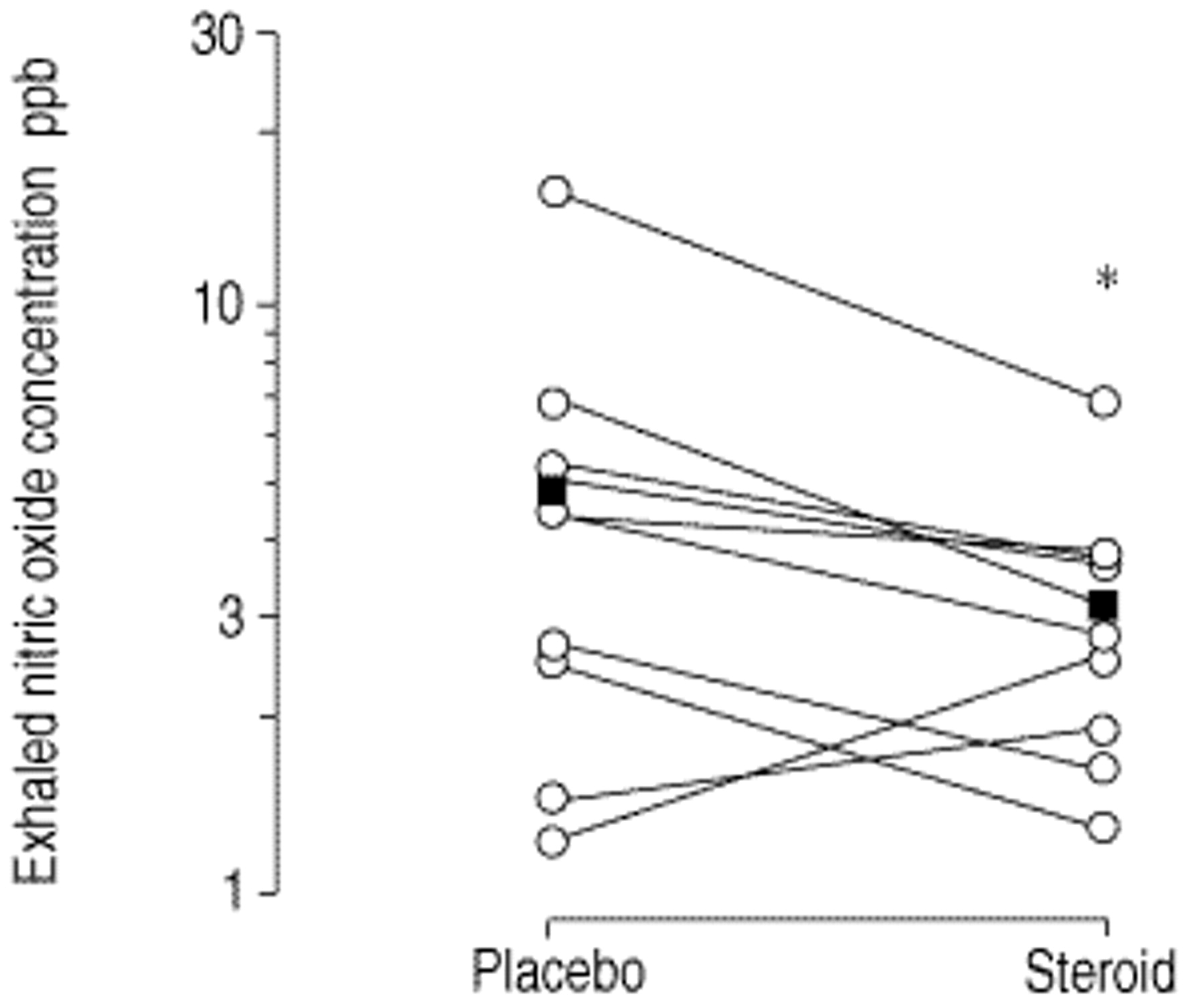
Mean exhaled NO decreased significantly following glucocorticoid treatment (fig. 1⇓), with eight of the 10 patients showing a reduction in exhaled NO. The two patients in which exhaled NO rose had the lowest concentrations while on placebo. Spirometric indices were not altered following prednisolone treatment (table 1⇓). Peripheral blood differential white cell counts showed an increase in mean concentration of neutrophils and a decrease in eosinophils after glucocorticoid treatment (table 1⇓). There was no change in the mean serum NO2/NO3 or CRP after each treatment period. The responses in the three patients on inhaled glucocorticoids prior to study entry were similar to those of the remainder of the patient group.

