





Abstract
The reproducibility and acceptability of airways resistance measurements using the interrupter technique (MicroRint) obtained using a mouthpiece were compared with those using a face mask.
Fifty children aged 4–7 yrs performed four sets of six Rint measurements; two using a mouthpiece and two using a face mask with integral mouthpiece.
Complete data were obtained from 45 (90%) children using the mouthpiece and 43 (86%) children using the mask. The two methods were equally repeatable with comparable intraclass correlation coefficients (ICC) and coefficients of variation. Mean Rint values obtained using the mouthpiece were significantly lower than those using the face mask ((mean±sd) mouthpiece=0.81±0.18 kPa·L−1·s, mask=0.88±0.24 kPa·L−1·s p=0.0002). Although the mean paired differences between the two methods were small (0.07 kPa·L−1·s), the ICC and limits of agreement confirmed that the two methods could not be used interchangeably. Sixty-seven per cent of children preferred the face mask but this was more time-consuming (p=0.03). Children did not produce more repeatable results using their preferred method, nor did they improve with practice.
Repeatable airway resistance measurements using the interrupter technique can be obtained from young children using either a mouthpiece or a face mask, but there are significant clinical and statistical differences between the results obtained.
- airway resistance
- child
- interrupter technique
- masks
- reproducibility of results
- respiratory function tests
This study was supported by a grant from AstraZeneca Pharmaceuticals.
Lung function testing plays an important role in the assessment of a child with respiratory disease. In school-aged children it is used to aid diagnosis and guide treatment. It can detect abnormalities and assess their severity. It also allows a child's progress and response to treatment to be monitored objectively.
In younger children, where making a diagnosis may be more difficult, objective information about lung function would also be useful. Unfortunately, few children <7 yrs can perform spirometry reliably and although some can produce repeatable peak expiratory flow (PEF) readings 1, these are effort-dependent and may be inaccurate at the low flow rates produced by young children 2, 3. They may also fail to identify clinically significant falls in forced expiratory volume 4. Until recently, however, alternative objective methods were not widely available.
Several techniques have now been developed specifically for use in preschool children 5–10. Most of these require complex equipment and are mainly used as research tools. However, the interrupter technique enables the measurement of airways resistance (Rint) easily and repeatably in young children 11, 12. When used in conjunction with a bronchodilator, it can help separate children with reversible airways disease from those with other disorders 12. This allows antiasthma therapy to be used more selectively in young children and should help to ensure that those with severe airways obstruction are identified and monitored appropriately.
The interrupter technique is based on the assumption that, during transient occlusion of the airway at the mouth, alveolar pressure will equilibrate rapidly with mouth pressure. Airways resistance can then be calculated from the ratio of the mouth pressure (measured immediately after occlusion) to the airflow at the mouth (measured just prior to occlusion) 13. As equilibration of mouth and alveolar pressure may occur more slowly in obstructed airways, Rint tends to underestimate airways resistance in children with asthma 6, 14. However, in children aged 5–15 yrs it has been shown to be as sensitive as spirometry in detecting bronchodilator responsiveness 15. Rint can now be measured using portable, affordable equipment 8, 10, 12, 15–18, hereby providing the potential to assess lung function more easily in children <7 yrs. In the past this was only possible using expensive and complex plethysmographic methods 5, 6, 14, 19, 20.
Rint measurements are obtained during tidal breathing, are noninvasive, effort- independent and require minimal subject cooperation. However, they are critically dependent on the position of the head and the compliance of the upper airway 8, 14. Measurements may be obtained using a face mask 5, 6, 18, 19 or a mouthpiece and noseclip 8, 11, 12, 15–17. Both methods show good intrasubject 5, 6, 8, 11, 12, 15–19and interobserver reliability 12, 21, but it is not clear whether one is superior to the other. Some authors have reported difficulties in obtaining repeatable results in up to 30% of children using the mouthpiece 11, 12. This may be due to problems in forming a tight seal or difficulties with the noseclip. Such measurements might be more successful using a face mask. There are no published comparisons of face mask and mouthpiece measurements and it is not known whether the results are method-dependent. As reference ranges are currently being developed 5, 11, a standardized method for measuring Rint needs to be agreed.
The aim of this study in 4–7-yr-old children, was to compare the reproducibility, ease and acceptability of Rint measurements using a mouthpiece and noseclip with measurements using a face mask (fig. 1⇓).

