





Abstract
The aim was to examine the relationship of serum inflammatory markers to the level of single-breath diffusing capacity of carbon monoxide (TL,CO).
A stratified sample (n=1,121) of a Norwegian general population aged 18–73 yrs was examined. The inflammatory markers measured were calprotectin, a prominent protein in the cytosol fraction of neutrophil granulocytes, and α1-antitrypsin (α1-AT), the major inhibitor of neutrophil elastase in the lower respiratory system. Both markers have increased circulating levels in the course of an acute inflammatory reaction.
Subjects with a TL,CO<80% of predicted value had a higher level of both α1-AT (p=0.003) and calprotectin (p<0.03) than those with a TL,CO>100%. In multiple linear regression analyses, α1-AT was still significantly associated with TL,CO after adjusting for sex, age, smoking habits, haemoglobin, carboxyhaemoglobin, forced expiratory volume in one second and alveolar volume. In a similar analysis, no significant overall association was found between calprotectin and TL,CO, but in a stratified analysis, calprotectin was significantly related to TL,CO in females. However, no significant sex interaction in the relationship between the inflammatory markers and TL,CO was found.
The findings suggest that increased levels of α1-antitrypsin and of calprotectin are risk factors for decreased diffusing capacity of carbon monoxide.
This study was supported by the Royal Norwegian Council for Scientific and Industrial Research, the Norwegian Research Council for Science and Humanities, and the Norwegian Asthma and Allergy Association.
Previous studies have shown a correlation between systemic inflammatory markers and decline in forced expiratory volume in one second (FEV1) 1, as well as increased bronchial reactivity 2. An inflammatory process may also affect the alveolar system in the lungs, but to date, only a few studies have shown a relationship between inflammatory markers in the blood and level of gas exchange in the lungs 3, 4.
Calprotectin is a prominent zinc and calcium binding protein in the cytosol fraction of neutrophil granulocytes 5. It can be used as a plasma marker for neutrophil activation/degranulation, and its level increases in plasma and in body fluids during infections or inflammatory conditions 5. Furthermore, increased concentration of this protein may reflect the elastase load on lung tissue to be balanced by α1-antitrypsin (α1-AT) 6.
α1-AT is regarded as the major guard against the neutrophil elastase in the lower respiratory system 7, 8, and this is clearly shown by the development of emphysema in severe α1-AT deficiency (Pi type ZZ or OO). It is also known that in α1-AT deficient patients, the single-breath diffusing capacity of carbon monoxide (TL,CO) can be extremely low 9. To the authors' knowledge, no community study has examined the association between TL,CO and α1-AT in blood in a general population. In the present study, the authors wanted to see if a reduction in TL,CO was associated or not with alterations in serum α1-AT or plasma calprotectin.
Methods
Study population
The study is a two-phased cross-sectional community survey. The methods of selection and the characteristics of the population have been given in detail previously 10, 11. A questionnaire was mailed to a random sample of 4,992 subjects of the general population, aged 15–70 yrs, and living in Hordaland county on the south west coast of Norway. The response rate was 90% (n=4,469).
Based on the information obtained from the postal survey, the respondents living in Bergen and 11 surrounding municipalities (n=3,370) were divided into two strata. The first stratum contained subjects who had received a physician's diagnosis of asthma and emphysema, subjects who had been occupationally exposed to asbestos or to quartz, and nonsmokers without respiratory symptoms. The second stratum contained those not included in the first 11. In the second phase of the survey, a 91% random sample of the subjects in stratum 1 and a 22% random sample of the subjects in stratum 2, altogether 1,512 subjects were invited to a standardized clinical examination. The overall attendance rate was 84% of those invited 11. The examination included completion of a questionnaire on respiratory symptoms, TL,CO and spirometric measurements, and a clinical examination.
Spirometric and diffusing capacity of carbon monoxide measurements
The equipment, as well as the standardized procedure, have been described in detail previously 12, 13. The TL,CO testing was done with a Gould 2100 automated system (Sensor Medics BV, Bilthoven, the Netherlands), using a gas mixture that contained 10% helium, 0.3% carbon monoxide, 21% oxygen, and a balance of nitrogen. The breath-holding time was preset to 10 s and the wash-out volume to 0.75 L. The dead space of the sample bag was 6.25 mL 12. Each subject's height was measured in stocking feet to the nearest cm. Weight was measured without shoes and with empty trouser-pockets. Before the test was performed, each subject was instructed in all the required manoeuvres. The test was performed in a sitting position wearing a noseclip. Each subject performed up to four measurements in order to provide two error free tests. A minimum of 4-min interval was required between each test. The Jones and Meade 14 method of determining the breath-holding time was used in this study.