{kind=link}
Effect of oral glucocorticoid treatment on exhaled nitric oxide concentration in cystic fibrosis patients. The values for each patient during placebo and glucocorticoid treatments are joined by a straight line. ▪: mean value during placebo=4.9; ▪: mean value during steroid treatment =3.1. *: p<0.05 versus placebo treatment.
Spirometric indices and blood parameters for placebo and glucocorticoid treatments
Discussion
The low exhaled NO concentrations observed in the present study during placebo ingestion are in agreement with previous reports in CF patients 1–3. Glucocorticoid treatment reduced the exhaled NO further in these stable patients (fig. 1⇑). The reduction in concentration was in excess of 30% of basal values. Since all measurements were carried out at constant flow, this represents an exactly equal reduction in the total amount of NO exhaled. NO is a highly reactive gas that is rapidly oxidized by reaction with oxygen and superoxide radical at or close to its site of production 17. Therefore, only a small proportion of the total NO that is produced will reach the airway lumen, in particular in the presence of airway inflammation. Thus, the measured reduction in exhaled NO underestimates the total reduction in NO production in the cells of the airway epithelium.
Glucocorticoid treatment produced the expected effects on peripheral blood cell counts 18, increasing total cell and peripheral neutrophil counts and reducing the eosinophil count (table 1⇑), confirming that the patients complied with the study protocol.
Glucocorticoids have been shown to reduce the expression of iNOS but not the constitutive NOS (cNOS) isoforms in vitro 10. In asthmatic subjects, exhaled NO is increased due to the activity of iNOS and glucocorticoid treatment reduces both iNOS expression and exhaled NO 13, 14. The observation that a similar dose of oral glucocorticoid reduced exhaled NO in CF subjects, suggests that iNOS activity contributes to the exhaled NO in CF patients. Although iNOS expression in CF airway epithelium is reduced, its expression in the subepithelial tissues is increased 5. Glucocorticoid suppression of this subepithelial iNOS could account for the decreased NO excretion observed in the present study.
CF is characterized by a massive neutrophil influx into the lung tissue and since these cells express iNOS, they are a potential source of the exhaled NO. There is evidence that glucocorticoids may reduce neutrophil migration into the airways, a further mechanism that could reduce the amount of iNOS present in the CF airways. However, at the dose of oral glucocorticoid used in the present study, this effect is unlikely to be significant 19. Nonetheless, it is a mechanism that may have contributed to the decrease in exhaled NO.
Given the ability for strains of Pseudomonas to respire anaerobically by means of denitrification 20, it has been suggested that changes in NO2/NO3 in CF patients infected with P. aeruginosa should not be interpreted without reference to changes in bacterial load 7. Since NO is a reaction intermediate in this process, and all patients in the study had positive P. aeruginosa sputum cultures, bacterial denitrification is another potential source of NO in CF airways. However, a reduction in the number of bacteria would be required to account for the observed fall in exhaled NO. Given the well-known immunosuppresive effects of glucocorticoids, this seems unlikely.
In conclusion, following a short course of oral glucocorticoid treatment, exhaled nitric oxide was reduced when compared to placebo administration in adults with stable cystic fibrosis. The most plausible explanation for this finding is that a proportion of nitric oxide detectable in the breath of stable cystic fibrosis patients, is due to the presence of the glucocorticoid-suppressible isoform of nitric oxide synthase in the patients' airways.
Acknowledgments
The authors gratefully acknowledge the support of the staff of the Pathology Dept, St Vincent's University Hospital, Dublin, Hoechst Marion Roussel Ltd for the gift of prednisolone tablets and matched placebo, and M. Henry for assistance during exercise testing.
- Received July 20, 2000.
- Accepted January 19, 2001.
- © ERS Journals Ltd
References