Face mask with integral mouthpiece, noseclip and mouthpiece.
Materials and methods
Subjects
Fifty children (23 male, mean age 5.8 yrs, range 4.2–7.8 yrs) were recruited from local primary schools, the outpatient dept at the City General Hospital, Stoke-on-Trent, UK, and from an ongoing asthma study. All children aged 4–7 yrs seen during the study period were approached. Both asthmatic and nonasthmatic children were included. Children with respiratory diseases other than asthma were excluded, as were children with current wheeze. The local research ethics committee approved the study and parents gave informed written consent for their children to take part.
Measurements
Expiratory Rint measurements were obtained by a single observer using the Micro Rint machine (MicroMedical Ltd, Rochester, Kent, UK). Flow and pressure calibrations were performed as recommended by the manufacturer. Each measurement consisted of six acceptable Rint readings 12. To see if children produced more repeatable results with practice, four measurements, two with a mask (M1 and M2) and two with a mouthpiece (MP1 and MP2), were obtained from each child. The child alternated between methods, 50% starting with the mouthpiece and 50% with the face mask.
All measurements were obtained during quiet tidal breathing with the child seated with their head slightly extended. No formal measurements of respiratory rate, flow or tidal volume were made, but the child's breathing pattern was observed closely by the study team. Rint readings were rejected if the child coughed or breathed irregularly, or if the pressure/time curve failed to fulfil accepted criteria 8, 18. The child was familiarized with the sensation of valve closure prior to data collection. Airway occlusion occurred within 10 ms of peak tidal flow and lasted 100 ms.
Mouthpiece measurements were obtained with the child breathing through a 2.7 cm diameter cardboard mouthpiece (dead space 40 mL). The child wore a noseclip, the cheeks being supported from behind by a single observer. Where children refused the noseclip, their noses were occluded manually by the same observer. Face mask measurements were obtained using a single noncompressible face mask (AstraTech, Gloucester, UK) with integral mouthpiece, as described by Klug and Bisgaard 19 (fig. 1⇑). The mask was firmly applied to the face, ensuring there were no leaks and that the mouthpiece was inside the mouth. The mask had a total dead space of 133 mL and the integral mouthpiece had a dead space of 29 mL.
After the final measurement, the children were asked whether they preferred using the mouthpiece or the face mask. To assess ease of administration, the time taken to obtain each of the four measurements was recorded.
Statistical analysis
To identify a minimum difference of 15% between the two methods with 95% power and a two-sided significance level of 1%, a sample size of 36 was required. A difference of 15% was chosen because the published within-subject coefficient of variation for Rint measurements in children is 7–14% 5, 6, 8, 12, 15–18. The final sample of 50 children allowed for a failure rate of up to 28% 11, 12. For each set of six readings, the within-subject repeatability was assessed using the within-subject coefficient of variation (CoV). The intraclass correlation coefficient (ICC) 22, 23 was used to assess the agreement between mean values obtained by the same method on the two occasions (M1 and M2, MP1 and MP2) and by different methods on the same occasion (M1 and MP1, M2 and MP2). The ICC is a measure of the agreement between repeated measurements using the same instrument in a number of individuals. Here it was calculated from a one way analysis of variance table and was used in preference to the better known kappa statistic, because it measures agreement between continuous rather than categorical data. The agreement between methods was further assessed using the limits of agreement 24, the mean paired differences and their sds.
Results
Twelve children (6 male) with a history of wheeze (wheezers) and 38 children (17 male) with no history of wheeze (nonwheezers) were studied. One child was coryzal but not currently wheezy and had no history of wheeze. The mean±sd age and height of the wheezers (6.1±0.7 yrs, 116.2±8.2 cm) and nonwheezers (5.7±0.9 yrs, 115.9±8.1 cm) were not significantly different.
Success rate
Complete data were obtained from 45 (90%) children using the mouthpiece and 43 (86%) children using the mask. Two (4%) children provided only a single set of measurements using the mask. Five (10%) children were unable to produce reliable results using either method. Two of these found the clicking noise frightening (aged 4.3 and 5.3 yrs). Three found it difficult to establish regular tidal breathing (aged 4.8, 5.2 and 5.6 yrs). Only the 43 children who completed all four sets of measurements were included in the analysis (32 nonwheezers, 11 wheezers).