Of the 1,275 subjects who performed the TL,CO test, data from 154 of them was excluded from further analysis for the following reasons: a leak in the sample bag occurring during the first 18 days of the study (n=108); subjects who were not able to hold their breath for 10 s in at least two TL,CO measurements (n=16); subjects not fulfilling the reproducibility criterion of two tests within 10% of each other (n=25); those performing unsatisfactory spirometric measurements (n=5). The reference equations for TL,CO used in this analysis were derived from a segment of healthy subjects who had never smoked, taken from a randomly selected population on the south-western coast of Norway, and were as follows 12: TL,CO (in mmol·min−1·kPa−1) in females:  in males:
in males:  Spirometry was performed on the Gould 2100 spirometer. The inspiratory and expiratory limbs of the spirometer were calibrated automatically with a 2.1-L motor driven syringe before each examination. The volume calibration was verified each day with a 3-L Gould Model M-20 calibrating syringe (Sensor Medics), with emptying times varying from 0.5–6 s 12. The variables recorded included forced vital capacity (FVC) and FEV1. Three technically satisfactory measurements were obtained in which FVC was reproducible within 300 mL. A technically satisfactory test met the lung function testing criteria of the European Coal and Steel Community 15.
Spirometry was performed on the Gould 2100 spirometer. The inspiratory and expiratory limbs of the spirometer were calibrated automatically with a 2.1-L motor driven syringe before each examination. The volume calibration was verified each day with a 3-L Gould Model M-20 calibrating syringe (Sensor Medics), with emptying times varying from 0.5–6 s 12. The variables recorded included forced vital capacity (FVC) and FEV1. Three technically satisfactory measurements were obtained in which FVC was reproducible within 300 mL. A technically satisfactory test met the lung function testing criteria of the European Coal and Steel Community 15.
The prevalence of bronchial asthma and chronic obstructive lung disease in this general population was 2.4% and 5.4%, respectively 11, while 29% of the subjects reported having been occupationally dust or gas exposed 11.
Blood samples
Prior to the diffusing capacity test, venous blood samples were drawn for determination of total haemoglobin (Hb) and carboxyhaemoglobin (HbCO) concentrations (OSM3 Hemoximeter, Radiometer, Copenhagen, Denmark). Analyses with this instrument are based on measurements of the transmission of light through the sample at six wavelengths.
Assessment of calprotectin in plasma
Ethylenediamine tetraacetic acid (EDTA)-plasma was tested in dilution 1:50 and 1:250 (if necessary) using a noncompetitive enzyme linked immunoassay 16, 17.
Briefly, samples and standards were incubated for 30 mins with shaking at ambient temperature in microtitre wells coated with the immunoglobulin-(Ig)G fraction of rabbit anticalprotectin. After washing, alkaline phosphatase labelled immunoaffinity purified rabbit anticalprotectin was added, followed by a second incubation. After a final wash, substrate was added and the colour read after ∼15 min. The coefficients of variation for this method are ∼5% within and 13% between assays.
Assessment of α1-antitrypsin in serum
The level of α1-AT was determined by rate nephelometry with the Behring Nephelometer Analyzer 18. The procedure supplied by the manufacturer was followed (Behring Nephelometer-System Folder) and specific kits were used for the assay of α1-AT. Testing the precision from day to day (n=21 days, four different serum pools) in the laboratory resulted in a coefficient of variation of 2.5%. In this study, samples were not analysed in duplicate. The analysis of calprotectin in plasma was performed within 48 h of the sample being taken. The analysis of α1-AT in serum was performed on the same day as the sample was taken.
Smoking status
According to their smoking habits, subjects were divided into three groups: nonsmokers, exsmokers, and current smokers. Nonsmokers were defined as subjects who stated that they had never smoked daily. Exsmokers were those who had smoked daily, but had given it up prior to the survey. Current smokers were those who smoked on average at least one cigarette daily at the time of the study.