Mean measurements
As expected, mean Rint measurements were height- (p<0.001) and age- (p≤0.002) dependent with smaller, younger children having significantly higher values. This was true for both mask and mouthpiece readings. There was no significant difference between mean Rint measurements obtained from children with and without a history of wheeze.
Repeatability of measurements
Both methods were equally repeatable. Readings taken on the first occasion showed a mean±sd intrasubject CoV of 10.6±4.7% for the mouthpiece and 11.4±8.3% for the mask. Mean Rint measurements obtained on the two occasions by the same method were not significantly different (table 1⇓). The ICC (1 sided lower 95% confidence limit) for the mouthpiece measurements (mean MP1) was 0.76±0.69 and for the mask measurements (mean M1) was 0.77±0.70. The paired differences (mean±sd) between mean Rint values on the two occasions were −0.02±0.11 kPa·L−1·s for the mouthpiece and −0.01±0.17 kPa·L−1·s for the mask. There was no significant correlation between CoV and age with either method on the first occasion. On the second occasion there was a moderate negative correlation between CoV and age using the mouthpiece (r=−0.45, p=0.002) but not using the mask.
Comparison of airway resistance measurements using the interrupter technique (Rint) with mouthpiece and face-mask; mean value, repeatability and time taken.
Comparison between measurements using the mask and the mouthpiece
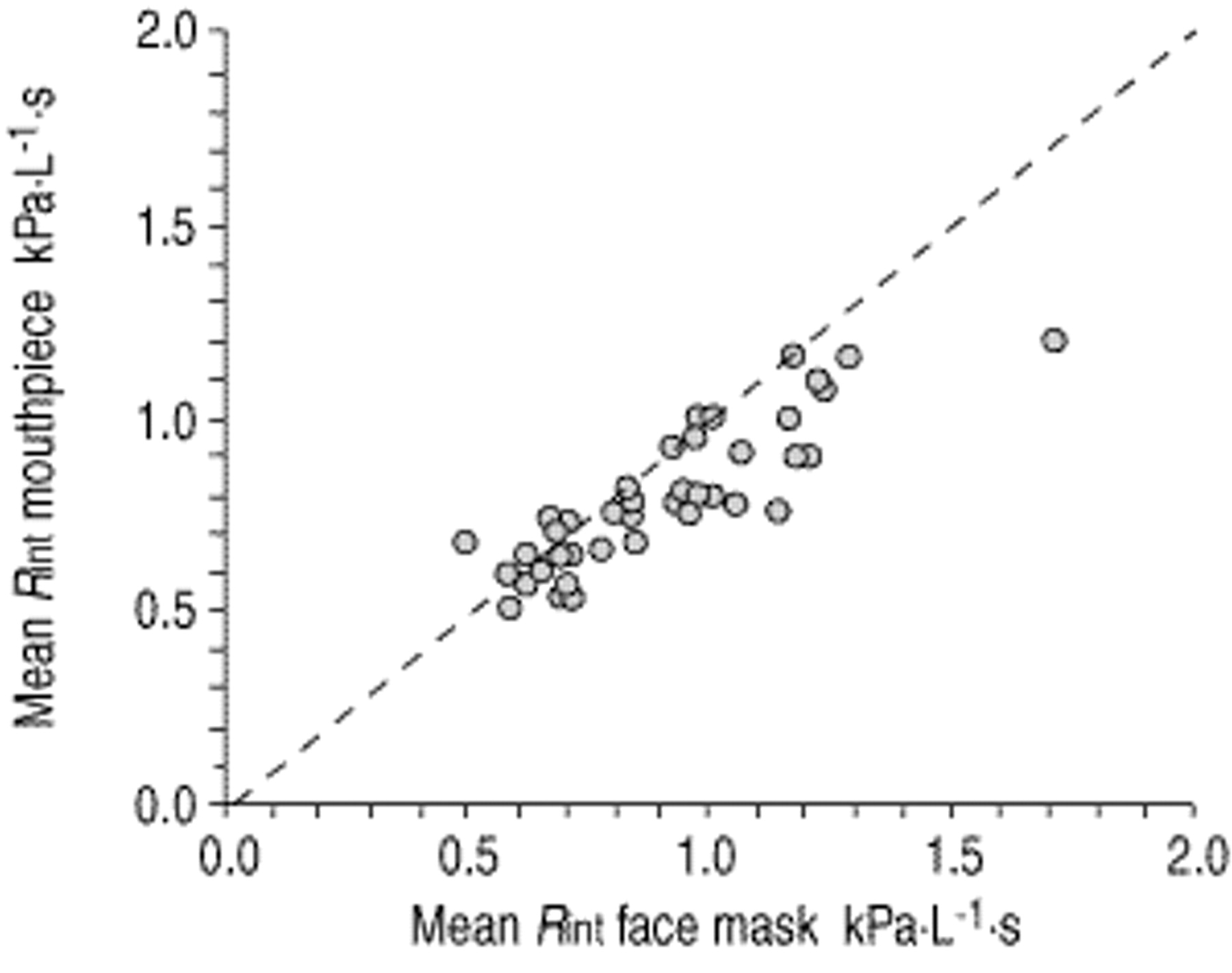
Results obtained using the two methods were significantly different, with the mask giving higher mean results on both occasions (table 1⇑, fig. 2⇓). The paired differences (mean±sd) between mean Rint values obtained using the two methods were 0.07±0.12 kPa·L−1·s on the first occasion and 0.06±0.12 kPa·L−1·s on the second occasion. The paired differences between methods increased significantly with increasing values of Rint by face mask (r=0.69, p<0.001; fig. 2⇓). This was not due to age, as the paired difference and age were not significantly correlated. Comparison between mean measurements obtained on the first occasion by the two methods revealed an ICC (1 sided lower 95% confidence limit) of 0.75±0.43. Limits of agreement, calculated using the equation d±2s (where d=mean difference between the mask and mouthpiece measurements (first occasion) and s=the standard deviation of the differences) 24, were wide (−0.17–0.31 kPa·L−1·s) (fig. 3⇓). Mouthpiece measurements were obtained more quickly than mask measurements (table 1⇑). Children did not produce faster or more repeatable results on the second occasion with either method.

Comparison between mean airways resistance measurements using the interrupter technique (Rint) obtained using the two methods. The dashed line represents the line of equality.

Bland and Altman plot of the difference between mask and mouthpiece readings. Rint: airways resistance measured using the interrupter technique. Dashed lines indicate mean±2sd of the difference between the methods.
Preference
Thirty-one (62%) children preferred using the mask, 15 (30%) preferred the mouthpiece, two (4%) liked both methods equally and two (4%) did not state a preference as they only tried one method before withdrawing. The child's preference did not have a significant effect on the CoV of the method used on either occasion. Of the two children who failed to complete two sets of mask measurements, yet were successful with the mouthpiece, one preferred using the mask, the other the mouthpiece.
Discussion
This study confirms that reproducible Rint measurements can be obtained quickly and easily from children aged 4–7 yrs using either a face mask or a mouthpiece.
Rint correlates well with other measurements of lung function in normal children 8, 11, 19, in children with asthma 6, 8, 15, 17 and in children with cystic fibrosis 8. The correlation between Rint and specific airways resistance measured using a plethysmograph is also good 5, but Rint measurements are potentially affected by the resistance of the lungs and chest wall as much as that of the airways themselves 25.