Statistical methods
Descriptive statistics were computed separately for males and females (table 1⇓). The relationships between the two inflammatory markers and age, smoking habits, FEV1 and TL,CO in per cent predicted were considered first by univariate analysis (table 2⇓), and secondly by multivariate analysis (table 3⇓). Percentage predicted values for FEV1 and for TL,CO were calculated by using a prediction model based upon asymptomatic subjects who had never smoked 12, 19. Age, height, smoking status, FEV1, alveolar volume (VA), Hb and HbCO level in the blood, as well as serum α1-AT, and plasma calprotectin were included in a multiple linear regression model to determine their ability in predicting TL,CO. Smoking status was categorized according to the three groups mentioned earlier, and were analysed using the dummy variable technique. For analysing the relationship between the two inflammatory biomarkers and lung function, subjects were divided by tertiles according to their level of per cent predicted FEV1 and TL,CO (table 2⇓). All analyses were performed using the BMDP statistical software package (BMDP Statistical Software Inc., Los Angeles, CA, USA) 20.
Characteristics of the study population by sex (n=1121)
Levels of α1-antitrypsin and ln(calprotectin) by age, smoking habits, transfer factor of the lung for carbon monoxide (TL,CO) % pred, forced expiratory volume in one second FEV1 % pred in a Norwegian population (n=1121).
Multiple linear regression models for adjusted transfer factor of the lung for carbon monoxide (TL,CO) in males and females in a Norwegian population sample (n=1121)
Results
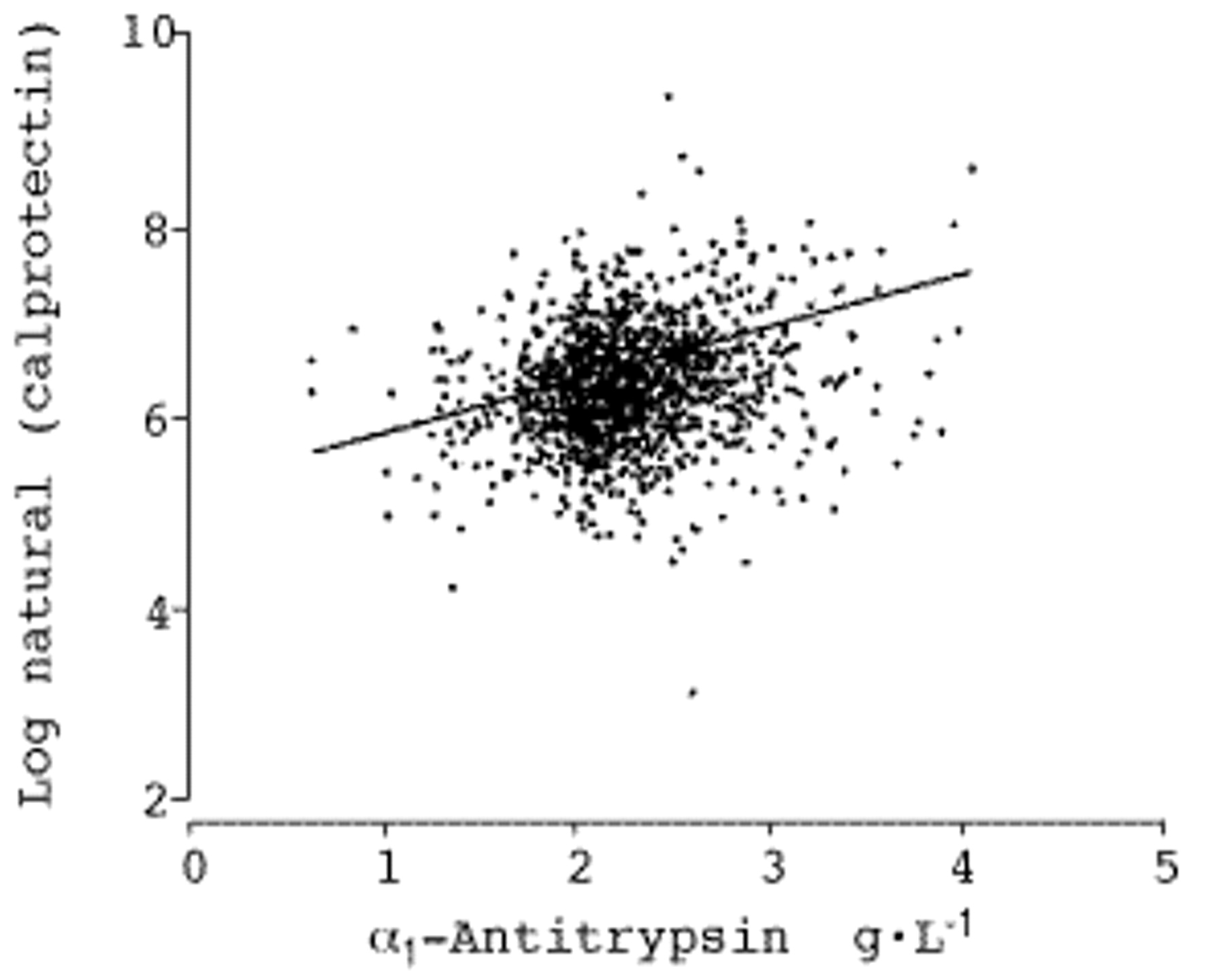
Characteristics of the study population are shown in table 1⇑. The distribution of serum α1-AT of the 1,121 subjects followed approximately a Gaussian curve. The concentrations were higher in females than in males (table 1⇑), higher in the older patients than in the younger age group and higher in current smokers than in nonsmokers or exsmokers (table 2⇑). Inversely, plasma calprotectin levels were higher in males than in females (table 1⇑). For further analyses, all calprotectin data were loge transformed to obtain normal distributions. Calprotectin levels were higher in the older subjects than in the younger age group, and did not vary significantly by smoking habits (table 2⇑). A significant but weak linear association (fig. 1⇓) was found between loge plasma calprotectin and serum α1-AT (correlation coefficient=0.22, p-value <0.001). The α1-AT level increased significantly with decreasing per cent predicted of FEV1 and decreasing per cent predicted of TL,CO (table 2⇑). Calprotectin showed an inverse borderline association in per cent predicted of TL,CO only. In a multiple linear regression analysis, α1-AT was significantly associated with TL,CO (regression coefficient=−0.25 mmol·min−1·kPa−1; p-value <0.001) after adjusting for sex, age, smoking habits, Hb, HbCO, FEV1 and VA. In a similar analysis using calprotectin instead of α1-AT as an explanatory factor, no significant association was found. When including both inflammatory markers in the model, α1-AT was still significantly associated with TL,CO (p-value=0.04). Neither VA nor FEV1 interacted on the relationship between α1-AT and TL,CO.