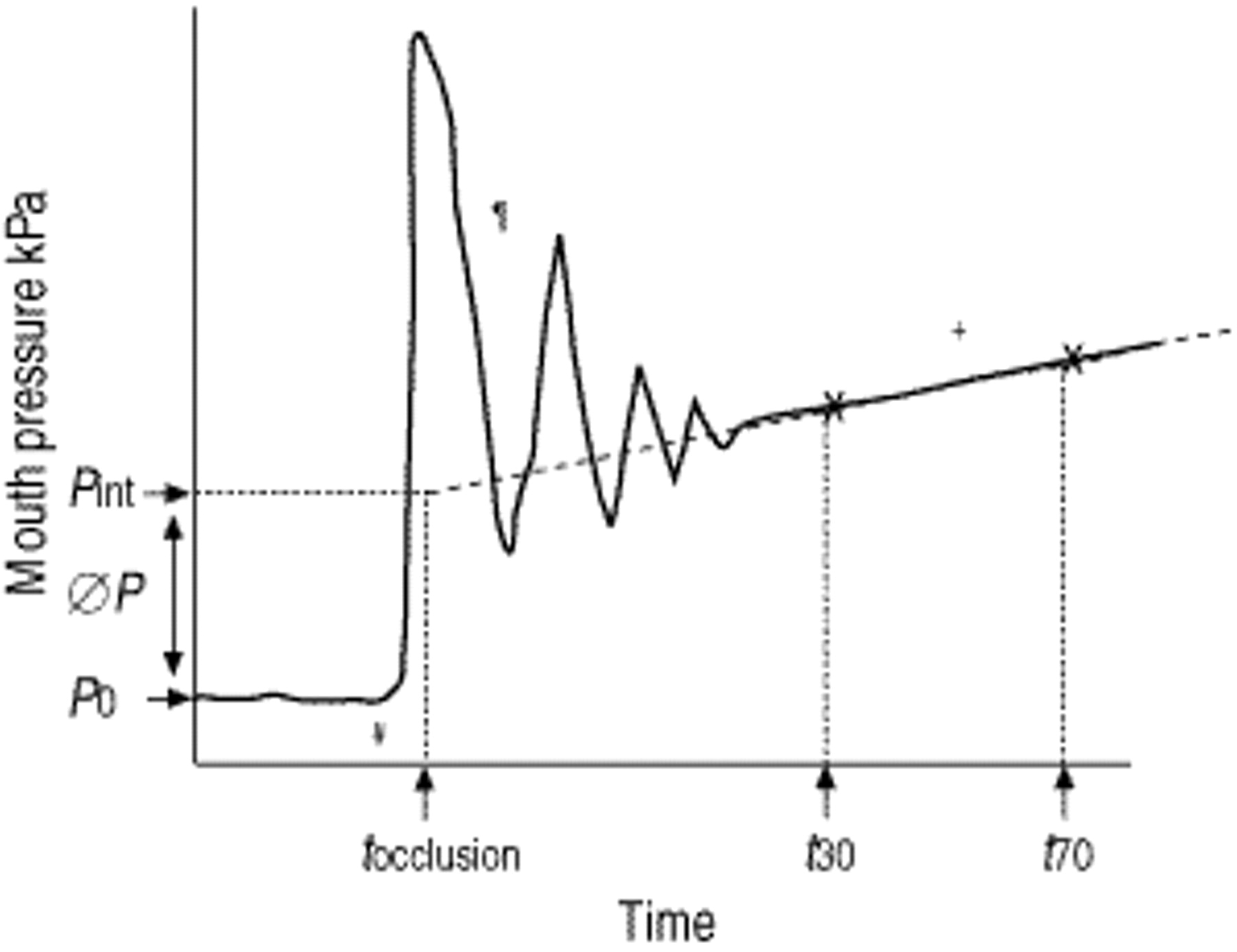
Following airway occlusion, a mouth pressure/time (Pm(t)) curve is produced (fig. 4⇓). The relative contributions from the airways, lungs and chest wall to the final measurement depend very much on how this curve is analysed 25. Animal experiments suggest that measurements taken from an early point on the curve provide the best approximation of the true airways resistance but are less repeatable that those taken later 25. In this study expiratory linear back extrapolation Rint (Rint,L) (fig. 4⇓) measurements were used because they have been shown to exhibit the least baseline variability and the greatest sensitivity for detecting induced airway obstruction 7.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Optimal mouth pressure/time (Pm(t)) curve showing back extrapolation airways resistance of the lungs using the interrupter technique (Rint,L). An optimal Pm(t) curve should display a sharp increase in pressure immediately following occlusion (#), a series of high frequency oscillations (¶) and a smooth increase in pressure (+) 8, 12, 18. Rint,L measurements are obtained by linear back extrapolation of two points from the curve, 30 and 70 ms post-occlusion (t30 and t70) to an arbitrary point, 15 ms post- occlusion, at which total valve closure is thought to have occurred (tocclusion). Mouth pressure measurements are taken pre-occlusion (P0) and at tocclusion (Pint). ΔPint is calculated from the difference between these two measurements (ΔP). The ratio of this measurement to the expiratory flow at the mouth at the time of occlusion gives the Rint measurement 18.
Measurements using the mouthpiece and the face mask were equally successful and reproducible. The higher success rate in wheezers (11/12) than nonwheezers (32/38) may have been because wheezy children were familiar with a face mask from past inhalation therapy. Surprisingly, although most children preferred using the face mask, it took longer and measurements were more difficult to obtain. Children tended to breathe more quickly and deeply once the face mask was applied and at times it was difficult to establish regular tidal breathing. This explained the slightly higher failure rate using the face mask. Overall, the child's preference did not influence the success rate or the reproducibility of the measurements. The children in this study were all >4 yrs; failure rates using a mouthpiece are highest in children <4 yrs 11, 12. Success rates may be improved by using a face mask in such children.