{kind=link}
Scatter plot of ln(calprotectin) against α1-antitrypsin in a Norwegian general population sample (n=1121). p<0.001, r=0.215.
The analysis above was then performed for males and females separately. In males, calprotectin was not associated with level of TL,CO, while a significant association was observed in females (table 3⇑). As for α1-AT, the association with TL,CO was significant only in females (table 3⇑). The relationship between TL,CO and the inflammatory markers was also assessed separately on the three smoking categories. No difference in this relationship was observed between the three groups.
When excluding subjects with bronchial asthma and chronic obstructive lung disease from the analysis (n=90), the relation between α1-AT and TL,CO remained significant (regression coefficient=−0.20; p-value=0.04).
Discussion
To the authors' knowledge, this is the first general population study to examine the relationship of inflammatory markers to level of TL,CO. Previous population surveys have been restricted to coal miners 4 or adults with pulmonary disease or other forms of poor health 3. It was observed that level of serum α1-AT was independently and inversely associated with level of TL,CO. The association tended to be stronger in females than in males and persisted after excluding subjects with obstructive lung disease. For calprotectin a borderline significance to TL,CO in females was found.
Methodological consideration
As it has been advocated recently 13, data was not excluded from the 32% of subjects who were not able to fulfill the criterion of an inspiratory vital capacity (IVC) superior or equal to 90% of their FVC at the TL,CO measurement. When the obtained IVC/FVC ratio was included in the analyses, no significant change was noted in the relationships between TL,CO and the inflammatory markers. Furthermore, adjusting for the stratified sampling did not modify the association between TL,CO and the inflammatory markers. It is worth noting that α1-AT deficiency is associated with emphysema which would lead to a reduced TL,CO. However, the present population did not contain subjects with α1-AT deficiency.
Discussion of main findings
The finding that calprotectin levels are higher in males than in females and that no significant difference was found between smokers and nonsmokers are in agreement with previous studies 21. As for α1-AT, a higher level in females than in males, as well as an increasing level by age, have previously been described in a general population in Norway 22 as well as in nonsmoking individuals with α1-deficiency in Sweden 23. The independent association between TL,CO and the two inflammatory markers may have several explanations. Firstly, elevated levels of α1-AT and calprotectin may reflect a prolonged or intermittent low grade inflammatory activity in the lung parenchyma, resulting in decrease in the diffusing capacity of the lung. The gas-transfer impairment may indicate the presence of early lung parenchymal damage, due to reduction of effective surface-for-gas exchange.
It has been postulated that progressive destruction of alveolar structures occurs because of an imbalance of the protease-antiprotease system at the alveolar level, and that α1-AT is the major anti-elastase 8, 24, 25. The quantity of α1-AT that diffuses passively from the blood to the lung increases during an acute inflammatory process 25, 26. This may indicate increased requirement of α1-AT to meet the needs of overcoming the release of various enzymes from neutrophilic cells 27 in the lung parenchyma, but its protective function may be overrun by the high concentration of proteinases 28.
Calprotectin is released by the activated neutrophil cell during an inflammatory process and its raise might be associated with any active lung disease where pulmonary inflammation is a feature 6. Neutrophils have been implicated in the pathogenesis of several lung diseases, including pulmonary emphysema 8. Recent studies indicate that neutrophil kinetics in the lungs are very different from those found in the microcirculation elsewhere 29. During the passage of blood through the lungs, activated leukocytes may be retained in the capillaries 30 and interact with the alveolar endothelium 31.
Secondly, the possibility of a pathological process originated in tissues remote from the lung and secondarily affecting the gas exchange in the lungs cannot be excluded. An immunological mechanism could lead to diffuse endothelial injury in the alveolar capillary bed. In such an instance, the decrease in TL,CO would be mainly related to a reduction in the transfer of gas to the alveoli due to loss of functional capillaries. In the acute phase, alveolar-capillary membrane thickening due to collagen and elastin alteration and oedema may affect the gas exchange. Circulating α1-AT and calprotection levels may be elevated in a variety of inflammatory conditions such as diseases of the gastrointestinal tract 16, 32, 33, inflammatory joint diseases 34, and bacterial infections 5, 35.
In a study aimed at investigating whether any pulmonary function testing abnormalities could be found in inflammatory bowel disease patients (n=132), a significant reduction in TL,CO was observed in 18% of the patients compared to none in the 36 healthy controls 36. More interestingly, as much as 88% of the subjects with the TL,CO abnormalities were in the active phase of the inflammatory bowel disease. Furthermore, activation of neutrophils is well documented in inflammatory bowel disease 37.
An inflammation of the lungs observed in a general population sample may theoretically be due to inhaled dust of both organic and inorganic origin as well as occupational and nonoccupational fumes and gases. However, the inflammatory marker-TL,CO association were not markedly changed when omitting subjects with occupational dust of gas exposure from the analyses. Conversely, this does not rule out airborne exposure as an explanatory variable as the exposure characterization in this community sample may not be precise enough.
It is worth noting that the inflammatory marker-TL,CO association persisted after excluding subjects with obstructive lung disease. Hence, the present finding was not driven by COPD subjects who may be characterized by impaired diffusion capacity and increased level of circulating inflammatory markers.
The finding that α1-AT and calprotectin are poorly correlated with each other (fig. 1⇑), and that both are independently associated with TL,CO, strengthens the theory that an ongoing systemic inflammation is linked to a decreased TL,CO. This also suggests that these parameters reflect separate aspects of the neutrophil-mediated inflammatory response. However, when assessing the associations of the inflammatory markers to level of TL,CO, it is important to note that the associations are weak, for instance when compared to that of smoking to TL,CO. Both the inflammatory markers and the TL,CO were measured at a single point of time. Hence, this cross-sectional study cannot provide data as to what extent the levels of the inflammatory markers and TL,CO may covariate over time. To answer this, a longitudinal study design is necessary.
Compared to males, females had larger coefficients for the relationships between inflammatory markers and TL,CO. It has been shown that a given immune response is affected by the level and nature of circulating steroid sex hormones 38. As a consequence, this may also result in subtle sex differences in triggering an inflammatory process. However, the interpretation should be cautious as no significant interaction by sex in the inflammatory markers-TL,CO relationships were observed. No previous study has examined any sex-effect on this relationship.
Conclusion
In conclusion, the present study showed that in a general population sample aged 18–73 yrs, an increase in levels of calprotectin and of α1-AT was associated with a decrease in TL,CO. The present findings raise the possibility that an ongoing inflammatory process, initiated either in the lung or elsewhere, results in injury in the alveolar space.
In the future, long-term studies are needed to confirm that subjects with an ongoing systemic inflammation over a given period are at risk of developing pulmonary dysfunction. The cumulative effect of repeated episodes of inflammation may account for the gas diffusion impairment, and may contribute to respiratory symptoms only after a long period of time.
- Received July 26, 2000.
- Accepted January 18, 2001.
- © ERS Journals Ltd
References