Although statistically significant, the mean differences between the two methods were small (7–10%). For a method with a CoV of 10–12% these differences may appear clinically insignificant, especially as the ICC (0.75) shows moderately good agreement between methods 22. However, the ICC result must be interpreted with caution as the 95% confidence limit of 0.43 is very low. This suggests that agreement between the methods may be very poor. This is supported by the wide limits of agreement which show that measurements using a mask can vary from 0.17 kPa·L−1·s below to 0.31 kPa·L−1·s above those using a mouthpiece. For a measurement with a range of 0.49–1.71 kPa·L−1·s this difference is unacceptable. The two methods cannot, therefore, be used interchangeably.
Previous studies have reported good success rates even with relatively inexperienced personnel 12 and this was confirmed in the present study. The present results are similar to those published both in terms of success 11, 12 and repeatability 6–8, 11–13, 15–16, 17, 26. Based on Shrout's 22 reliability standards, the ICCs obtained suggest that both methods were only moderately reliable 22. However, compared with specific airways resistance (sRaw), respiratory resistance and respiratory impedance measurements 5, 6, 27 in children of similar ages, the present study's CoVs were good. No evidence was found that children produced more reliable results with practice and it was confirmed that recording more than six Rint values makes little difference to the mean result 12. In this study, the coefficient of variation and the time taken were no better on the second occasion with either method.
The results from this study cannot be extrapolated to other face masks. Standard oronasal face masks, including those routinely supplied with the Micro Rint machine, do not allow any assessment to be made of the relative contributions from nose and mouth breathing 18. This is important because nose breathing has a major effect on total airways resistance 28. To overcome this problem, a modified face mask with an integral mouthpiece was used. This mask has been used previously to give reproducible Rint measurements with a plethysmograph 6, 19. In terms of patient comfort, this mask maintains all the benefits of a face mask but is really a specialized mouthpiece. Like the mouthpiece, it fails to support the floor of the mouth but ensures stable and reproducible mouth opening. It also provides firm support of the cheeks and prevents significant nose breathing 19.
The higher Rint values using the face mask may be explained by differences in the child's breathing pattern between the two methods or by the design of the face mask mouthpiece. Respiratory apparatus is known to influence breathing patterns with tidal volumes increasing more with a face mask than with a mouthpiece and noseclip 29. Although this was not formally measured in the present study, it was noted that children tended to breathe more deeply and rapidly through the face mask. This is likely to have increased the Rint values obtained. In terms of airways resistance, the major difference between the mouthpiece and the face mask was that the mask mouthpiece was slightly smaller in diameter than the standard mouthpiece (fig. 1⇑). It also contained a small ridge where it connected to the mask. The absolute size of the two mouthpieces is unlikely to have limited flow in the children studied but the ridge may have caused turbulence, reduced flow and, therefore, increased the Rint measurement. The mask may have provided better support of the upper airway than the mouthpiece. In this case, mask readings should have been less variable than mouthpiece readings. Incomplete nose-occlusion or a poor seal around the mask mouthpiece may also have contributed to the higher values using the face mask. This would tend to increase the variability of the mask readings relative to the mouthpiece. In this study, the CoVs between the two methods were not significantly different.
Conclusions
It is possible to measure airways resistance in young children using the interrupter technique in a nonspecialist setting. Reliable, repeatable measurements can be obtained quickly and easily using either a face mask or a mouthpiece. Children aged 4–7 yrs find both methods acceptable, but most prefer using a face mask. The results obtained are method-dependent and a face mask will tend to give higher values than a mouthpiece. Reference values should be interpreted with care as they are valid only for subjects using the same methodology. In order to ensure normal values are widely applicable, standardization of airway resistance measurements using the interrupter technique is necessary.
Acknowledgments
The authors would like to thank the parents, children, and teachers at The Marsh and St Wulstan's Primary Schools, Stoke-on-Trent for their help with this research.
- Received October 13, 2000.
- Accepted January 31, 2001.
- © ERS Journals Ltd
References









